
Here’s the link: Crash Test Dummies Fatter too!
Related blog posts:

In brief: A recent cross-sectional study (KM Clark et al. J Pediatr 2017; 181: 56-61) showed that breastfeeding at 9 months of age in Chinese infants was associated with iron deficiency anemia.. Iron deficiency can contribute to neurodevelopmental delays in addition to anemia.
My take: In later infancy (after 6 months of age), breastfeeding infants are at increased risk for iron deficiency anemia.
Looking at a retrospective cohort of 194 neonates, a recent study (SR Jadcherla et al. J Pediatr 2017; 181: 125-30) showed that infants discharged with a gastrostomy tube (Gtube) had associated lower cognitive outcomes.
The authors examined discharge milestones along with Bayley Scales of Infant Development (3rd edition) at 18-24 months of age.
Key findings:
My take: This study provides evidence for an expected finding –infants who need gtubes have poorer neurodevelopmental outcomes than infants who do not need gtubes.
Related blog posts:

Thanks to an Olive Oyl fan for this picture
A recent study (BA Carter et al. J Pediatr 2017; 181: 102-11) provides some preliminary data on the use of glucagon-like peptide-2 (GLP-2) (Teduglutide) for pediatric short bowel syndrome (SBS).
This was a 12-week, open-label study in patients aged 1-17 years with intestinal failure (IF) associated with SBS. Prior to the study, patients had shown little to minimal advance in enteral nutrition for at least 3 months. Three doses of GLP-2 (0.0125 mg/kg/d, 0.025 mg/kg/day, and 0.05 mg/kg/day).
