A recent ‘clinical quality forum’ sponsored by The Children’s Care Network (TCCN) and Nutrition4Kids featured several good lectures. The symposium was titled, “It’s Alimentary.” What follows are my notes –the full lectures from these talks will be available in the coming weeks on the Nutrition4Kids website. My notes may include some errors in transcription and errors of omission.
“The Fiber Movement: Why Kids Need It and How to Get It” by Maria Oliva-Hemker (Director of Division of Pediatric Gastroenterology, Johns Hopkins). This was a terrific lecture which pulled together a lot of useful information. Despite hearing a lot about fiber, this lecture showed me that there is a lot that I still need to learn.
Key points:
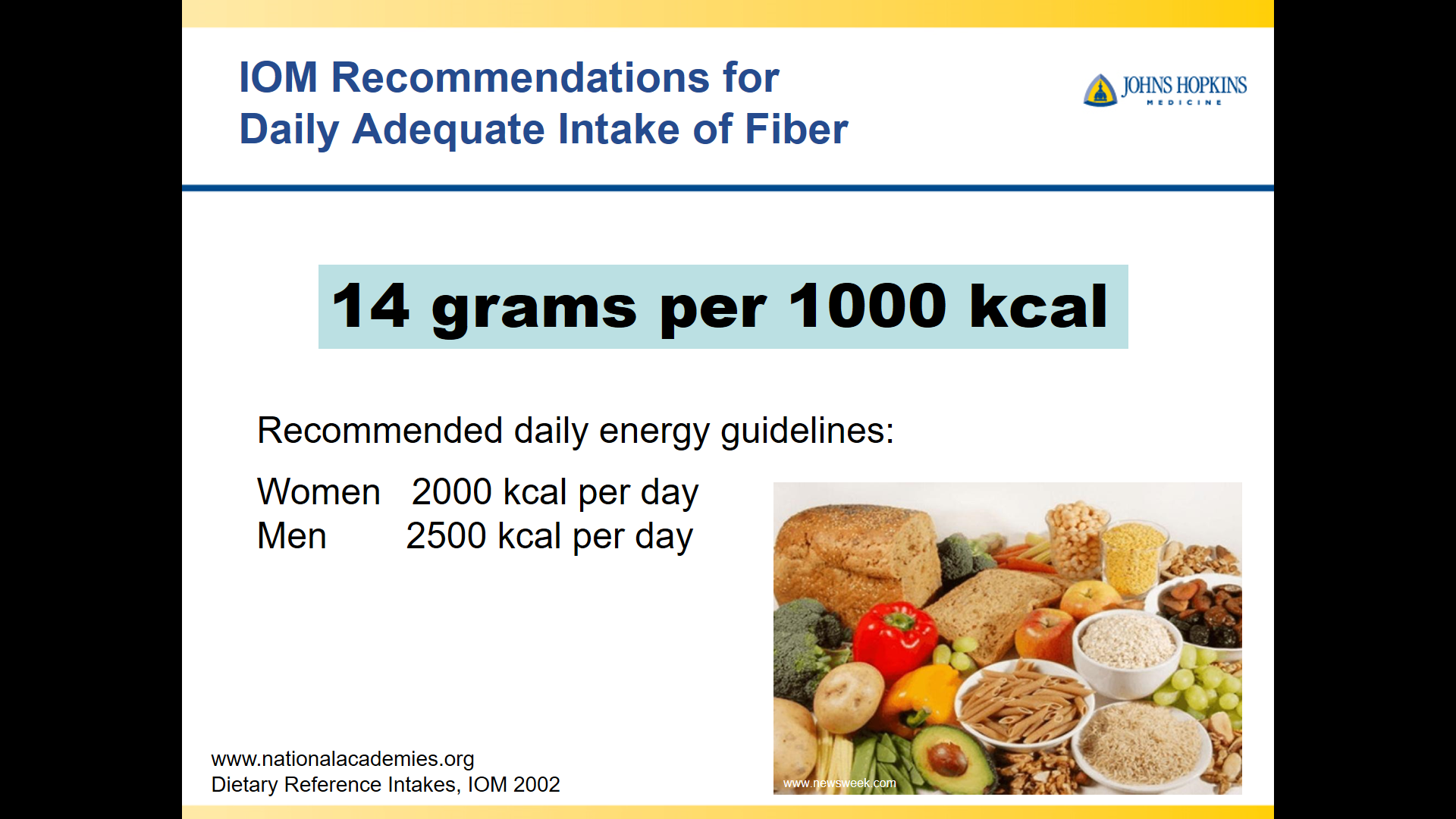
- Institute of Medicine recommends 14 grams of fiber per 1000 kcal of dietary intake. This is a higher amount of fiber than prior recommendations.
