I am a pediatric gastroenterologist at GI Care for Kids (previously called CCDHC) in Atlanta, Georgia. The goal of my blog is to share some of my reading in my field more broadly. In addition, I wanted to provide my voice to a wide range of topics that often have inaccurate or incomplete information.
Before starting this blog in 2011, I would tear out articles from journals and/or keep notes in a palm pilot. This blog helps provide an updated source of information that is easy to access and search, along with links to useful multimedia sources.
I was born and raised in Chattanooga. After graduating from the University of Virginia, I attended Baylor College of Medicine. I completed residency and fellowship training at the University of Cincinnati at the Children’s Hospital Medical Center. I received funding from the National Institutes of Health for molecular biology research of the gastrointestinal tract.
During my fellowship, I had the opportunity to work with some of the most amazing pediatric gastroenterologists and mentors. Some of these individuals included Mitchell Cohen, William Balistreri, James Heubi, Jorge Bezerra, Colin Rudolph, John Bucuvalas, and Michael Farrell. I am grateful for their teaching and their friendship. During my training with their help, I received a nationwide award for the best research by a GI fellow.
I have authored numerous publications/presentations including original research, case reports, review articles, and textbook chapters on various pediatric gastrointestinal problems. In addition, I have been recognized by Atlanta Magazine as a "Top Doctor" in my field multiple times.
Currently, I am the vice chair of the section of nutrition for the Georgia Chapter of the American Academy of Pediatrics. In addition, I am an adjunct Associate Clinical Professor of Pediatrics at Emory University School of Medicine. Other society memberships have included the North American Society for Pediatric Gastroenterology Hepatology and Nutrition (NASPGHAN), American Academy of Pediatrics, the Food Allergy Network, the American Gastroenterology Association, the American Association for the Study of Liver Diseases, and the Crohn’s and Colitis Foundation.
As part of a national pediatric GI organization called NASPGHAN (and its affiliated website GIKids), I have helped develop educational materials on a wide-range of gastrointestinal and liver diseases which are used across the country. Also, I have been an invited speaker for national campaigns to improve the evaluation and treatment of gastroesophageal reflux disease, celiac disease, eosinophilic esophagitis, hepatitis C, and inflammatory bowel disease (IBD). Some information on these topics has been posted at my work website, www.gicareforkids.com, which has links to multiple other useful resources.
I am fortunate to work at GI Care For Kids. Our group has 17 terrific physicians with a wide range of subspecialization, including liver diseases, feeding disorders, eosinophilic diseases, inflammatory bowel disease, cystic fibrosis, DiGeorge/22q, celiac disease, and motility disorders. Many of our physicians are recognized nationally for their achievements. Our group of physicians have worked closely together for many years. None of the physicians in our group have ever left to join other groups. I have also worked with the same nurse (Bernadette) since I moved to Atlanta in 1997.
For many families, more practical matters about our office include the following:
– 14 office/satellite locations
– physicians who speak Spanish
– cutting edge research
– on-site nutritionists
– on-site psychology support for abdominal pain and feeding disorders
– participation in ImproveCareNow to better the outcomes for children with inflammatory bowel disease
– office endoscopy suite (lower costs and easier scheduling)
– office infusion center (lower costs and easier for families)
– easy access to nursing advice (each physician has at least one nurse)
I am married and have two sons (both adults). I like to read, walk/hike, bike, swim, and play tennis with my free time.
I do not have any financial relationships with pharmaceutical companies or other financial relationships to disclose. I have helped enroll patients in industry-sponsored research studies.
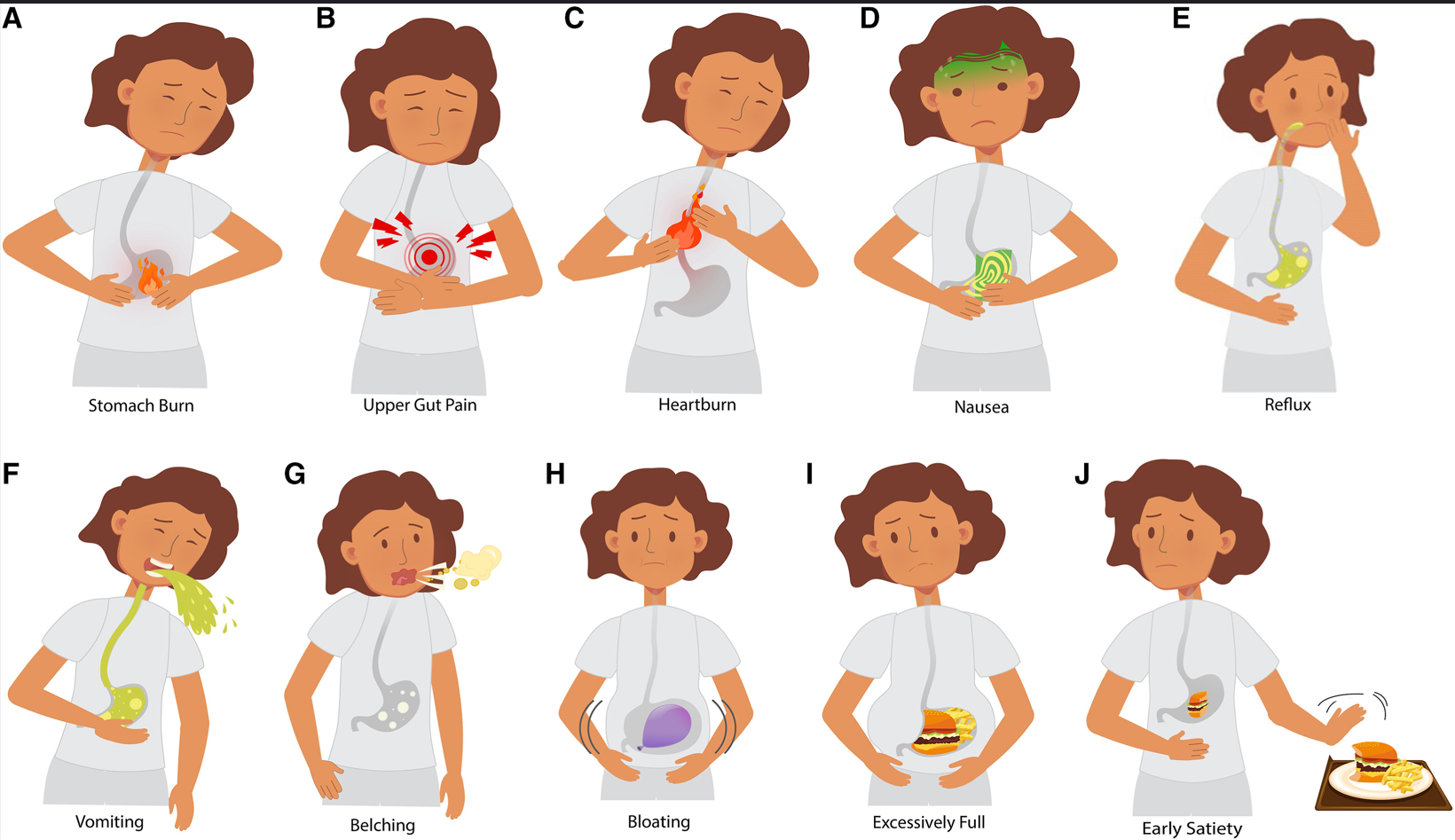
The authors attempted to develop useful pictograms to help enable standardization of symptom reporting in children with gastroduodenal disorders.
Figure 2: Pediatric gastroduodenal symptom pictograms. A, stomach burn; B, upper gut pain; C, heartburn; D, nausea; E, reflux; F, vomiting; G, belching; H, bloating; I, excessively full; and J, early satiety. (The same images were used to create the animated set).
Key findings:
Face and content validity were higher for the pediatric static and animated pictogram sets compared with pre-existing adult pictograms (78% vs 78% vs 61%).
Participants with worse gastric symptoms had superior comprehension of the pediatric pictograms (χ2 [8, N = 118] P < .001)
“Little significant comprehension was gained by having the animated pictograms.”
My take: Some research while worthwhile does not pan out. This is what I was thinking when I read this study. Upper GI symptoms are difficult to convey in pictures; in addition, some patients will have multiple overlapping symptoms. This is why the validity percentages are not higher. I don’t foresee using these pictograms in clinical practice.