Key findings:
My take: This open-label study has many limitations; further studies are planned (ClinicalTrials.gov, NCT02682381). Nevertheless, this study indicates that GLP-2 holds promise as a therapy for SBS/IF.
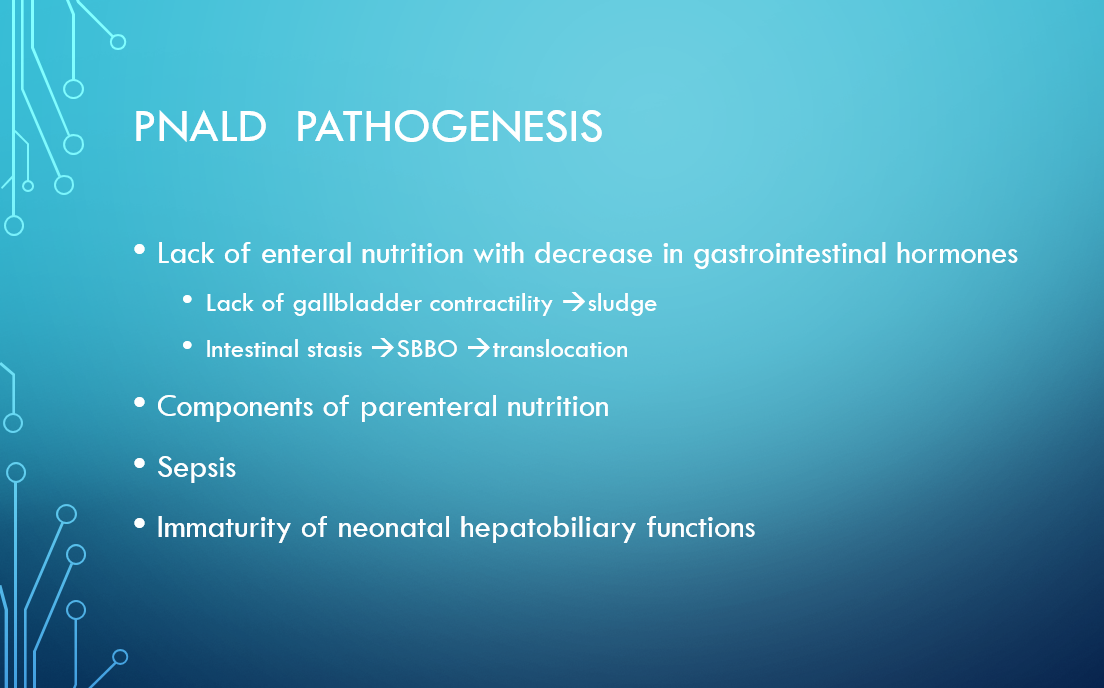
Another slide in a recent lecture on PNALD (slide derived from Conrad Cole lecture in Octobler 2015 -available at Pediatric Nutritionist Blog, slide 49):

Related blog posts:
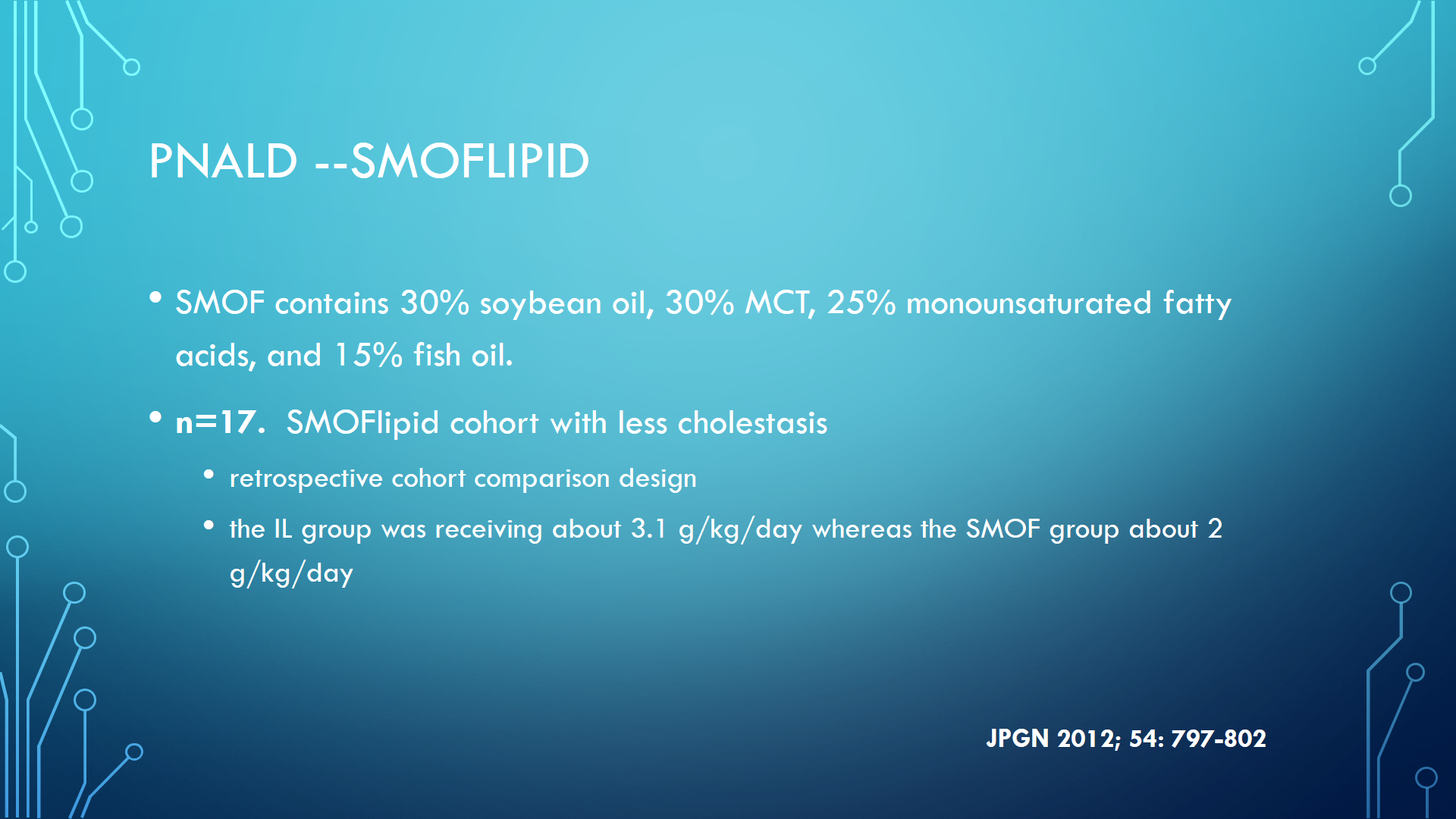
With newer lipid emulsions, there is the potential to give more lipids and have less liver injury. A recent report by Diamond et al (JPEN J Parenter Enteral Nutr. 2016 Feb 2. pii: 014860711562692) provides some of the best data for the use of SMOFlipid in infants: Preventing the Progression of Intestinal Failure-Associated Liver Disease in Infants Using a Composite Lipid Emulsion: A Pilot Randomized Controlled Trial of SMOFlipid.
Here’s the abstract: and afterwards some slides from a recent lecture that I gave regarding parenteral nutrition associated liver disease (and intestinal failure associated liver disease):
To examine whether SMOFlipid prevents progression of intestinal failure-associated liver disease (IFALD) in parenteral nutrition (PN)-dependent infants with early IFALD (conjugated bilirubin 17-50 µmol/L, 1-3 mg/dL).
