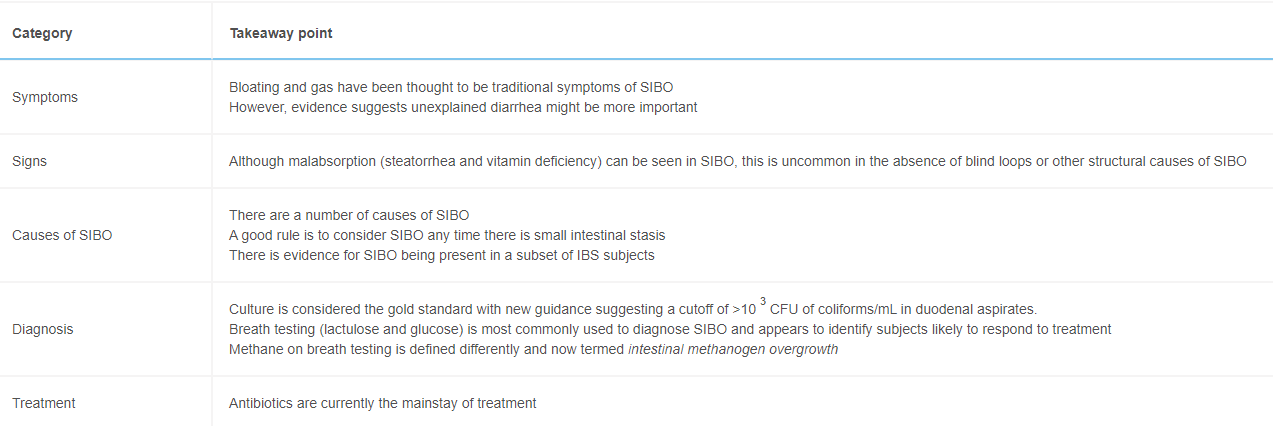
This is a really lousy clinical practice guideline but a pretty good review of small intestinal bacterial overgrowth (SIBO). The reason why it is lousy: it provides virtually no recommendations on how to define/diagnose SIBO, does not recommend specific testing and equivocates on specific treatments.
Here are a few of the “best practice advice” as examples:
#1 The definition of SIBO as a clinical entity lacks precision and consistency; it is a term generally applied to a clinical disorder where symptoms, clinical signs, and/or laboratory abnormalities are attributed to changes in the numbers of bacteria or in the composition of the bacterial population in the small intestine
#5 A major impediment to our ability to accurately define SIBO is our limited understanding of normal small intestinal microbial populations
#6 Controversy remains concerning the role of SIBO in the pathogenesis of common functional symptoms, such as those regarded as components of irritable bowel syndrome
#9 There is a limited database to guide the clinician in developing antibiotic strategies for SIBO
While not providing ‘best practical advice,’ the article does provide details regarding limitations in testing, underlying pathogenesis, and potential treatment regimens for adults.
A recent correspondence letter (CJ Black, AC Ford. AJG 2020; doi: 10.14309/ajg.0000000000000932. Full text: Efficacy of Ondansetron for Irritable Bowel Syndrome With Diarrhea) shows that ondansetron could be an effective option for irritable bowel syndrome with diarrhea. Thanks to Ben Gold for this reference.
“We found histologic evidence of UC activity (Geboes score ≥ 2B.1) in biopsies from 182 patients (65%) and endoscopic evidence of UC activity in 149 patients (53%) (substantial agreement, κ = 0.60).”
“Histologic features of UC activity were associated with increased rates of systemic corticosteroid use, colectomy, and hospitalization in the entire cohort (P < .05 for all) and associated with increased rates of systemic corticosteroid use in an analysis limited to patients in endoscopic remission (P < .001).”
