The results of a phase 2 trial for Ozanimod have been published: WJ Sandborn et al. NEJM 2016; 374; 1754-62.
Ozanimod (RPC1063) is “an oral agonist of the sphingosine-1-phosphate receptor subtypes 1 and 5 that induces peripheral lymphocyte sequestration, potentially decreasing the number of activated lymphocytes circulating to the gastrointestinal tract.”
From the abstract:
METHODS
We conducted a double-blind, placebo-controlled phase 2 trial of ozanimod in 197 adults with moderate-to-severe ulcerative colitis. Patients were randomly assigned, in a 1:1:1 ratio, to receive ozanimod at a dose of 0.5 mg or 1 mg or placebo daily for up to 32 weeks. The Mayo Clinic score was used to measure disease activity on a scale from 0 to 12, with higher scores indicating more severe disease; subscores range from 0 to 3, with higher scores indicating more severe disease. The primary outcome was clinical remission (Mayo Clinic score ≤2, with no subscore >1) at 8 weeks.
RESULTS
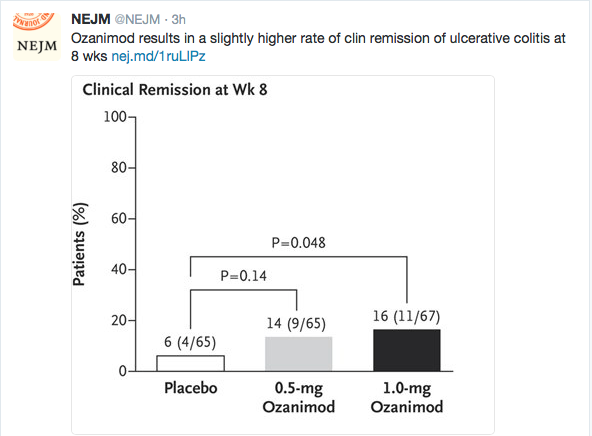
The primary outcome occurred in 16% of the patients who received 1 mg of ozanimod and in 14% of those who received 0.5 mg of ozanimod, as compared with 6% of those who received placebo (P=0.048 and P=0.14, respectively, for the comparison of the two doses of ozanimod with placebo). Differences in the primary outcome between the group that received 0.5 mg of ozanimod and the placebo group were not significant; therefore, the hierarchical testing plan deemed the analyses of secondary outcomes exploratory. Clinical response (decrease in Mayo Clinic score of ≥3 points and ≥30% and decrease in rectal-bleeding subscore of ≥1 point or a subscore ≤1) at 8 weeks occurred in 57% of those receiving 1 mg of ozanimod and 54% of those receiving 0.5 mg, as compared with 37% of those receiving placebo. At week 32, the rate of clinical remission was 21% in the group that received 1 mg of ozanimod, 26% in the group that received 0.5 mg of ozanimod, and 6% in the group that received placebo; the rate of clinical response was 51%, 35%, and 20%, respectively. At week 8, absolute lymphocyte counts declined 49% from baseline in the group that received 1 mg of ozanimod and 32% from baseline in the group that received 0.5 mg. The most common adverse events overall were anemia and headache.
In this preliminary trial, ozanimod at a daily dose of 1 mg resulted in a slightly higher rate of clinical remission of ulcerative colitis than placebo. The trial was not large enough or of sufficiently long duration to establish clinical efficacy or assess safety. (Funded by Receptos; TOUCHSTONE ClinicalTrials.gov number, NCT01647516.)
Related blog post: CCFA Conference Notes 2016 (part 5) -Emerging Therapies …