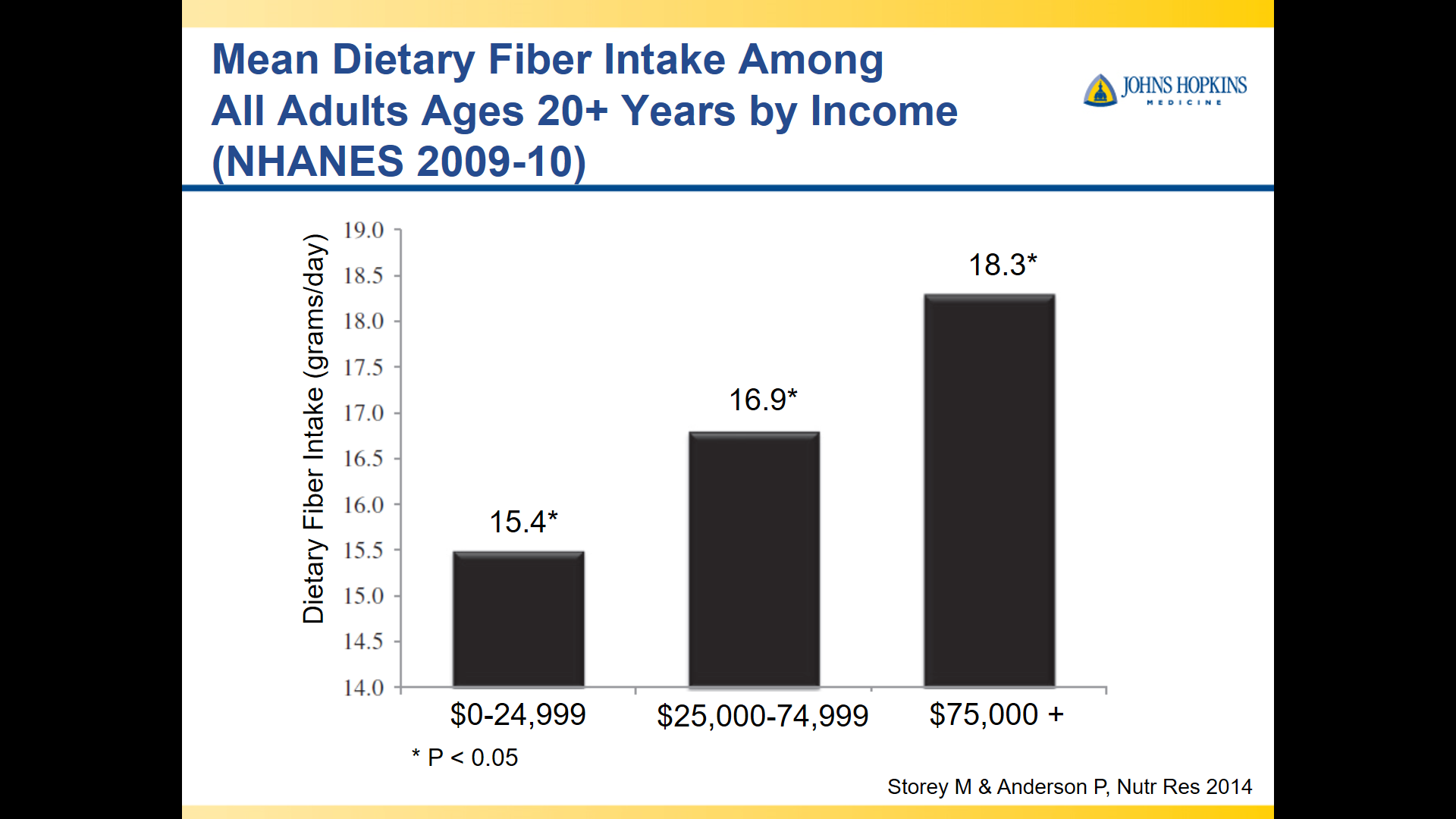
- Most adults are consuming about 50% of the fiber that they should
- Whole foods should be encouraged over fiber supplements
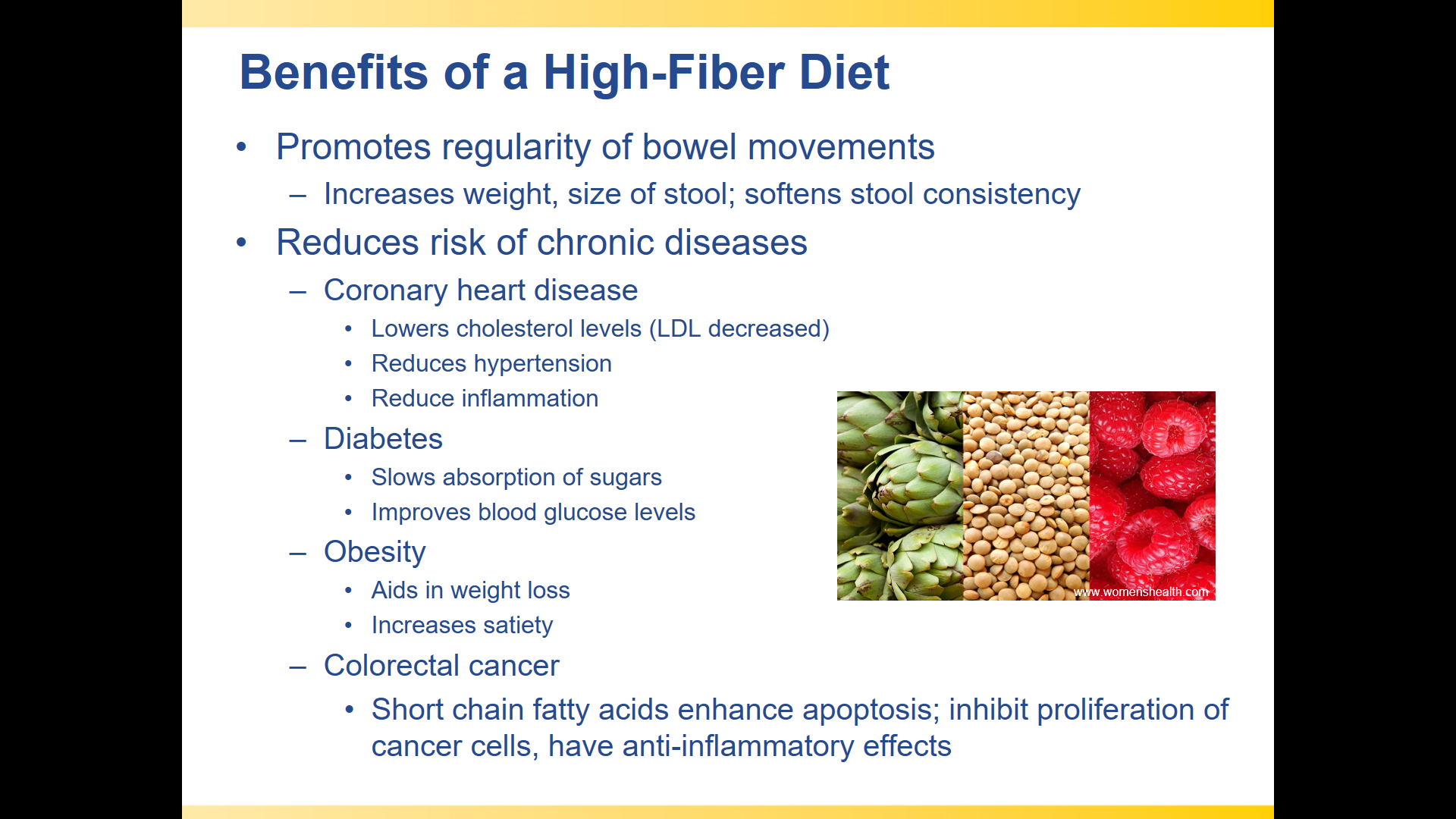
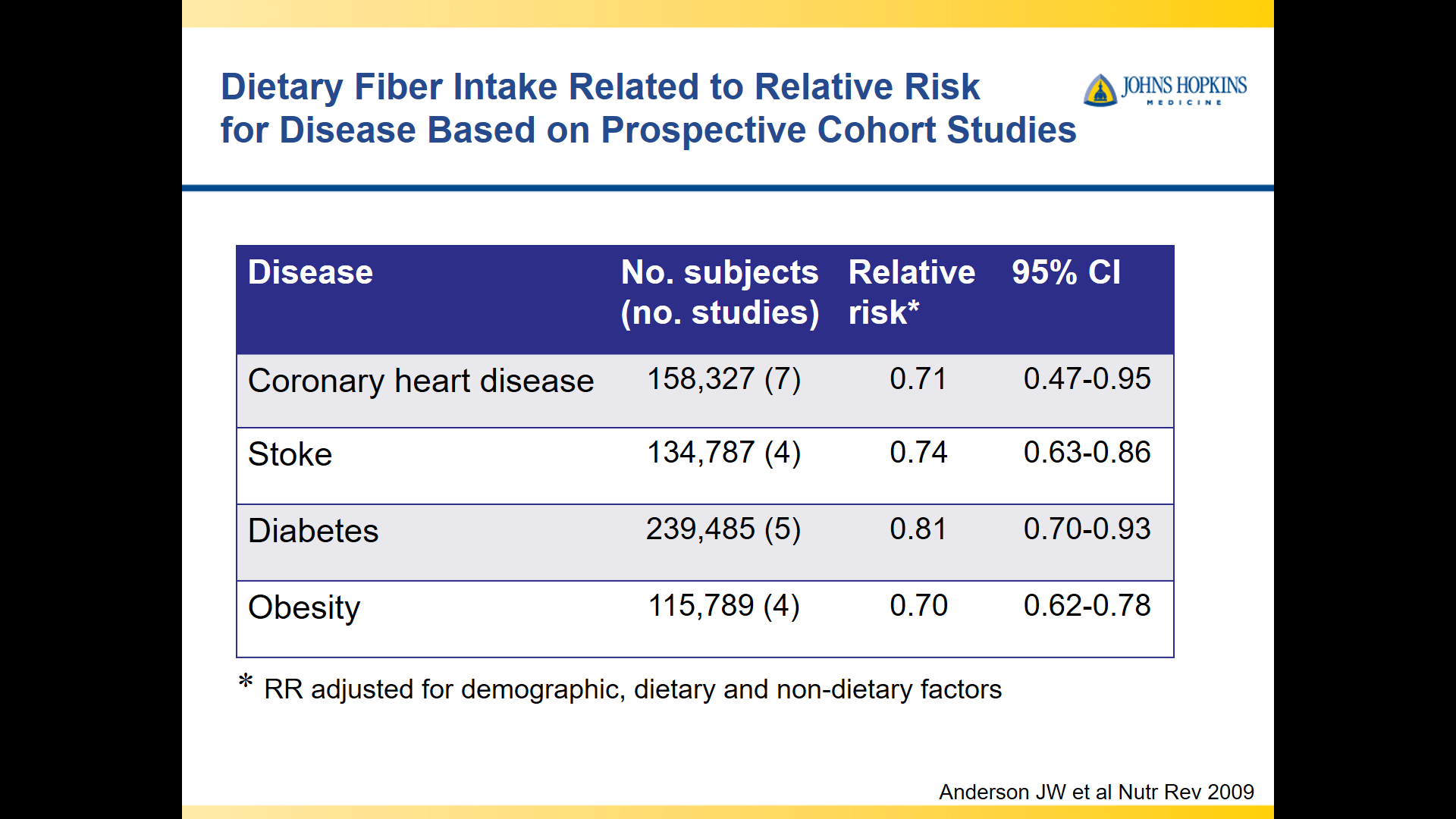
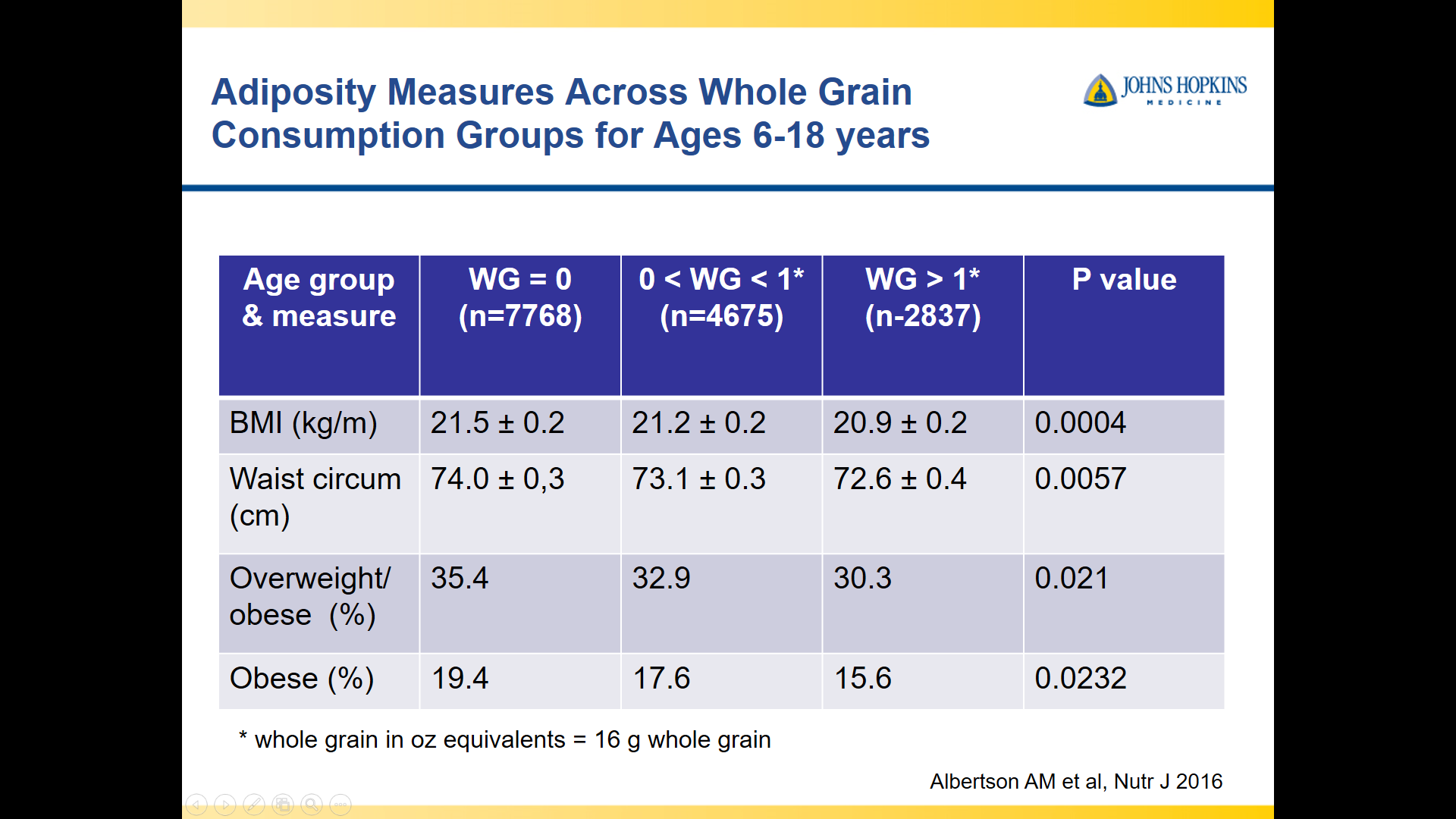
- Increased fiber associated with lower risk of obesity, stroke, coronary heart disease, and diabetes