This was a multicenter retrospective cohort study of adults with ulcerative colitis comparing upadacitinib (n=70) to ustekinumab (n=148). The upadacitinib-treated patients were all bio-exposed, had more advanced therapy failures, and higher baseline SCCAI (simple clinical colitis activity index).
Key findings:
Upadacitinib-treated patients had better outcomes: Clinical response of 82.9% vs. 63.5%, Steroid-free clinical remission 62.1 % vs. 34.7%, improvement in arthralgia 64.3% (9 of 14) vs 23.4% (11 of 47), and endoscopic remission 37.5% (9 of 24) compared with 15.9% (7 of 44).
The odds ratio (OR) after inverse probability of treatment-weighting were in favor of upadacitinib: Clinical response OR 2.39, SFCR OR 3.17, and endoscopic remission OR 5.10
Similar amounts of adverse effects were reported in each group
My take: Upadacitinib had better response rates within 52 weeks even though the patients receiving this medication had more advanced therapy failures. However, it is important to keep in mind the limitations of this retrospective study. The improved outcomes are in contrast to a study comparing another JAK inhibitor (tofacitinib) to ustekinumab in which the outcomes appeared equivalent (Tofacitinib vs Ustekinumab -Which is Better for Ulcerative Colitis?).
This article provides guidance on what is mild Crohn’s disease (CD) and suggested management. The authors note that there are limited randomized controlled trial data focusing on patients with mild CD.
Key points:
“Maintenance strategies often fall under the realm of supportive care. Therapeutic approaches need to factor clinical effectiveness, prevention of disease-related complications, risks of adverse events resulting from undertreatment or overtreatment and costs of care.”
For induction, the authors suggest budesonide 9 mg per day for 8 weeks with tapering, a tapering course of prednisone or sulfasalazine for colonic CD
In those with response to induction, the authors recommend supportive care including anti-diarrheal agents and dietary modifications. Ongoing monitoring is suggested including clinical symptoms and objective labs/biomarkers (every 12 weeks if CD activity and every year during remission)
In those without response or early relapse, the authors advocate for further evaluation for disease activity and alternative etiologies along with consideration of advanced therapies (f objective evidence of persistent activity)
“Accumulating evidence supports diets rich in fruits and vegetables with limited intake of foodstuffs containing saturated fats, ultraprocessed foods, artificial sweeteners, and emulsifiers.”
Advanced therapies “such as vedolizumab, ustekinumab, and risankizumab may be considered owing to favorable effectiveness and safety profiles…may be too cost-prohibitive to justify use for mild CD.”
My take: As younger patients are at increased risk for disease progression, the approach recommended in this article would have very limited application in the pediatric age group.
D Hemenway. NEJM 2024; 390:1352-1353 Twenty-Five Years after Columbine — Firearms and Public Health in the United States
This commentary notes that in the aftermath of Columbine, Smith and Weston had agreed “to upgrade its products and practices to help reduce the harms caused by its guns. Since a common cause of unintentional shootings is incorrectly believing that the gun is unloaded, its pistols would have chamber load indicators, and magazine disconnects would be available. The company would provide “ballistic fingerprints” on new firearms to help law-enforcement agencies trace guns. It would sell its guns only to dealers who had a plan for preventing gun theft and — to reduce gun trafficking — would agree to limit multiple-handgun sales to any individual buyer. The dealers would also have to agree not to sell large-capacity magazines.1 But the firearms industry immediately began boycotting the company, and its chief executive officer was forced to retire.”
This article offers the following advice to reduce firearm mortality, the number one killer of children:
“The Surgeon General could provide biannual reports on guns and suicide; the federal government could both conduct and fund research into smart guns and safer means of home protection than owning a handgun”
“Police could have social workers embedded in precincts”
“The faith community could make it clear that it is a cardinal sin to sell a gun to a stranger without a background check”
“Probably the most important thing our country can do is to elect more officials who will help make changes where the effect will be greatest — in the gun industry and the gun culture”
“To achieve a huge reduction in gun deaths will probably require mandating what is common for car drivers in the United States and for gun owners in other high-income countries: gun licensing, gun training, and handgun registration, along with universal background checks. These requirements are supported by most Americans”
“PLCAA (Protection of Lawful Commerce in Arms Act) protections should be eliminated, and the gun industry treated like other industries”
“And just as car manufacturers had to be forced to put seat belts, airbags, collapsible steering columns, and safety glass into their vehicles, the gun industry should be forced to take the types of steps that Smith and Wesson was willing to take 25 years ago”
No Exaggeration: Too Many Children Are Dying in the U.S. “The sad fact is that a child or adolescent in the United States is 57% more likely to die by the age of 19 years than those in other wealthy nations.” This is due mainly to more deaths from MVAs and from gun violence.