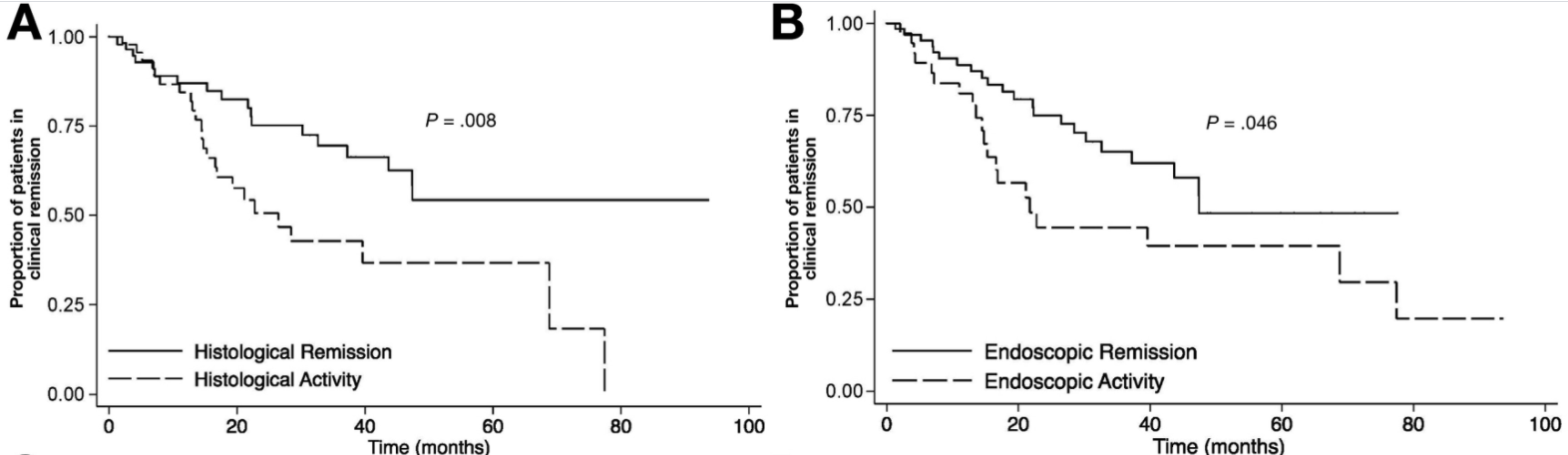
At ileo-colonoscopy, 63% of patients had endoscopic healing and 55% had histologic evidence of healing. The level of agreement between endoscopic and histologic activity was fair (62%, K = 0.2250, P = .0064)
On multivariate analysis, only histologic healing was associated with decreased risk of clinical relapse (hazard ratio [HR], 2.05; 95% CI, 1.07–3.94; P = .031), medication escalation (HR, 2.17; 95% CI, 1.2–3.96; P = .011), and corticosteroid use (HR, 2.44; 95% CI, 1.17–5.09; P = .018).
Kaplan-Meier analysis of effect of endoscopic and histologic activity on (A) clinical relapse-free survival versus histologic healing, (B) clinical relapse-free survival versus endoscopic healing
D Kevans et al. Inflamm Bowel Dis 2020; 26: 1722-1729. Histological Markers of Clinical Relapse in Endoscopically Quiescent Ulcerative Colitis Key finding: In endoscopically quiescent UC (n=76), active histological inflammation …[is] adjunctive histological marker associated with increased likelihood of disease relapse. The associated editorial (1730-32 by Asher Kornbluth) quotes Voltaire: “A wise Italian says that the best is the enemy of the good.” He notes that there is “a very real risk of abandoning an effective drug while chasing the goal of some yet to be universally defined histologic remission.” Currently organizational guidelines (ACG, AGA, ECCO, IOIBD) do NOT suggest the use of histologic normalization as an endpoint at this point.
My take: These studies show that histologic healing in ileal Crohn’s disease and in ulcerative colitis are associated with better outcomes that endoscopic appearance. However, there are a lot questions because many patients, possibly a majority, will not achieve histologic healing despite aggressive treatment. Related technical issues include how many biopsies are needed to assess histology and having a validated histologic assessment.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Background: AK002 (lirentelimab) is an anti-Siglec-8 antibody that depletes eosinophils and inhibits mast cells.
Methods: In this phase 2 trial, the authors randomly assigned adults (n=65) who had symptomatic eosinophilic gastritis, eosinophilic duodenitis, or both conditions in a 1:1:1 ratio to receive four monthly infusions of low-dose AK002, high-dose AK002, or placebo
Key findings:
The mean percentage change in gastrointestinal eosinophil count was −86% in the combined AK002 group, as compared with 9% in the placebo group
Treatment response (>30% reduction in total symptom score and >75% reduction in gastrointestinal eosinophil count) occurred in 63% of the patients who received AK002 and in 5% of the patients who received placebo
The authors note that AK002 “also resulted in alleviation of dysphagia in patients with a history of concomitant eosinophilic esophagitis.”
Limitations: Small study and 10% developed antibodies to drug
My take: Larger phase 3 studies with AK002 are underway (NCT04322604 & NCT04322708). AK002 looks promising for eosinophilic gastrointestinal diseases.
Change in total symptom score over 14 weeks. “Shown is the least-squares mean percentage change from baseline in total symptom score over time.” The total symptom score ranges from 0 to 80, with higher scores indicating greater symptom severity. Each of eight symptoms are given a score of 0 to 10: abdominal pain, nausea, vomiting, early satiety, loss of appetite, abdominal cramping, bloating and diarrhea.
Listed below are the 10 ‘Best Practice Advice’ recommendations. I think the acknowledgement that “hemostatic powder should be preferentially used as a rescue therapy and not for primary hemostasis, except in cases of malignant bleeding or massive bleeding with inability to perform thermal therapy or hemoclip placement” (#7) is very useful.
“Best Practice Advice:”
Endoscopic therapy should achieve hemostasis in the majority of patients with NVUGIB.
This may include clips, thermal (heater probes, bipolar/multipolar catheters, hemostatic forceps), diluted epinephrine injection, and hemostatic spray
Initial management of the patient with NVUGIB should focus on resuscitation, triage, and preparation for upper endoscopy. After stabilization, patients with NVUGIB should undergo endoscopy with endoscopic treatment of sites with active bleeding or high-risk stigmata for rebleeding.
Endoscopists should be familiar with the indications, efficacy, and limitations of currently available tools and techniques for endoscopic hemostasis, and be comfortable applying conventional thermal therapy and placing hemoclips.
Monopolar hemostatic forceps with low-voltage coagulation can be an effective alternative to other mechanical and thermal treatments for NVUGIB, particularly for ulcers in difficult locations or those with a rigid and fibrotic base.
Hemostasis using an over-the-scope clip should be considered in select patients with NVUGIB, in whom conventional electrosurgical coagulation and hemostatic clips are unsuccessful or predicted to be ineffective.
Hemostatic powders are a noncontact endoscopic option that may be considered in cases of massive bleeding with poor visualization, for salvage therapy, and for diffuse bleeding from malignancy.
Hemostatic powder should be preferentially used as a rescue therapy and not for primary hemostasis, except in cases of malignant bleeding or massive bleeding with inability to perform thermal therapy or hemoclip placement.
Endoscopists should understand the risk of bleeding from therapeutic endoscopic interventions (eg, endoluminal resection and endoscopic sphincterotomy) and be familiar with the endoscopic tools and techniques to treat intraprocedural bleeding and minimize the risk of delayed bleeding.
In patients with endoscopically refractory NVUGIB, the etiology of bleeding (peptic ulcer disease, unknown source, post surgical); patient factors (hemodynamic instability, coagulopathy, multi-organ failure, surgical history); risk of rebleeding; and potential adverse events should be taken into consideration when deciding on a case-by-case basis between transcatheter arterial embolization and surgery.
Prophylactic transcatheter arterial embolization of high-risk ulcers after successful endoscopic therapy is not encouraged.
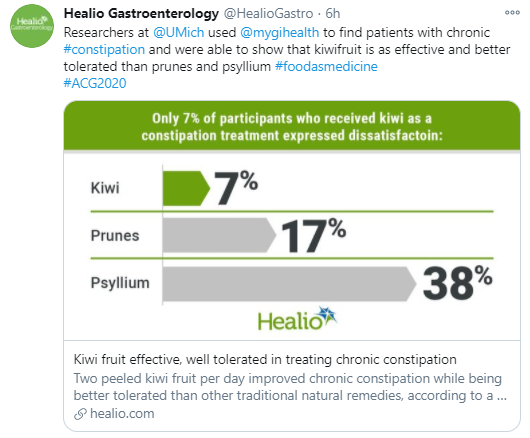
From a randomized (Virtual) ACG 2020 study from Samuel W. Chey and colleagues (University of Michigan), n=79 adults:
“All three treatments improved complete spontaneous bowel movement (P .003). Prunes demonstrated the largest magnitude of response at 67% vs. 64% for psyllium vs. 45% for Kiwi fruit”
“The highest proportion of participants – 68% – reported treatment satisfaction with kiwifruit while similar proportions of those receiving prunes and psyllium – 48% – reported satisfaction”