Pilot multicenter blinded randomized controlled trial comparing SMOFlipid with Intralipid. Patients received the trial lipid for up to 12 weeks, unless they achieved full enteral tolerance sooner. The primary clinical outcome was the serum conjugated bilirubin.
Twenty-four infants (mean age, 6 weeks) participated in the trial (13 Intralipid and 11 SMOFlipid). At the time of trial enrollment, patients in both groups were receiving 90% of their calories by PN. Mean duration on trial was 8 weeks and did not differ according to treatment (P = .99). At trial conclusion, patients who received SMOFlipid had a lower conjugated bilirubin than those who received Intralipid (mean difference, -59 µmol/L; P = .03). Patients receiving SMOFlipid were also more likely to have a decrease in serum conjugated bilirubin to 0 µmol/L than those in the Intralipid group over the entire observation period (hazard ratio, 10.6; 95%; P = .03). The time to achievement of full enteral tolerance did not differ statistically (hazard ratio, 1.3; P = .59) between the groups. There was no significant difference in safety outcomes between the groups.
Compared with Intralipid, SMOFlipid reduces the risk of progressive IFALD in children with intestinal failure. This trial was registered at clinicaltrials.gov as NCT00793195.
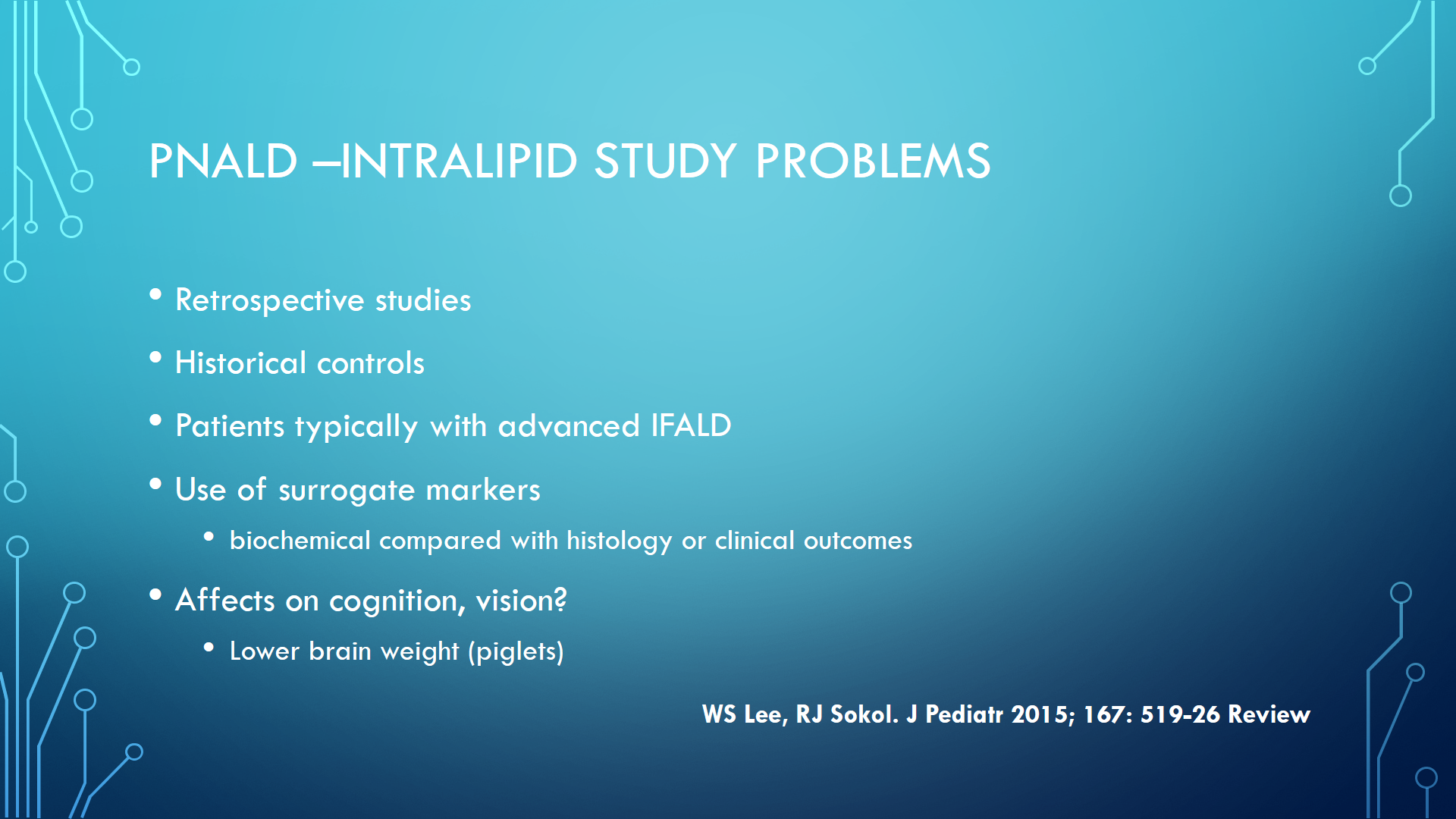
Here are a few more slides from my recent lecture on PNALD/IFALD:
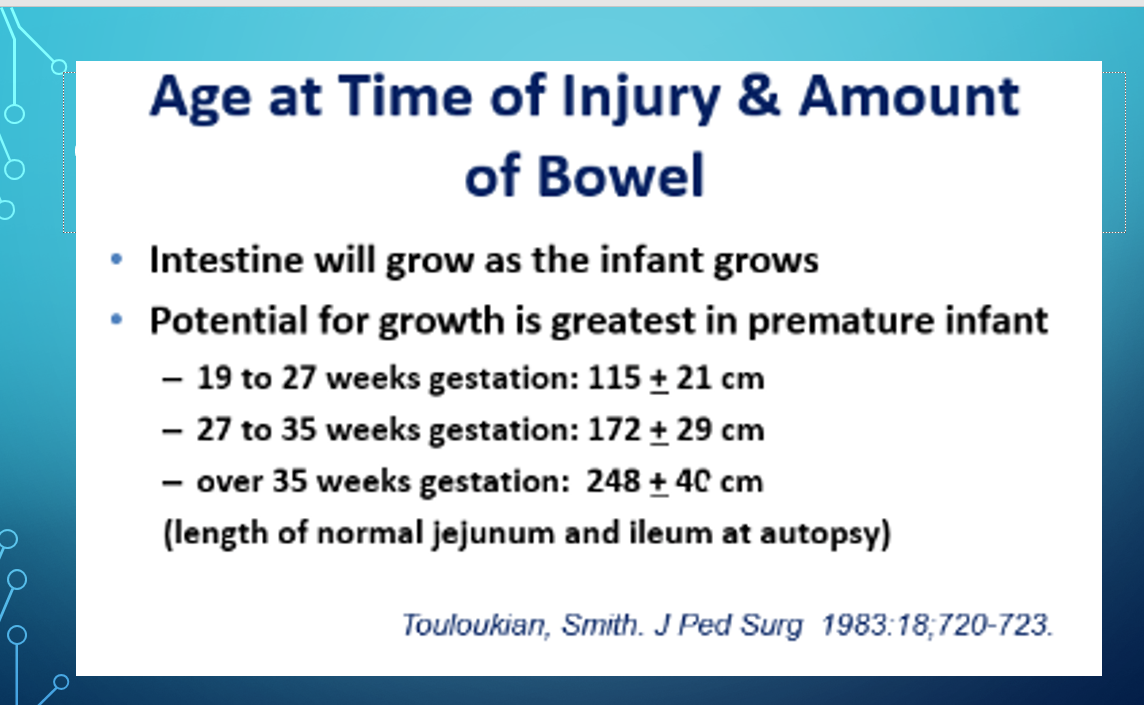
The above slide was borrowed from a talk by Dr. Conrad Cole on short bowel syndrome (available online via the Pediatric Nutritionist blog).
Related blog posts:
Recently I gave a lecture on parenteral nutrition associated liver disease (PNALD), though the term intestinal failure associated liver disease (IFALD) is probably more popular at this time. The day afterwards, I read an important study (L Beauport et al. J Pediatr 2017; 181: 29-36) reiterating one of the concerns in the lecture.
This study showed that higher lipid intake in a cohort of neonates born at <30 weeks during the first 2 weeks after birth was associated with a lower incidence of brain lesions and dysmaturation when examined by MRI at term equivalent age (TEA).
Details: This prospective cohort study examined energy/lipid intake in the first 2 weeks of life. Eligible patients were neonates ≤30 weeks. Group 1 with 27 patients had birth weight median of 900 gm compared with Group 2 with 15 patients had median weight of 844 gm. During the first year of the study, participants received a soybean emulsion whereas in the last year of the study, the neonates received a mixture of soybean and olive oil (Clinoleic).