A recent blog post (Is Medicine a “Calling?”) reviewed a commentary about whether physicians have become ‘cogs of capitalism’ leading to dissatisfaction.
A recent response letter (RL Albin. N Engl J Med. 2024 Apr 18;390(15):1444. doi: 10.1056/NEJMc2403045) offered some useful insights:
Before WWII, physicians were paid directly by patients. Afterwards, “taxpayer-subsidized, employment-based health care and social insurance guaranteed healthy incomes. Generous subsidies for higher education lowered barriers to professional entry…”
Due to “clever political lobbying, physicians enjoyed these considerable subsidies without major sacrifices of sovereignty.2 This system was economically unsustainable…”
“Physician lobbying played a sizable role in defeating efforts toward rational public control, unwittingly advancing corporatization with its gross inefficiency, multiple inequities, and erosion of physician sovereignty. Physicians are “cogs of capitalism,” but we continue to be well-paid, respected professionals. The real victims are the many Americans who lack access to decent health care”
A related article: K Schulman, B Richman. NEJM 2024; 390: 1445-1447. Hospital Consolidation and Physician Unionization. This article describes the increase in physician unionization that is taking place and makes the following points:
“Since the 1990s, hospitals have been consolidating to form health systems that now exert monopolistic leverage in many health care markets in the United States”
“In 2012, only 5.6% of U.S. physicians were directly employed by a hospital,1 and another 23% were in a practice that was at least partially owned by a hospital…By January 2022, the proportion of hospital-employed physicians had risen to 52%, with another 22% of physicians being employed by other corporate entities”
[Unionization] “is a natural consequence of hospital consolidation and the corporatization of health care delivery… Executives may also consider physicians to be largely interchangeable…Amid shifts in practice structures, physicians may experience a deterioration in their working conditions, job satisfaction, and — most important — involvement in the governance of health care delivery”
[Unionization provides] “the opportunity to negotiate over wages with monopolists…Unions often express workers’ concerns about non–wage-related matters, including issues affecting job satisfaction, professional meaning, and workplace conditions”
“Physicians supporting these drives have emphasized concerns about staffing, burnout, and the quality of patient care as motivations for unionization. Collective bargaining has been a direct response to the most negative consequences of hospital consolidation”
My take: Doctoring can be sacred work. While physicians need to work to improve workplace environments and enhance personal interactions with patients, it is sobering to realize that many patients have been harmed much more than physicians with the changes in healthcare delivery and costs.
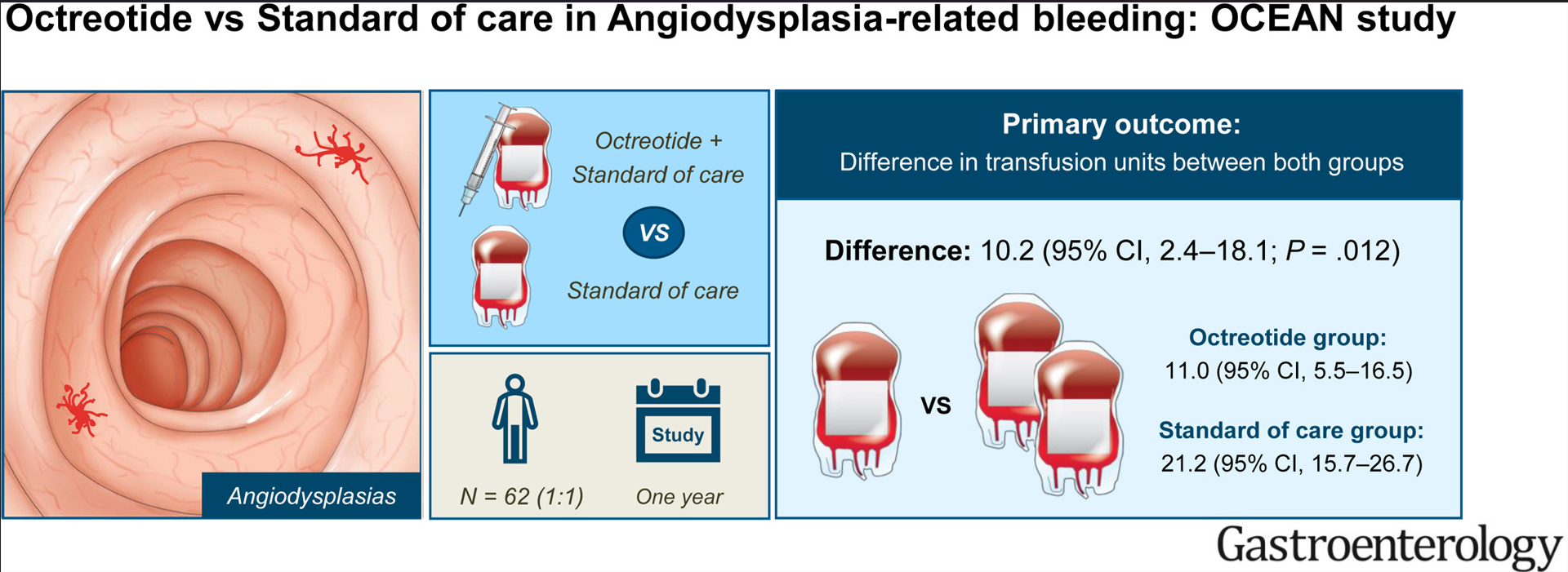
Methods: The study was designed as a multicenter, open-label, randomized controlled trial. Patients with angiodysplasia bleeding were required to have had at least 4 red blood cell (RBC) units or parental iron infusions, or both, in the year preceding randomization. Patients were allocated (1:1) to 40-mg octreotide long-acting release intramuscular every 28 days or standard of care, including endoscopic therapy.
Key findings:
Baseline: Patients (n=62, with mean age 72 years) required a mean number of 20.3 transfusion units and 2.4 endoscopic procedures in the year before enrollment.
During Study: The total number of transfusions was lower with octreotide (11.0) compared with standard of care (21.2). Octreotide reduced the annual volume of endoscopic procedures by 0.9.
Adverse events: Octreotide-related AEs were common (65%);however, these AEs were mild and self-limiting nature. They “rarely elicit treatment discontinuation.”
mean number of transfusion units patients in the octreotide group and standard of care group
My take: Fortunately (for me), angiodysplasia is quite rare in the pediatric age group. In adults, octreotide helps reduce transfusions and need for endoscopy.
This “retrospective cohort study was conducted using data acquired from SPARC IBD, a component of the Crohn’s & Colitis Foundation’s IBD Plexus research platform. SPARC IBD is a prospective cohort study conducted at 18 US centers and includes more than 4000 patients.” The median patient age was 37 years.
Key findings:
Following an initial negative result in 687 patients, 269 patients received a second test (after an initial negative test), of which 5 were positive (1.9%), which was not significantly different from the prevalence with the first test
Oral steroids were associated with an increased proportion of indeterminate results, although not achieving statistical significance
The authors did not identify any potential risk factors for latent tuberculosis among the covariates investigated
Overall, the authors found “found that there is continued utility for the use of IGRA tests with patients receiving medication for IBD despite the declining incidence of tuberculosis in the United States. In addition to testing before administration of treatment, this study suggests serial testing may still be necessary because of a substantial rate of positive conversions among patients in the cohort.”
After reading this study, I did an informal survey from the physicians/APP in my group. As a group, we take care of approximately 1000 children with inflammatory bowel disease. Over the last 20 years, only one of my partners recollects having a true positive test result after an initial negative result. This particular patient who was asymptomatic received a 9 month course of isoniazid.
My take: There is a low yield of follow-up testing for tuberculosis, especially in pediatric patients with no exposure history or travel history. For our practice, this would be a good summer research project for a premed student, a resident or even a fellow. I would expect the yearly and cumulative costs of screening for latent tuberculosis in our practice to be quite high. A quick web search suggests that a single blood test costs ~$150 which would be $105,000 for 700 tests. However, the costs are much greater due to additional investigations related to indeterminate results.
Corporations are supposed to pay a nominal tax rate of 21%. But in recent years, the biggest pharmaceutical companies had an average effective tax rate of less than 12%, according to an analysis by the Senate Finance Committee….