“The kiwi group had the lowest proportion of participants reporting treatment dissatisfaction at 7%….Participants receiving prunes and psyllium were more likely to report abdominal pain and bloating than those receiving kiwi”
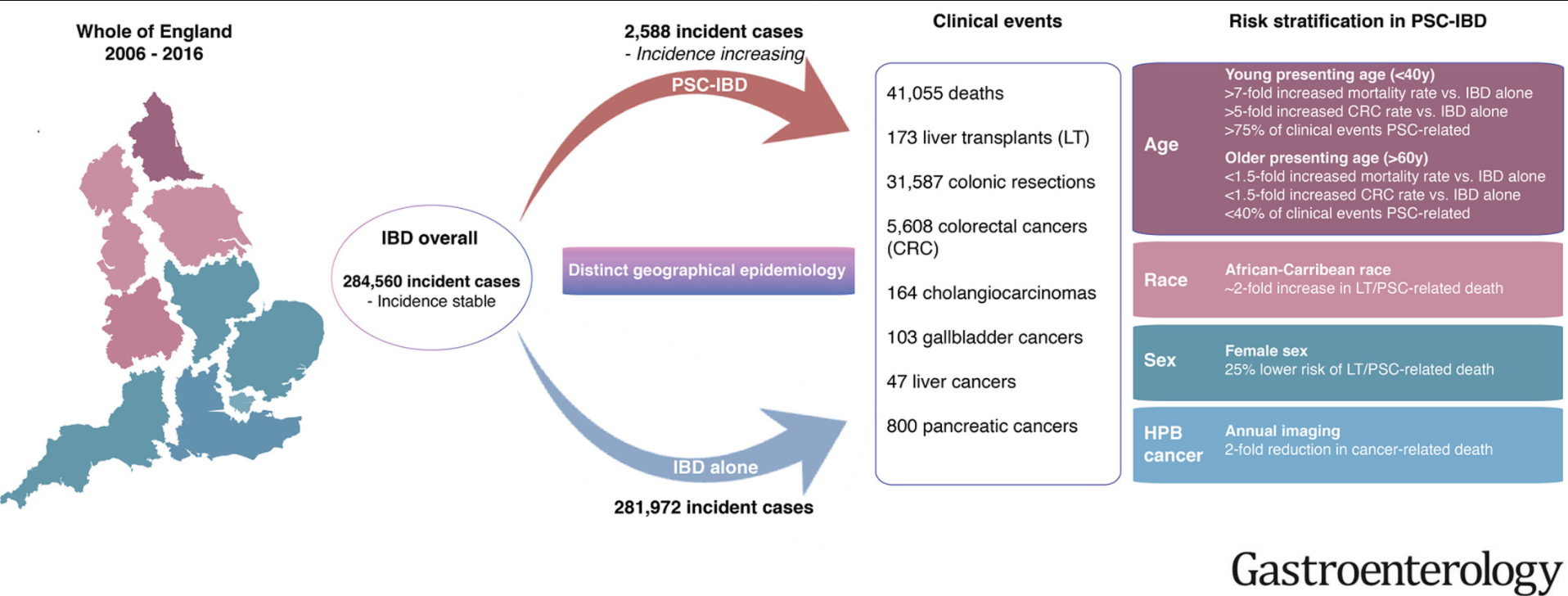
Methods: The authors linked prospectively collected data from national health care registries maintained for all adults in England on hospital attendances, imaging and endoscopic evaluations, surgical procedures, cancer, and deaths.
Key findings:
Over 10 years, we identified 284,560 incident cases of IBD nationwide; of these, 2588 patients developed PSC. This study excluded patients <18 years of age.
Development of PSC was associated with increased risk of death and CRC (hazard ratios [HRs], 3.20 and 2.43, respectively; P < .001) and a lower median age at CRC diagnosis (59 y vs 69 y without PSC; P < .001)
Compared to patients with IBD alone, patients with PSC-IBD had a 4-fold higher risk of CRC if they received a diagnosis of IBD at an age younger than 40 years
Development of PSC also increased risks of cholangiocarcinoma (HR, 28.46), hepatocellular carcinoma (HR, 21.00), pancreatic cancer (HR, 5.26), and gallbladder cancer (HR, 9.19) ( P < .001 for all)
The greatest difference in mortality between the PSC-IBD alone group vs the IBD alone group was for patients younger than 40 years
Patients with PSC-UC had >40% risk of colonic resection compared to patients with IBD alone (aHR 1.65)
My take: This study shows the impact the added diagnosis of PSC has for patients with IBD. One of the limitations in assessing outcomes is determining whether someone with IBD has PSC as there are a lot of patients with IBD who have asymptomatic changes in their biliary tree.
In an analysis (n= 279 adults, 70% female, average age 47 years) of patients with chronic constipation at a tertiary center who were referred for anorectal manometry, 19% had symptoms consistent with an eating disorder; this assessment was based on the Eating Attitudes Test (EAT-26).
“Gastrointestinal-specific anxiety fully mediated the relationship between the severity of ED pathology and constipation (standardized β, 0.11–0.16; P = .026–.024).”
The authors note that screening for eating disorders “is of particular importance before prescribing dietary interventions.”
My take: While this was a study with adults, it is likely that chronic constipation may be a presenting feature of an eating disorder in teenagers as well.
This prospective study combined 3-dimensional high-resolution manometry (3D-HRM) with detailed analysis of computed tomography images to study the EGJ (esophagogastric junction) in patients with achalasia (n=12) and healthy controls (n=10). Key finding: Besides LES, the 3D pressure profile of the EGJ can indicate anatomic and functional abnormalities of the crural diaphragm muscle in patients with achalasia esophagus
“In this edition of Gastroenterology, researchers led by Ravi Mittal …demonstrated an asymmetric, extrinsic CD (crural diaphragm) component to EGJ pressure superimposed on the intrinsic LES.”