Related blog posts:
- Why Fiber (Fruits and Veggies) Is Good For You
- Eat your veggies…if you do not want to get sick
- The Search for a Dietary Culprit for IBD
- Gut Microbiome, Crohn’s Disease and Effect of Diet
- Nutrition Week (Day 7) Connecting Epidemiology and Diet in Inflammatory Bowel Disease
- Dropping Weight by Adding Fiber in Diet | gutsandgrowth





“The LEAP Study and Its Implication for the Future of Food Allergies” Kiran Patel (Professor Pediatrics, Division of Allergy and Immunology, Emory University) This was the second opportunity that I had to hear Dr. Patel in the past 6 months –see An Allergy-Immunology Perspective on GI Diseases
Key points:
- There has been an increasing incidence of peanut allergies
- Early introduction of peanuts helps reduce peanut allergies. Suggested algorithm
- To reduce allergies, placing a best practice alert in electronic record could be necessary as rates of encouraging early peanut introduction in at risk children remains low
Related blog posts:
- The Peanut Story -From NEJM Blog | gutsandgrowth
- LEAP-ON Study: Early Peanuts Prevent Allergies | gutsandgrowth
- The “EAT” Study



LEAP study results
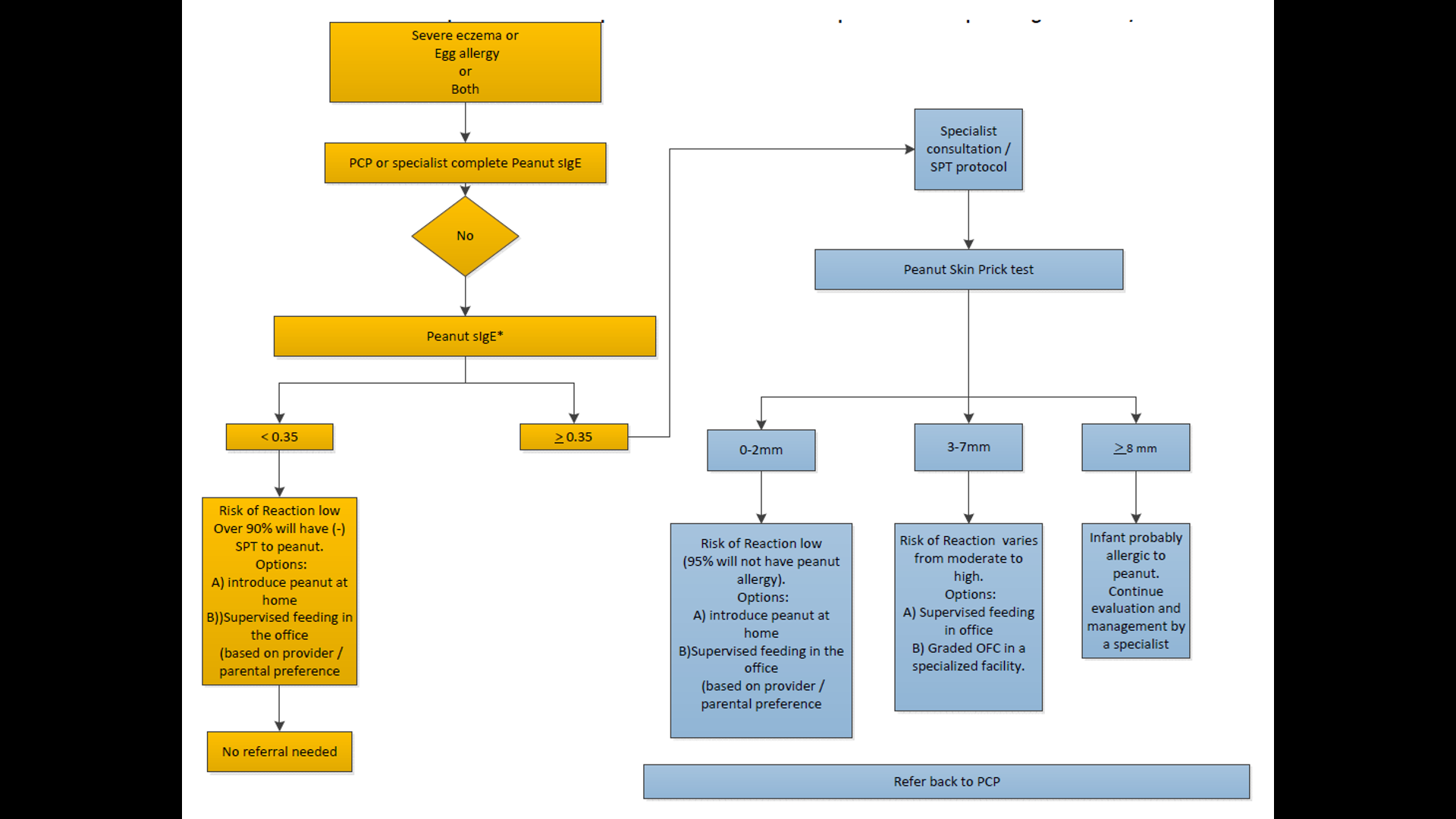


Slides with information on introduction of peanuts –this should be discussed with physician before implementation.


Disclaimer: These blog posts are for educational purposes only. Specific dosing of medications/diets (along with potential adverse effects) should be confirmed by prescribing physician/nutritionist. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.