An NPR examination of financial records for the top five drug companies in the U.S. showed that in 2023, all but Eli LIlly reported losing money in the US.
However, drug companies make most of their sales in the U.S., thanks in large part to its unique health care system and the higher prices Americans pay for drugs. The top five American pharmaceutical companies all had more drug sales in the U.S. than they did in all the other countries in the world put together…
“How do they do it? You license your intellectual property to an offshore subsidiary,” Setser tells NPR. “You produce the high value-added active ingredients in a factory in Ireland or Singapore, and you pretend like the profit is accrued to these offshore subsidiaries, even though the sales are back to the United States…”
The drug industry isn’t the only one that moves its income around to pay lower taxes, but the U.S. market’s role in driving the drug industry’s overall revenue makes the tax strategy stand out, says Ameet Sarpatwari, assistant director of the Program on Regulation, Therapeutics and Law at Harvard Medical School.
“These findings are striking because they show that the companies want to benefit from the high prices and the high sales in the U.S. market, but are doing everything possible to not contribute to the taxes that make that system and market function”
My take: Despite earning top dollar and receiving all sorts of research support, the pharmaceutical industry (like other industries) are taking advantage of US tax laws and not paying their fair share. Yet, I doubt there will be legislation passed in the near future to address this. “The pharmaceutical and health product industry spent $381 million lobbying Congress in 2023 – more than any other industry that year”.
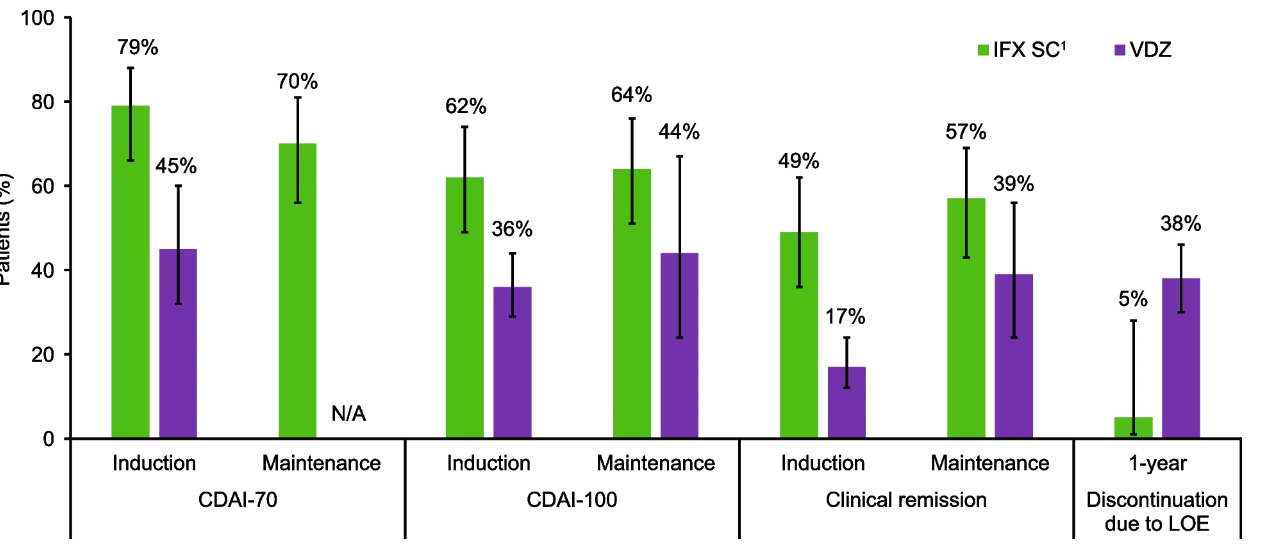
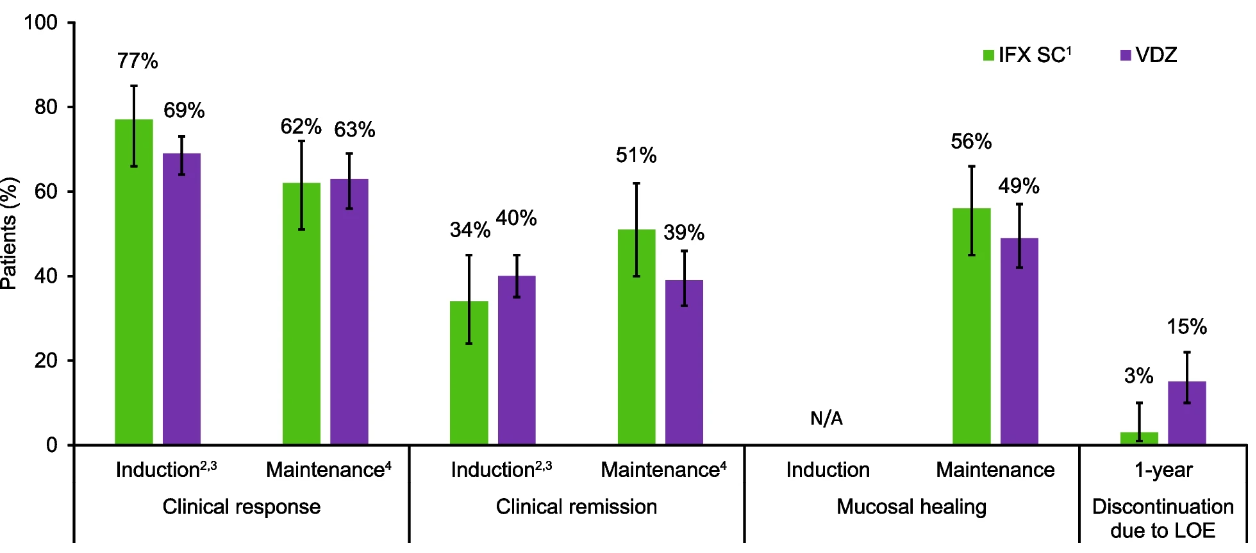
Methods: Studies included in the current analysis were parallel-group, randomised controlled trials (RCTs) that evaluated treatment with IFX SC, following induction therapy with IFX IV, or treatment with VDZ (either with VDZ IV or with VDZ SC [following IV induction therapy]). The authors identified three eligible CD trials and four eligible UC trials that assigned over 1200 participants per disease cohort to either IFX SC or VDZ.
Key findings:
Crohn’s disease: Intravenous induction therapy with IFX demonstrated better efficacy compared with VDZ; during the maintenance phase, IFX SC showed numerically better efficacy than VDZ. A lower proportion of IFX SC-treated patients discontinued therapy due to lack of efficacy over 1 year.
Comparison of IFX SC versus VDZ for key efficacy outcomes in patients with Crohn’s disease
Ulcerative colitis: Efficacy profiles were similar with IFX SC and VDZ during the induction and maintenance phases, and a lower proportion of IFX SC-treated patients discontinued therapy due to lack of efficacy over 1 year.
Comparison of IFX SC1versus VDZ for key efficacy outcomes in patients with ulcerative colitis
Safety: In both cohorts, safety profiles for IFX SC and VDZ were generally comparable during 1 year.
Discussion Points:
The authors discuss some limitations of their study. “The GEMINI I, GEMINI II, and VISIBLE 1 trials were rated as being at high risk of bias for the category ‘other’ bias, because only patients who achieved a clinical response during induction went on to participate in the maintenance phase, which could potentially lead to a higher estimate of efficacy during the maintenance phase than if patients who did not achieve a clinical response were also included.”
The vedolizumab studies notably included a high proportion of patients who failed to respond to anti-TNFs. “All VDZ studies permitted enrolment of patients with prior TNFi failure, accounting for 47.5% of VDZ-treated patients overall.” Thus, in a true head-to-head study with patients unexposed to biologics, VDZ may achieve better results.
My take: This study indicates that SC infliximab (like IV infliximab) appears to be more effective than vedolizumab for patients with Crohn’s disease and similarly effective for ulcerative colitis, keeping in mind the aforementioned discussion points. While not evident in this study, vedolizumab has a superior safety profile.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Personal pet peeve: I receive so many unwanted promotional materials from pediatric hospitals and pediatric gastroenterology divisions from across the country. This is such a waste of paper and effort. Presumably, this is an endeavor to raise the profile of these institutions and programs.
If anyone reading this blog has any role in this, please stop sending this crap and only send this material to alumni or those that request (opt-in) it.