Key finding: After adjusting for clinical risk scores and sepsis, the authors found that the higher energy/lipid intakes resulted in improved brain MRIs in group 1. A “10 Kcal/kg/day increase in energy of 0.7 g/kg/day increase in lipids intake would reduce the risk of having more severely abnormal MRI at TEA by >60%.”
Here are some slides from my talk relevant to this topic and to parenteral nutrition associated liver disease (PNALD):

Dr. David Suskind and colleagues have developed a website which provides a great deal of information regarding nutritional therapy, particularly the Specific Carbohydrate Diet (SCD), and inflammatory bowel disease. The website also facilitates contributions to Seattle Children’s Hospital and buying a book on the SCD.
Here’s a link to website: NIMBAL.org
Related blog posts:

Near Shem Creek, SC
A cross-sectional study (LN Anderson et al. J Pediatr 2017; 180: 47-52) of 2713 children extends prior observations that there is little evidence supporting the need for fasting prior to measurement of lipids.
Prior blog on this topic: Is Fasting Needed Before Checking Lipids
This study showed that fasting duration (0-5 hrs) was not significantly associated with total cholesterol, LDL, HDL, or triglycerides. This is most evident on the graphs on their Figure.
In the discussion, the authors note that the NHANES study 1999-2008 had similar results for the younger children. Overall, there were 12,744 children aged 3-17 years; 80% fasted at least 8 hrs. In this study, fasting did have a small effect on lipids, but among children 3-5 yrs, only LDL was statistically affected by fasting status.
My take: Based on this study and others, fasting seems to have only a small effect on lipid measurement and for routine screening, it is probably not needed.

Yosemite Natl Park
A small prospective study (M Manco et al. J Pediatr 2017; 180: 31-7) provides evidence that bariatric surgery/sleeve gastrectomy is effective at reversing nonalcoholic steatohepatitis (NASH) and hepatic fibrosis in adolescents (n=20).
All patients in this study had BMI >35 and weere 13-17 yrs of age.
Key findings at one year following intervention:
Full text link: Sleeve Gastrectomy for NASH
Limitations are discussed in the editorial by Inge and Xanthakos (pgs 6-7) and included small sample size, absence of patients with type 2 diabetes, and short followup period. Nevertheless, this is “the largest and most informative series…in select adolescents with severe obesity.”
My take: Given the lack of effective pharmaceutical therapy and the typically impotent effects of lifestyle intervention, this data supports bariatric surgery to facilitate weight loss/NASH reversal in select adolescents.
Related article: JCF Leung et al. Hepatology 2017; 65: 54-64. This study showed that the histologic severity and clinical outcomes are modestly better in nonobese patients (n=72) with NAFLD compared with obese patients (n=307). High triglycerides and higher creatinine were associated with more advanced liver disease in nonobese patients.
Briefly noted: D Houghton et al. Clin Gastroenterol Hepatol 2017; 15: 96-102. This study with 24 subjects with nonalcoholic steatohepatitis showed that exercise reduced hepatic triglyceride content, visceral fat, and plasma triglycerides. However, circulating markers of inflammation and fibrosis was not reduced. The implication is that exercise should be part of NASH treatment but that weight management/diet are needed as well.

Glacier Natl Park
. Related blog posts:
Our hospital has been working on childhood obesity and has developed a multifaceted program called “Strong4Life.” Recently the associated website has added some useful content for families.
From recent Children’s Healthcare of Atlanta email:
New Feeding and Wellness Resources for Parents
Children’s has launched a new feeding and wellness resource section on its dedicated parenting website, Strong4Life.com. The site is full of articles, videos and tools that new parents will find essential. From birth through school-age, Strong4Life equips parents to deal with everything from bedtime battles and mealtime tantrums, to food parenting and picky eating, and everything in between. With filtering of content by age of child, parents can now access relevant, easy-to-try tips, facts and advice from Children’s doctors, registered dietitians and wellness experts, who are also parents.
A sampling of the many articles and videos can be found here:
Other recommendations from Strong4Life:
Added Sugars
In August, the American Heart Association released its recommendations on the consumption of added sugars for children ages two to 18 years old. Children in this age range should not consume more than six teaspoons or 25 grams of added sugar per day; and children under age two should avoid it altogether. To learn where sugar may be hiding in children’s diets and simple ways to avoid it, visit strong4life.com/sugar.
Screen Time
The American Academy of Pediatrics (AAP) fine-tuned their screen time guidelines, to align better with the digital world we live in:

