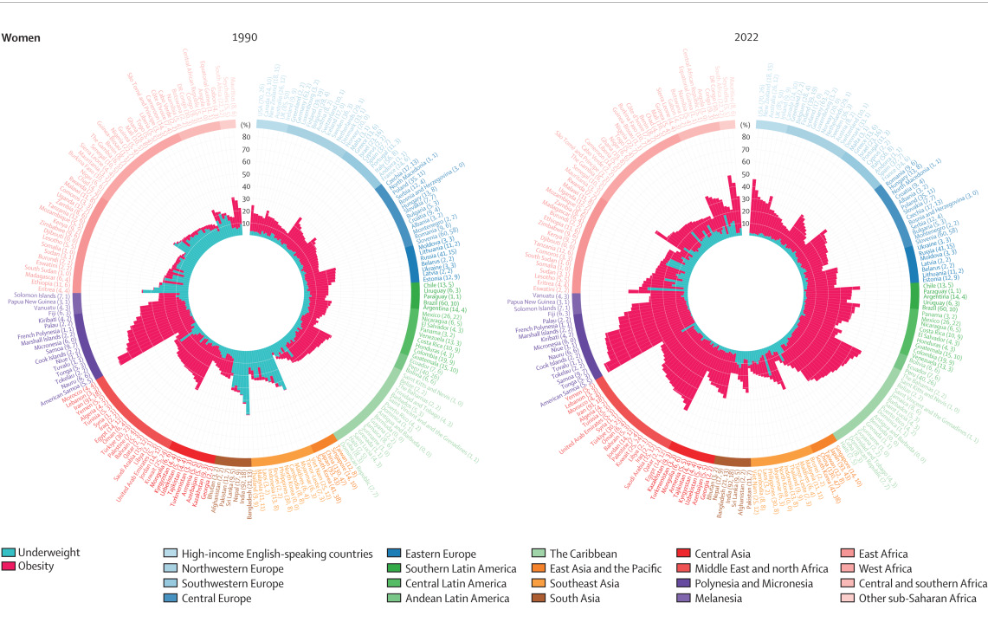
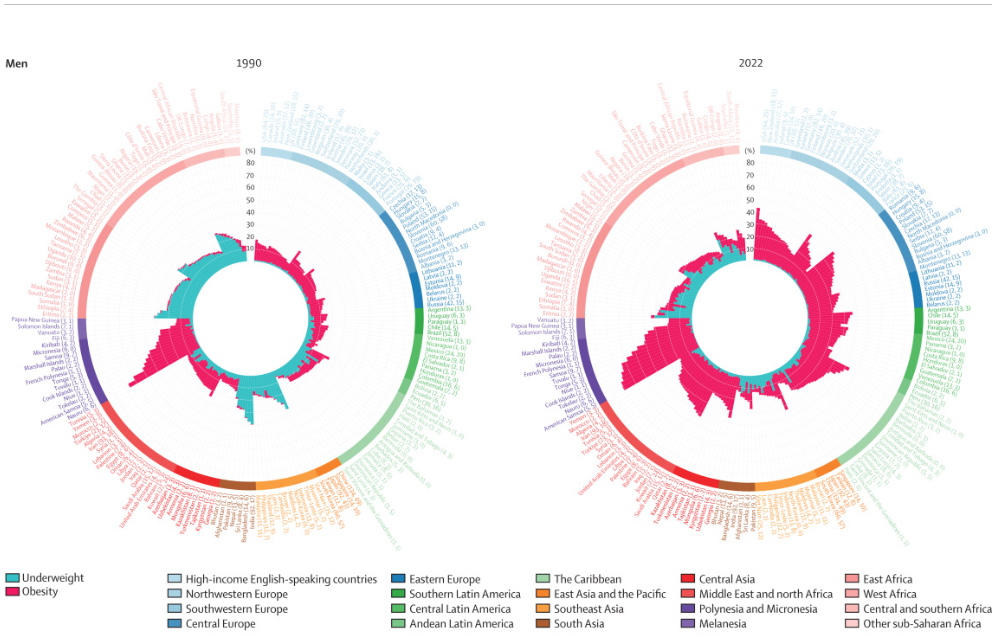
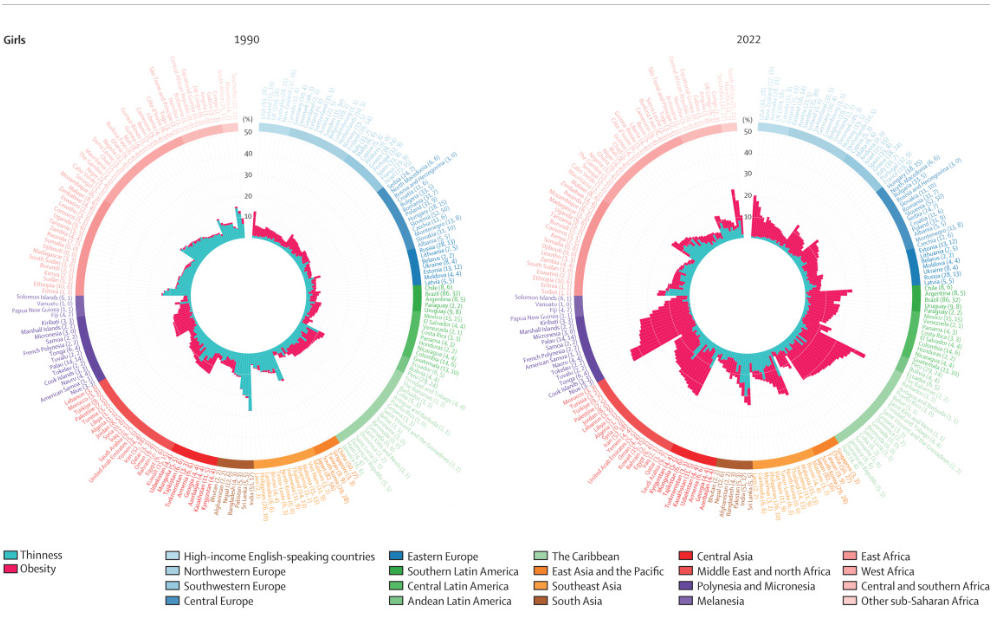
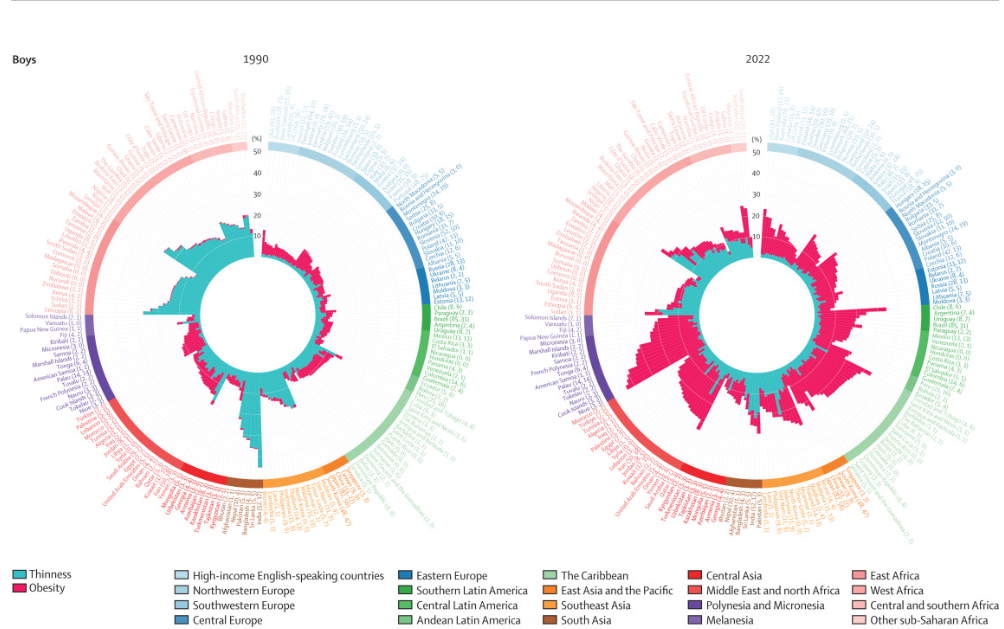
NCD Risk Factor Collaboration. The Lancet 2024; DOI:https://doi.org/10.1016/S0140-6736(23)02750-2 Open Access! Worldwide trends in underweight and obesity from 1990 to 2022: a pooled analysis of 3663 population-representative studies with 222 million children, adolescents, and adults
The authors used data from 3663 population-based studies with 222 million participants that measured height and weight in representative samples of the general population.
Key findings:
- More than a billion people globally are now considered obese.
- Obesity has more than quadrupled among children and adolescents since 1990.
- Among all adults, 43 percent were overweight in 2022.
- The combined burden of underweight and obesity has increased in most countries, driven by an increase in obesity, while underweight and thinness remain prevalent in south Asia and parts of Africa.
- The trend of increasing obesity prevalence was present in adults and children (5-19 years).
- Age-standardized prevalence of obesity increased by more than 20 percentage points in 49 countries (25%) for women and 24 countries (12%) for men, and by as much as 33·0 percentage points in The Bahamas for women and 31·7 percentage points in Romania for men.
My take: This is an impressive study providing extensive data on what’s happening with weight trends. Clearly, there is an urgent need for obesity prevention.
Related blog posts:
- “The Paramount Health Challenge for Humans in the 21st Century”
- Primary Prevention of Obesity Still Needed
- Childhood Obesity and Consensus Recommendations
- Nutritional Risks in Adolescents After Bariatric Surgery; Prevention of Childhood Obesity; Convalescent Serum for COVID-19
- How Often Do Children with Obesity Have a Fatty Liver?
- NY Times: “Our Food is Killing Too Many of Us”
- Skipping breakfast –boomerang effect for obesity | gutsandgrowth
- Eliminating sweetened beverages to help obesity | gutsandgrowth
- A liver disease tsunami | gutsandgrowth
- Six years later-Mediterranean diet comes out on top | gutsandgrowth
- Psychology of obesity and food addiction | gutsandgrowth
- Six year outcomes with bariatric surgery | gutsandgrowth
Humor from The Onion: