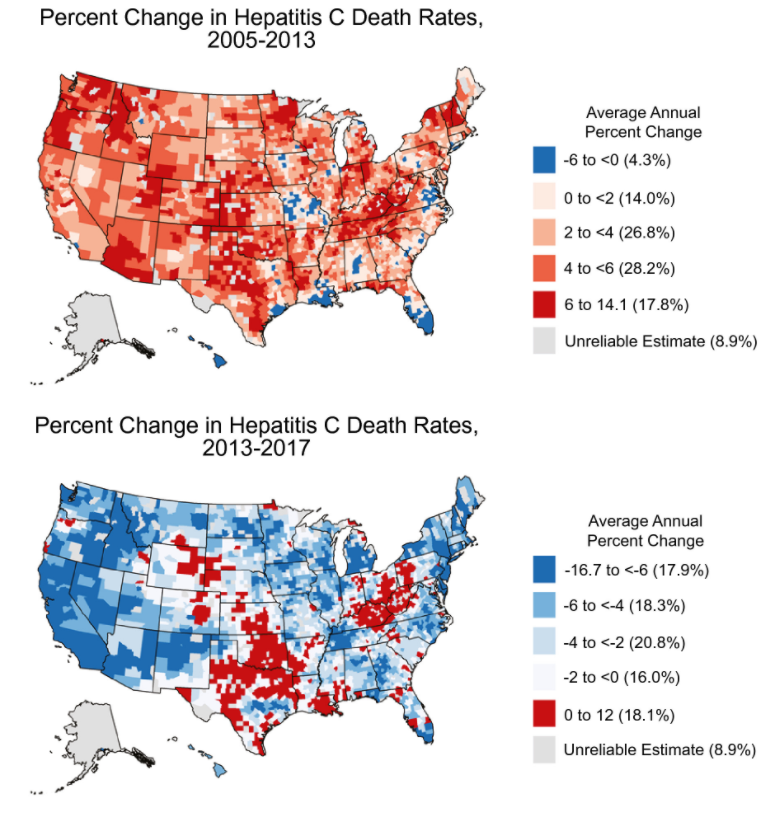
The authors used county-level HCV death rates and assessed trends in HCV mortality from 2005 to 2013 and from 2013 to 2017; the study is derived from mortality data from the National Vital Statistics System.
Key Findings:
Nationally, the age-adjusted HCV death rate peaked in 2013 at 5.20 HCV deaths per 100,000 persons and decreasing to 4.34 per 100,000 persons in 2017
There was heterogeneity in HCV mortality with the highest rates being concentrated in the West, Southwest, Appalachia, and northern Florida. 80% of counties had improvement in HCV mortality
My take: This study showed widespread improvement trends in HCV death rates from 2013 to 2017 and provides benchmarks for further progress. However, other studies have shown increasing rates of HCV tied to opioid crisis which could impact long-term outcomes as well.
In this retrospective study of 65 healthy infants (<3 months of age, median age 2 months) who had CT scans performed due to trauma, the authors investigated the frequency of a fatty liver.
Key findings:
Depending on the criteria used, 23% or 26% of infants had evidence of fatty liver on CT scan
The prevalence of maternal obesity and/or diabetes was 11% (of the 65 pregnancies) but there was no significant difference in maternal risk factors between infants with and without evidence of steatosis
My take: Whether the fatty liver seen on CT scans in this infant cohort persists and evolves to adolescent and adult fatty liver disease is unknown but intriguing.
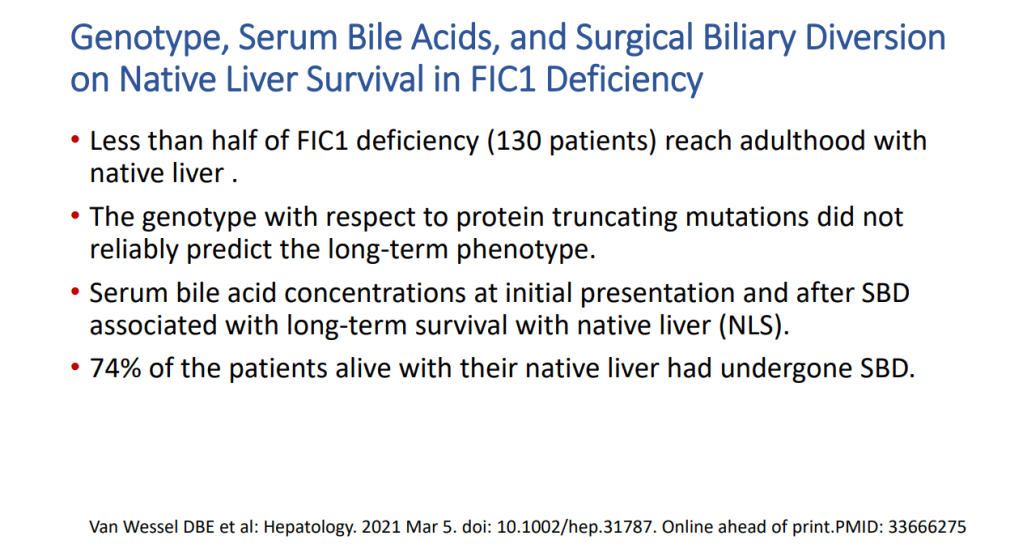
This huge collaborative study with 130 patients provides a great deal of information about familial intrahepatic cholestasis type 1 (FIC1). Key findings:
Survival analysis showed an overall native liver survival (NLS) of 44% at age 18 years. NLS was comparable among FIC1-A, FIC1-B, and FIC1-C (% NLS at age 10 years: 67%, 41%, and 59%, respectively; P = 0.12)
The number of predicted protein truncating mutations did not correlate with natural history or prognosis
In this study, the researchers 834 patients with CHB previously treated with TDF for ≥12 months who were switched to TAF in routine practice at 13 US and Asian center. Key findings:
“Overall, we observed continued improvement in virologic response, ALT normalization, and no significant changes in eGFR following switch to TAF from TDF.”
HBV DNA suppression increased from 88% to 92% at 48 weeks post-switch, and then 95% at 96 weeks postswitch
Improved renal function: “By week 96, 21% (55/267) of patients with CKD stage 2 at switch improved to stage 1 and 35% (30/85) of CKD stage 3-5 patients improved to stage 2 and 1.2% (1/85) to stage 1.”
This practice guidance (with 276 references) is an update from similar guidelines published in 2012.
Key Points For Children:
Children with cirrhosis and ascites should be referred for evaluation for LT
Children undergoing LVP should receive 25% albumin infusion of 0.5-1.0 g/kg, or 6-8 g per liter of ascites removed.
Diagnostic paracentesis should be performed in children with ascites and fever, abdominal pain, or clinical deterioration. The risks and benefits of this procedure for use in all children with new ascites but without these symptoms have not been defined.
Obituary from Cincinnati Enquirer:James E. Heubi. “In lieu of flowers, memorial contributions may be made to the James Heubi Fund at Cincinnati Children’s Hospital Medical Center: http://www.cincinnatichildrens.org/donate. Please direct funds to “other” and type “James Heubi Fund.”
———————————————-
This is the last of my lecture notes from this year’s Aspen Webinar 2021. This was a fantastic update by Dr. Balistreri highlighting the incredible advances in understanding the myriad of disorders which present as neonatal cholestasis.
This blog entry has abbreviated/summarized this presentation. Though not intentional, some important material is likely to have been omitted; in addition, transcription errors are possible as well.
Key points:
Idiopathic neonatal hepatitis was attributed as diagnosis in ~65% of cases in 1970 but in 2021 accounts for ~10%
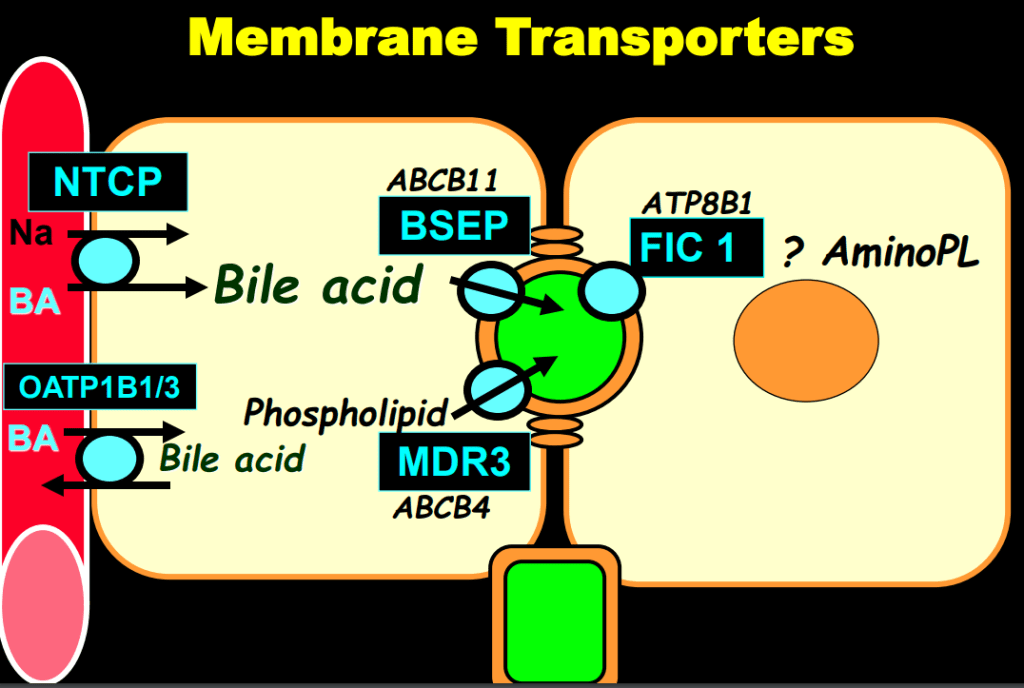
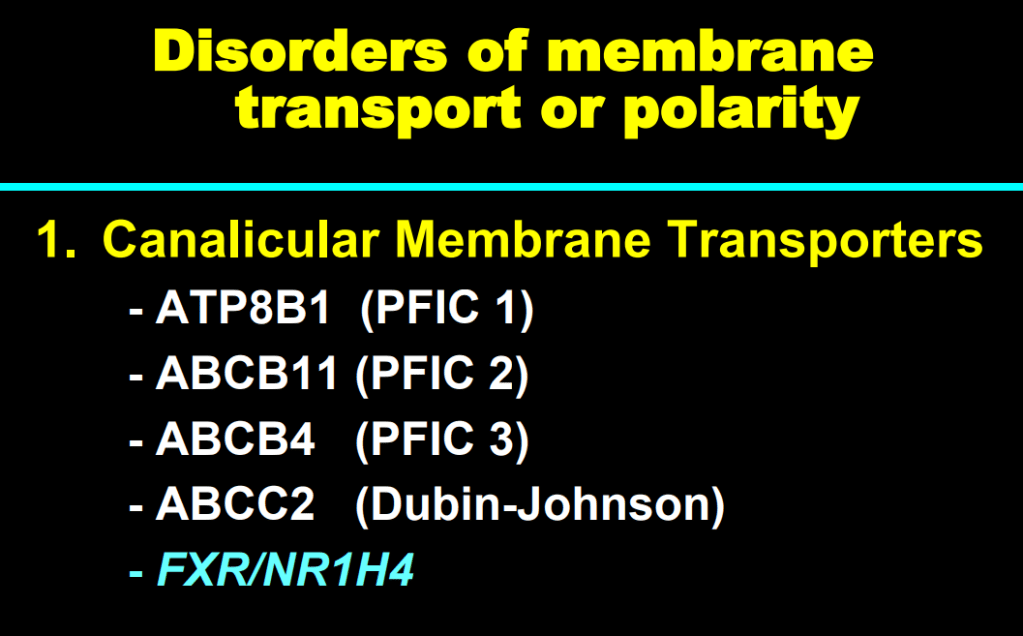
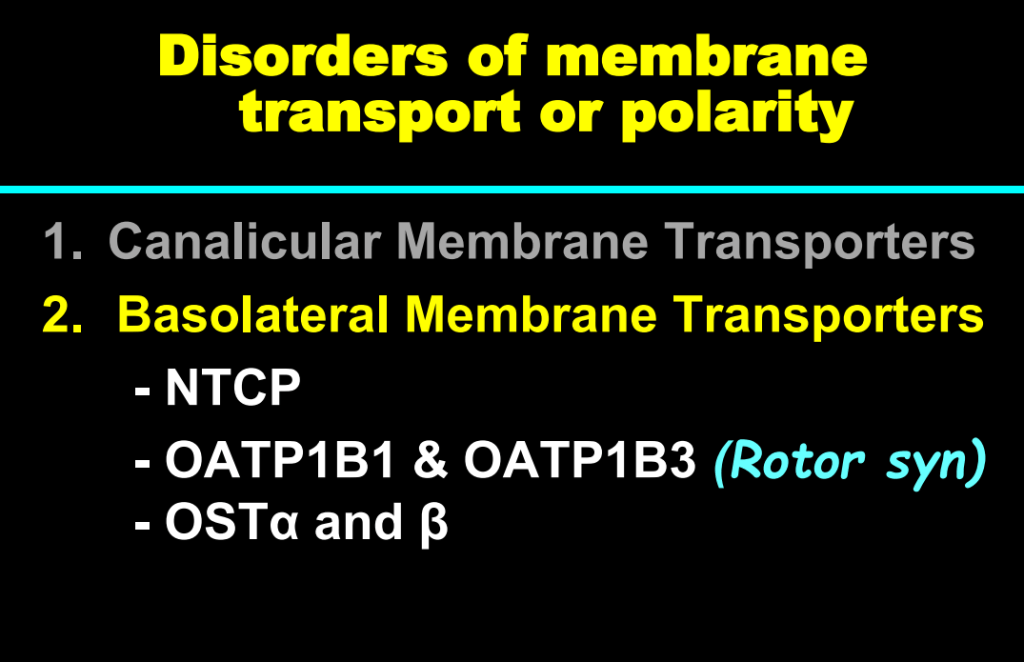
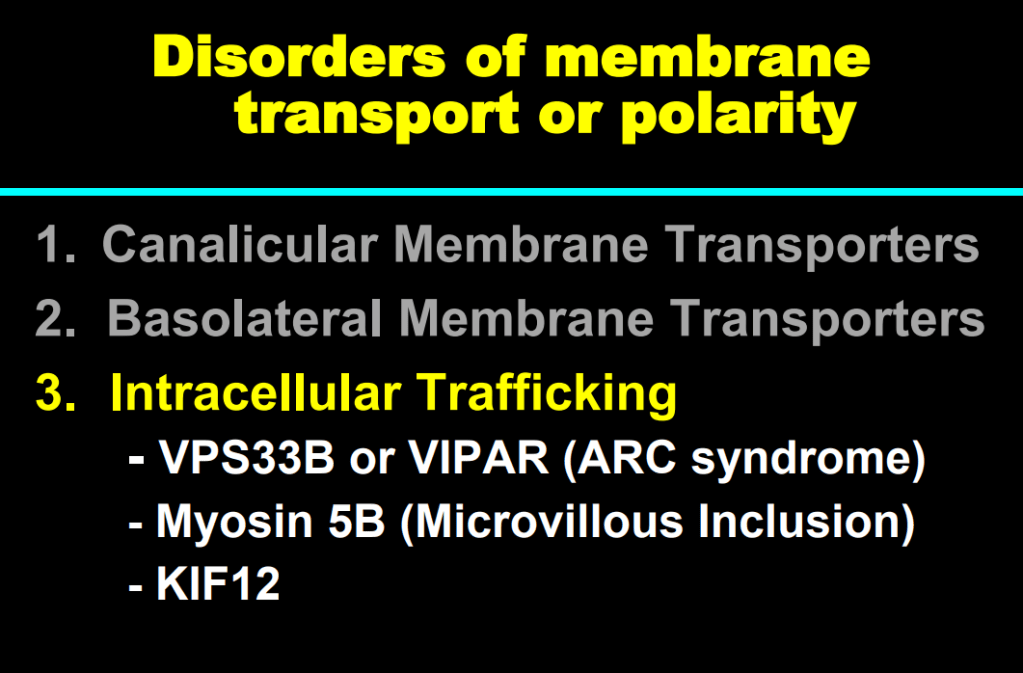
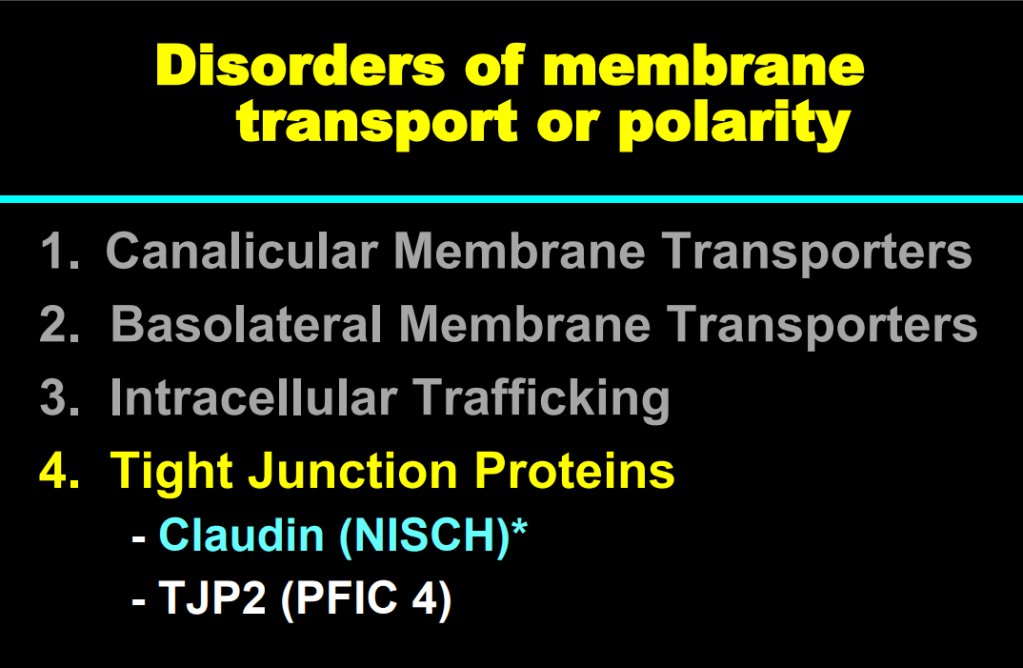
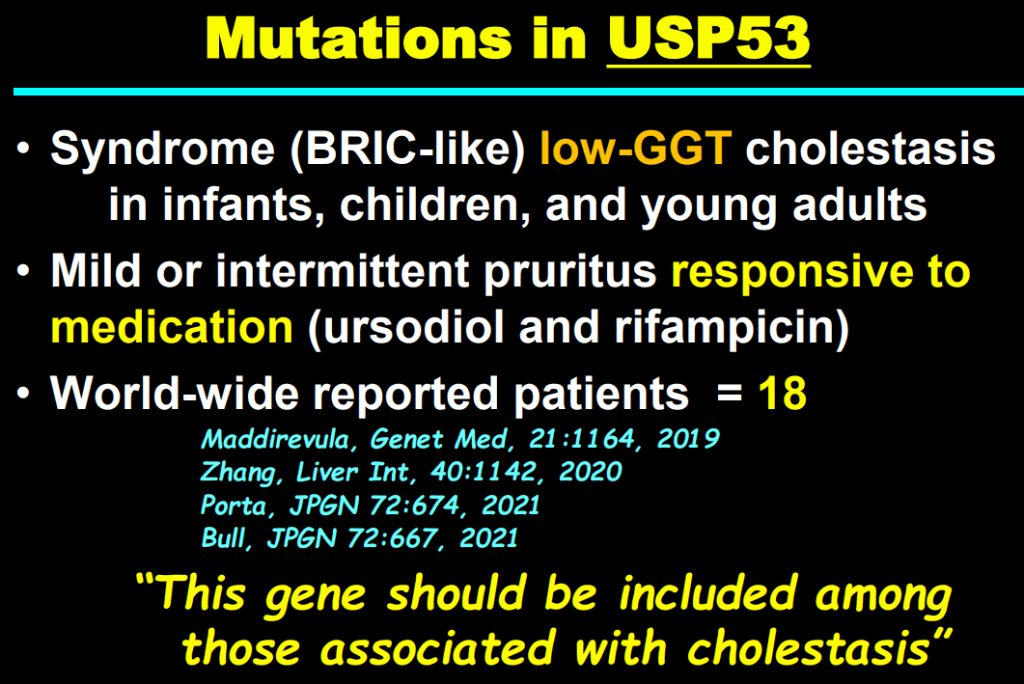
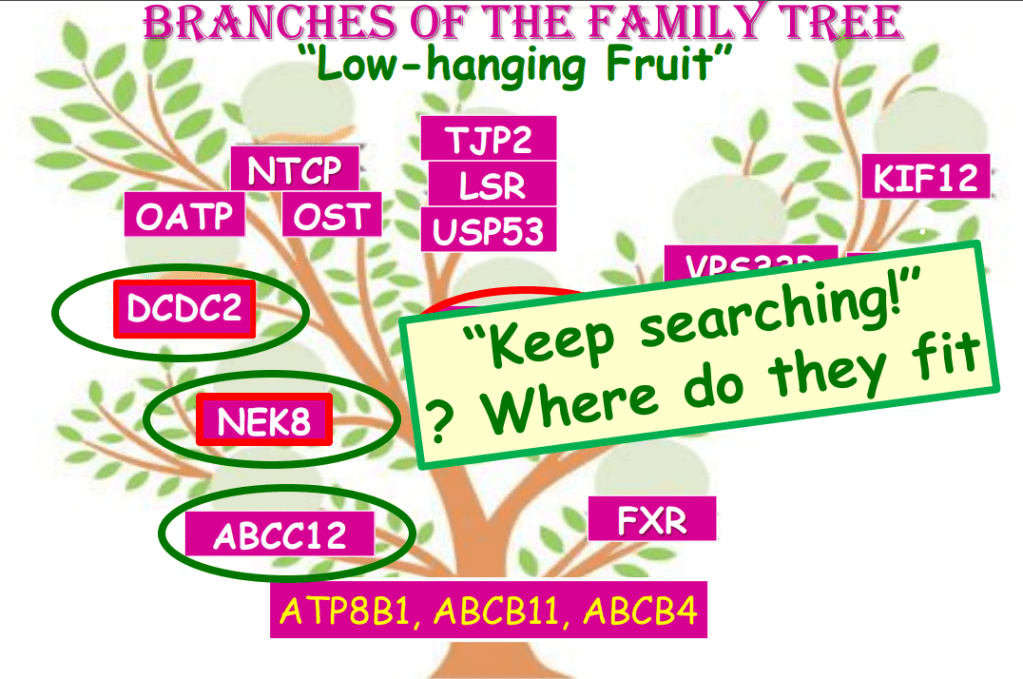
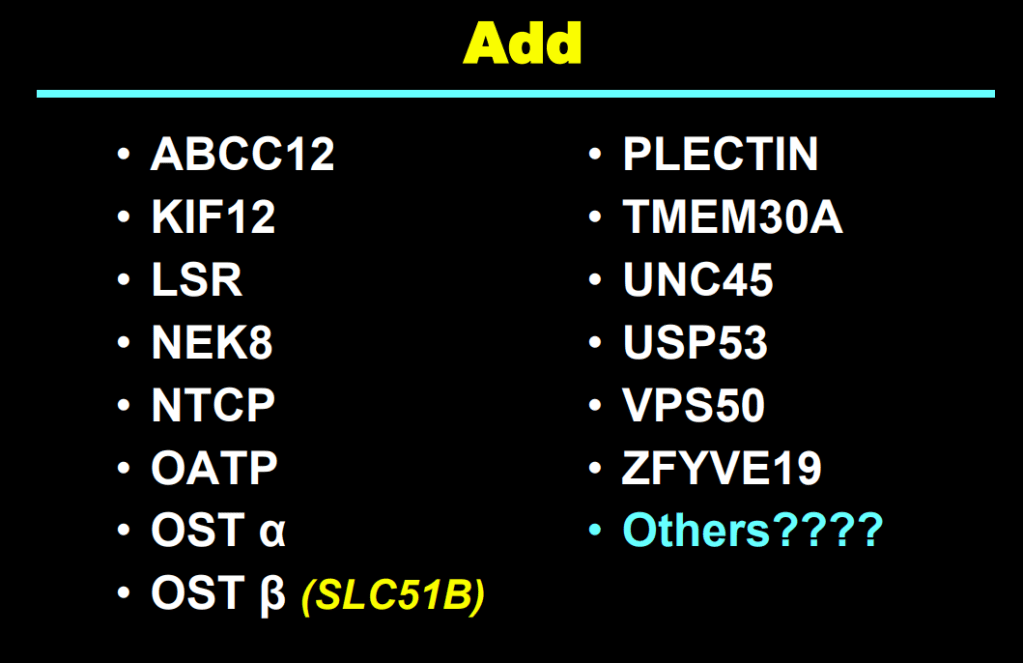
A lot of new disorders identified which interfere with bile flow
FXR helps prevent intrahepatic bile acid accumulation
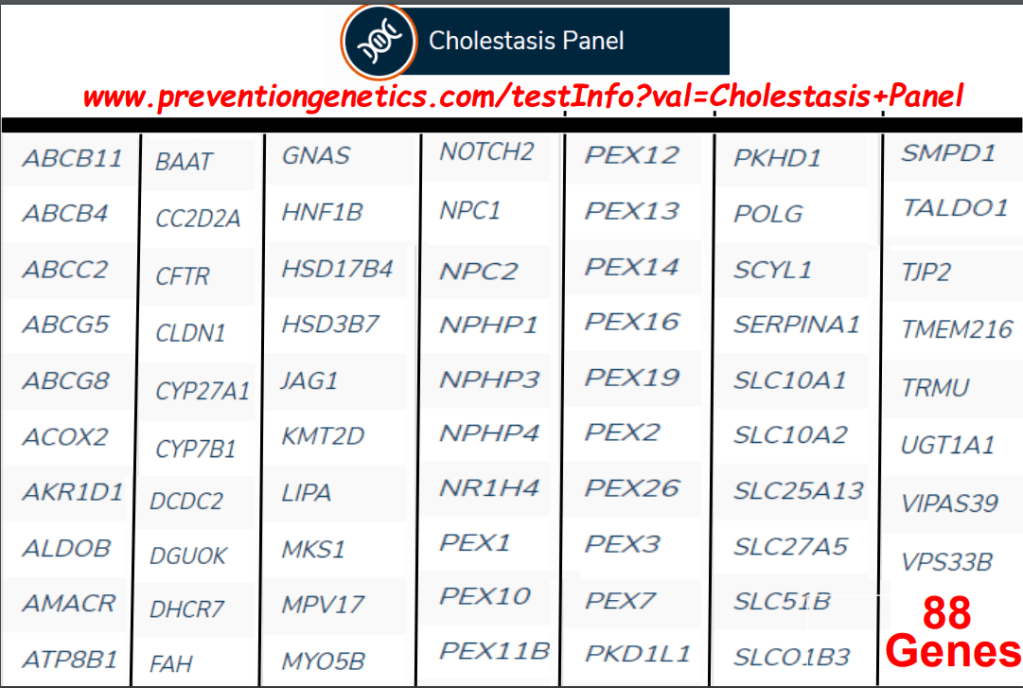
Genetic panels (~88 genes) quickly identify most disorders, but new disorders may be missed and need whole exome
10 mo with jaundice and pruritus. Labs note cholestasis (D bili 7.7), normal GGT, and mild elevation of transaminases. Unremarkable ultrasound. Liver biopsy showed nonspecific changes (cholestasis, no significant fibrosis). Genetic testing led to a diagnosis of PFIC. DDx: Obstruction, Infection, Toxic (drugs), Metabolic/Genetic including Alagille, PFIC
SAVE THE DATE for next year’s conference: July 11-15, 2022 in Snowmass Village, CO
More from Aspen Webinar 2021. This blog entry has abbreviated/summarized several presentations. Though not intentional, some important material is likely to have been omitted; in addition, transcription errors are possible as well. Great lecture from Jim Squires.
Key points:
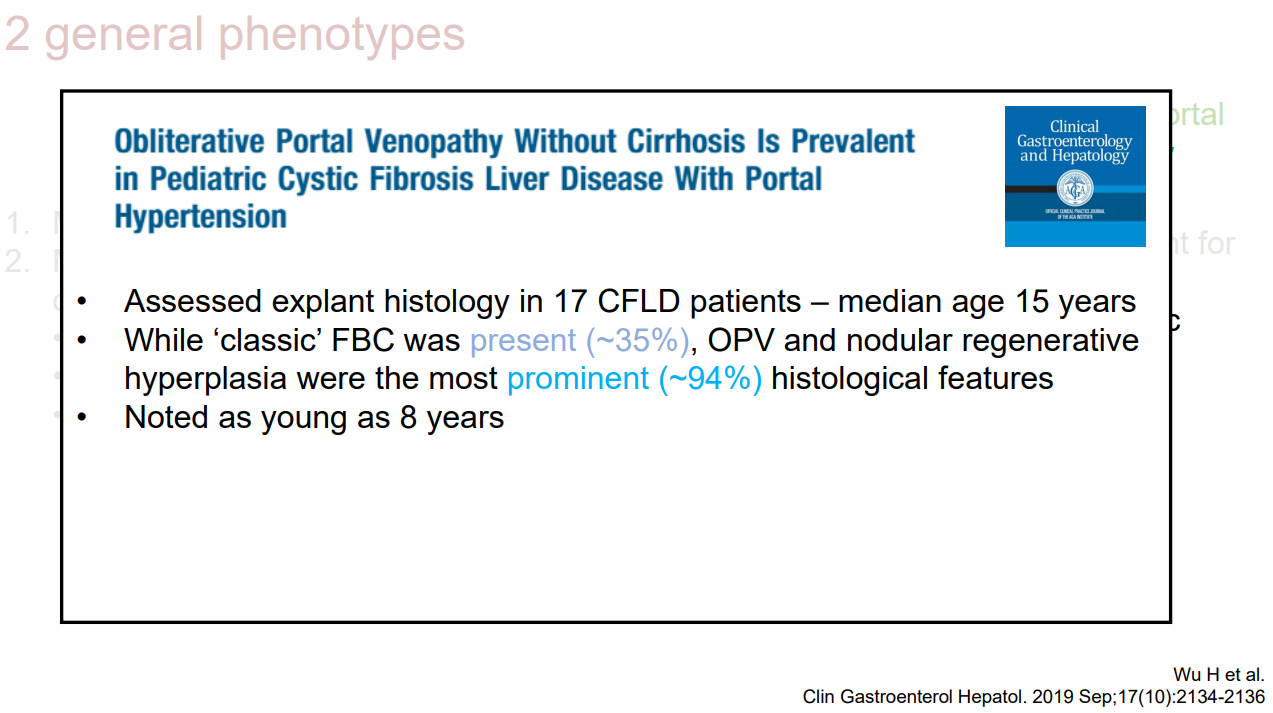
Cystic Fibrosis Liver Disease (CFLD) is variably defined
Risk factors include male patients, DeltaF508 mutations, meconium ileus and SERPINA1 Z allele
Two main phenotypes: Classic “Focal Biliary Cirrhosis” and Obliterative Portal Venopathy (increasingly recognized)
Intestinal microbiome and gut permeability/endotoxins may influence liver disease
Treatments: ursodeoxycholic acid may be helpful but overall evidence is low quality. Cochrane review does NOT recommend its routine use
More from Aspen Webinar 2021. This blog entry has abbreviated/summarized several presentations. Though not intentional, some important material is likely to have been omitted; in addition, transcription errors are possible as well. On the last day of this webinar conference, there were three more terrific lectures which addressed topics related to a a failing liver.
Key points:
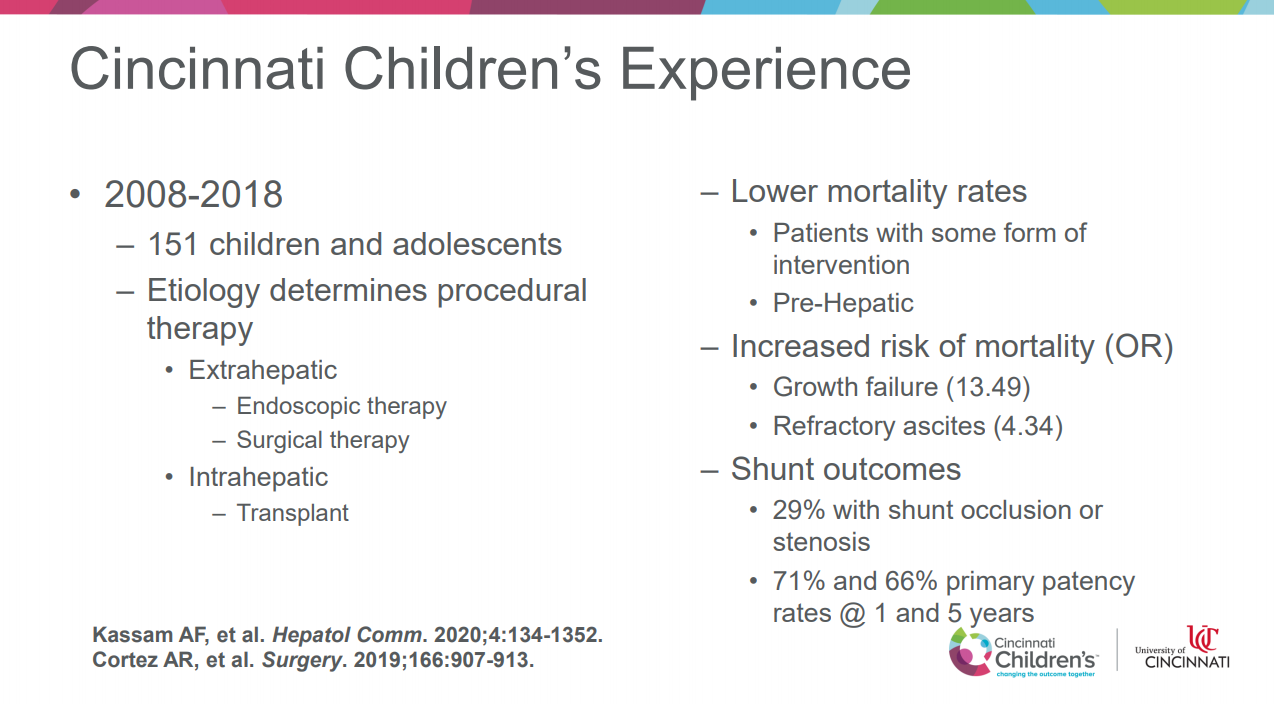
Surgical options are based on primary etiology: pre-hepatic, intra-hepatic, and post-hepatic
Rex procedure is technically difficult but is preferred for pre-hepatic obstruction
Warren Shunt (distal splenorenal) and TIPS can be done for intrahepatic disease
Often difficulty in selecting patients for surgical shunting beyond refractory bleeding
Some slides:
Experience at Cincy with portal hypertension patients and shunting
Key points:
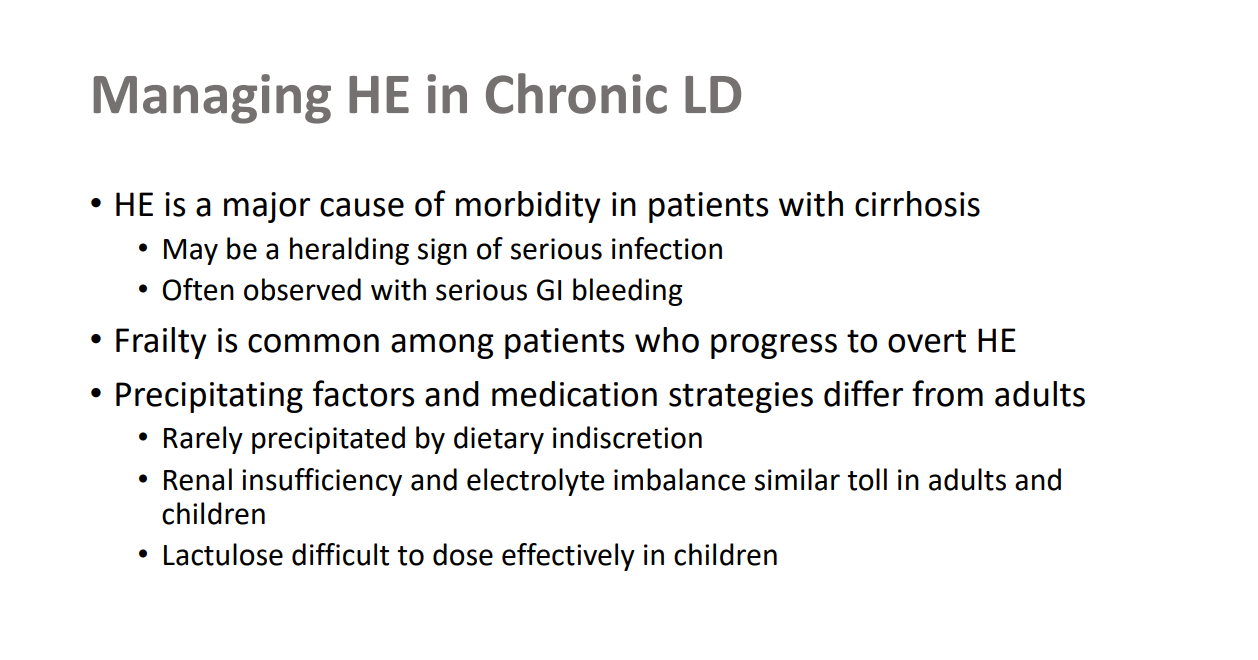
Hyperreflexia is a good indicator of stage 3 of HE
Patients with HE need to be managed in ICU
MARS is being used in some centers (even in infants)
Complications of ESLD -Kathy Campbell
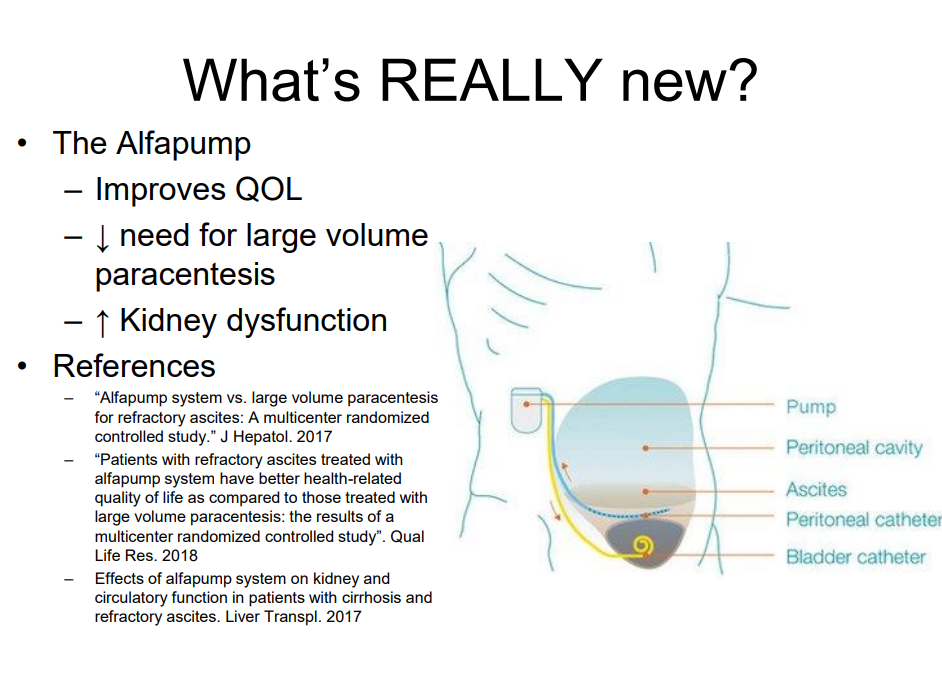
This talk provided a good overview of complications including ascites, variceal bleeding, frailty & sarcopenia, and hepatopulmonary syndrome.
More from Aspen Webinars. This blog entry has abbreviated/summarized several presentations. Though not intentional, some important material is likely to have been omitted; in addition, transcription errors are possible as well.
Dr. Mieli-Vergani presented case report of a boy with autoimmune sclerosing cholangitis and associated colitis who presented with minimal symptoms.
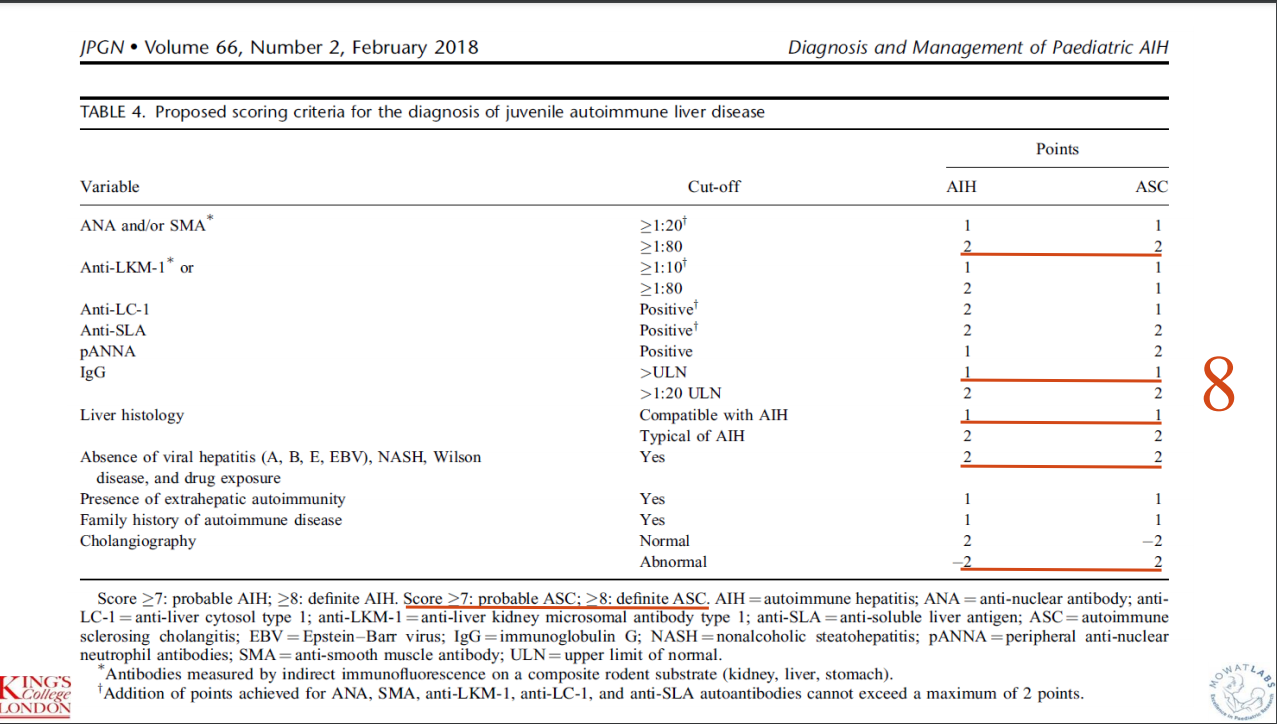
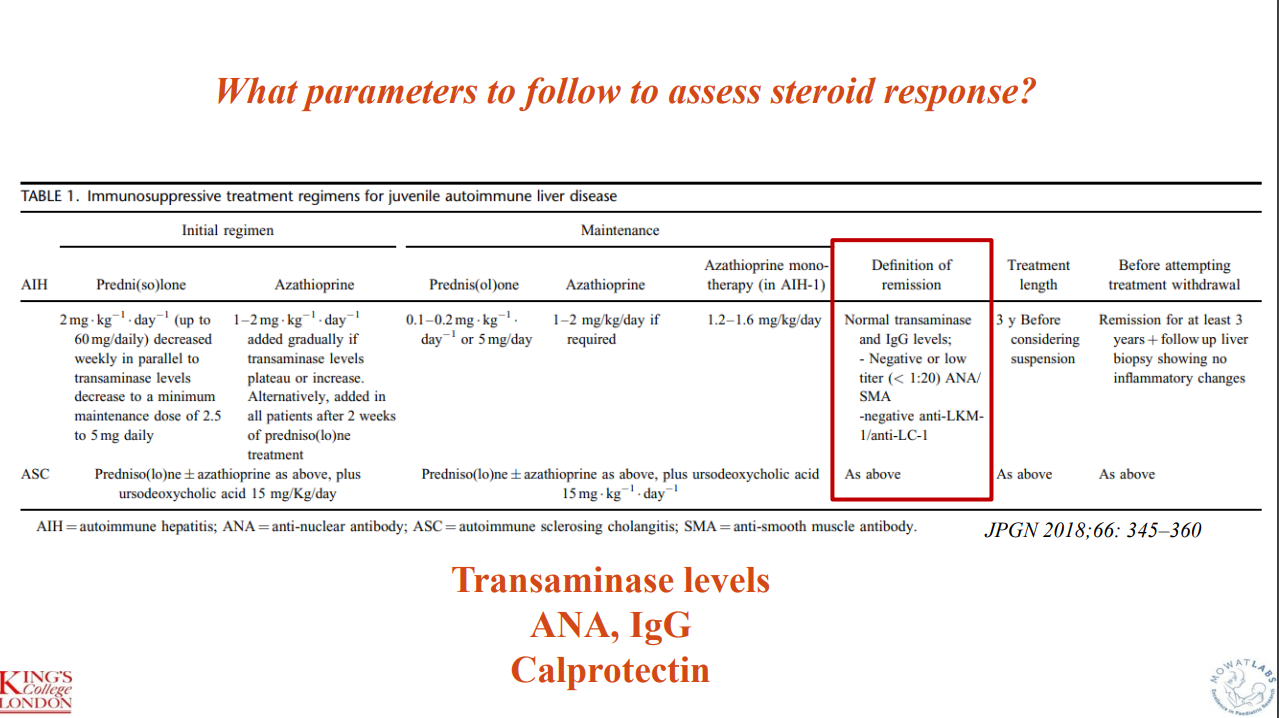
This case report highlights the evaluation and management of autoimmune liver disease hepatitis. Workup included autoimmune serology, GGT, celiac serology, calprotectin, and ultrasonography. EGD-Colonoscopy was prompted by elevated calprotectin. MRCP was prompted by elevated GGT (GGT were normal at the time of biopsy and MRCP) and liver biopsy findings.
“My message is that MRCP and colonoscopy should be done in all cases of autoimmune liver disease in children and adolescents, irrespective of calprotectin levels or elevated GGT and biliary changes on histology, as both IBD and sclerosing cholangitis can be present without any of the classical symptoms and signs. Only by doing this it is possible to reach an early diagnosis which is essential for early treatment and for a good outcome.”
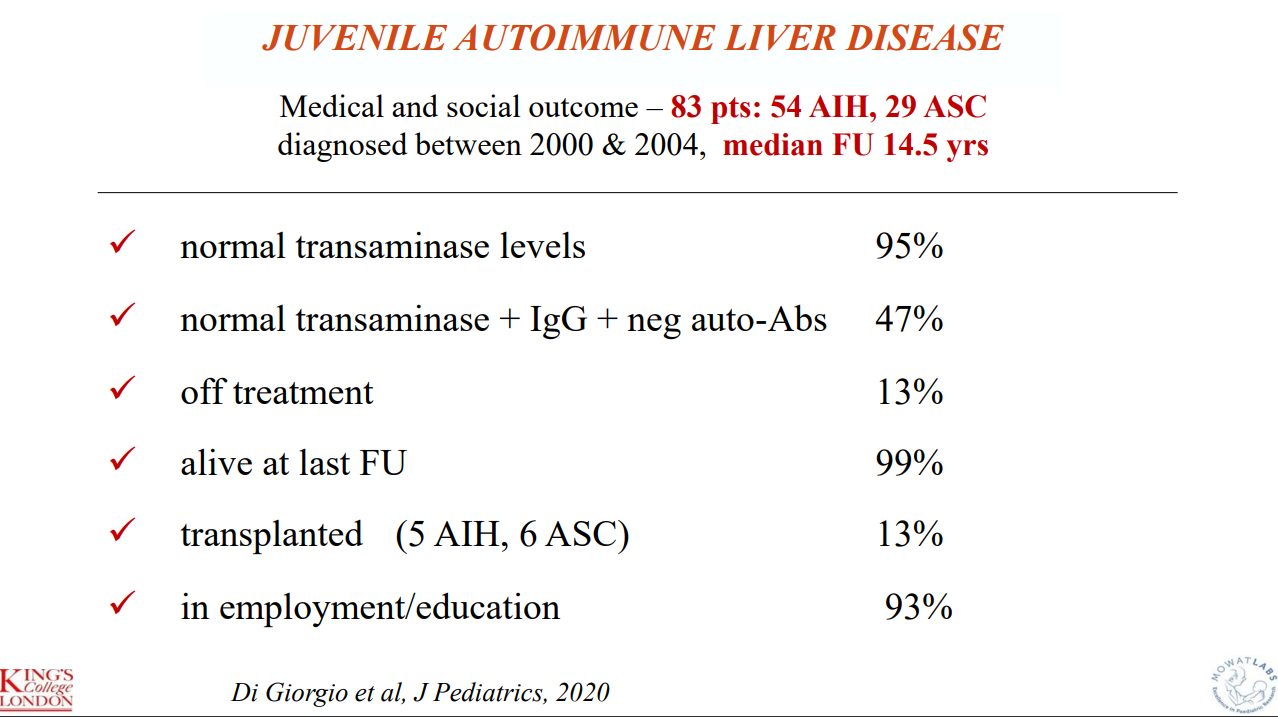
Outcome data indicate that 11 of 83 (13%, 5 AIH, 6 ASC)) required transplantation. “I have shown our long-term outcome data not to stress the number of patients who have required transplantation, but the number of patients who are well and have a normal life after over 14 years of follow-up. This can be only achieved if one thinks of autoimmune liver disease even if the child appears to have something non-specific, initiating correct treatment for the liver, and the gut if there is bowel disease, as soon as possible. At the beginning, treatment should be monitored very closely (at least weekly), to be able to decrease the dose of steroids swiftly, introduce azathioprine if needed, and avoid side affects.”
Key points:
Budesonide is not a good substitute for prednisone in autoimmune hepatitis
Mycophenolate is frequently used as a 2nd line agent
Consider calprotectin in patients with autoimmune liver disease to screen for IBD (though calprotectin can be falsely-negative)
Consider followup liver biopsy after normalization of liver enzymes for ~3 yrs (when consideration of stopping medications)
Recommends MRCP for all patients with AIH
Some slides:
Key points:
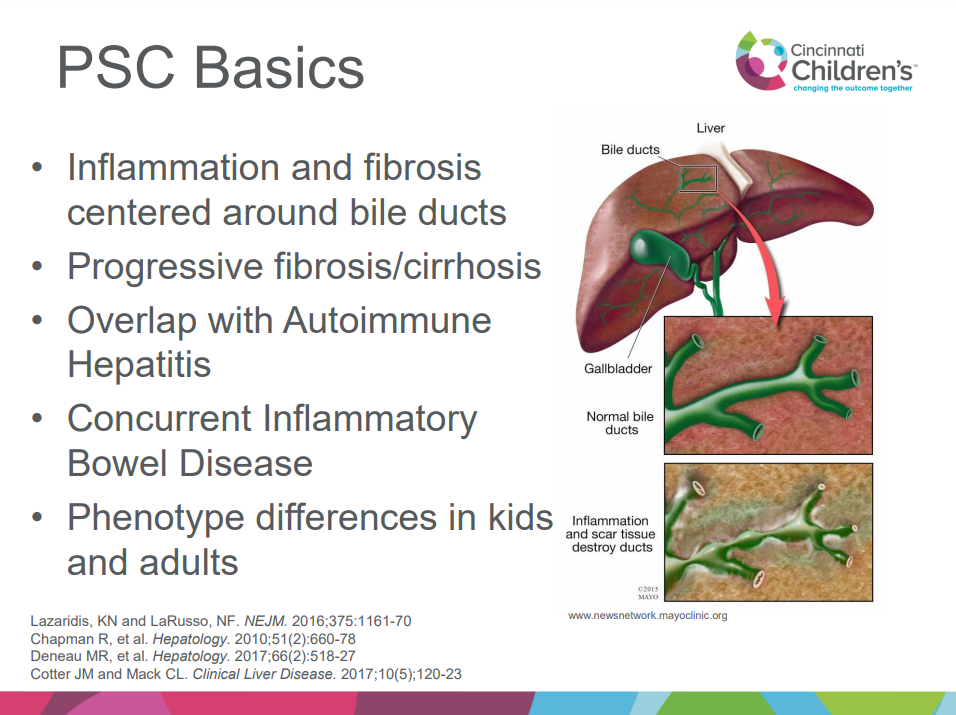
Better understanding of immune basis of PSC is developing
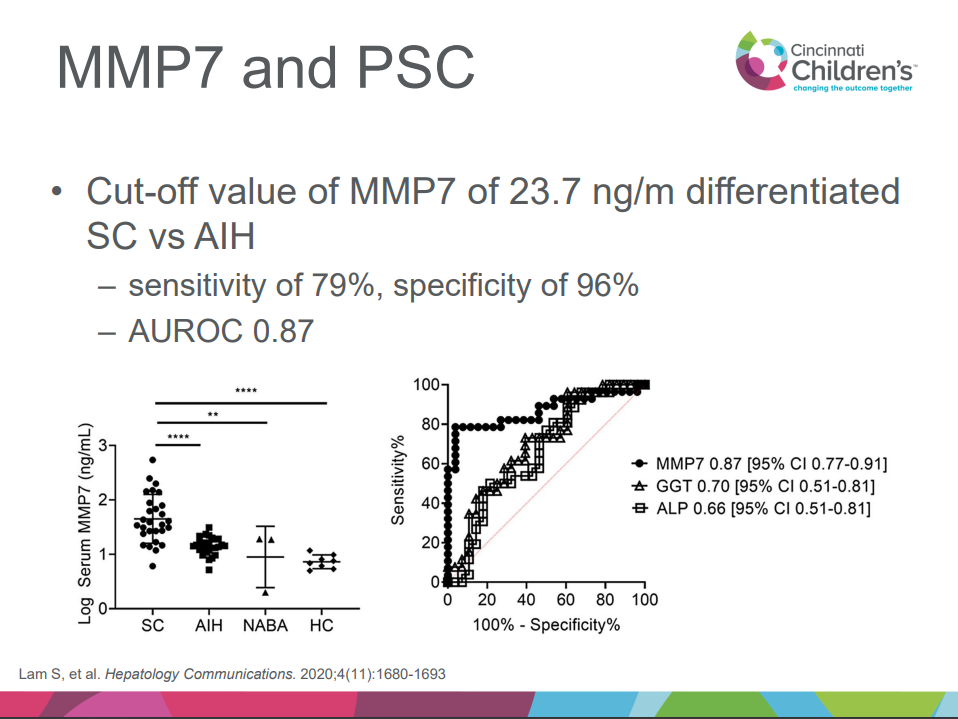
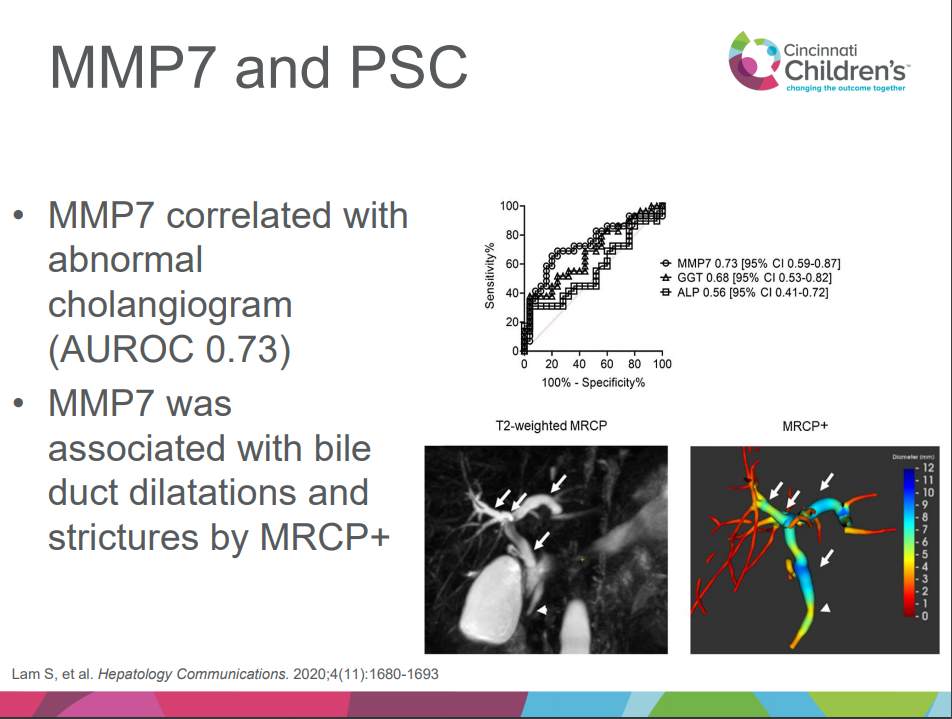
MMP-7 appears to help differentiate PSC/ASC from AIH
Small duct PSC is more common in children
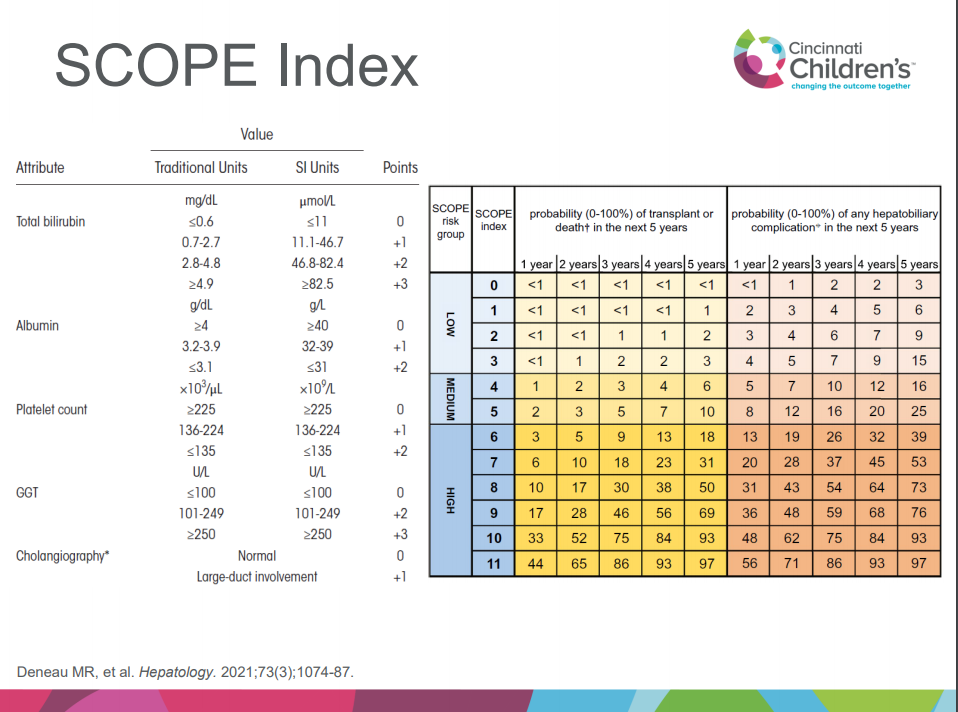
SCOPE index can help predict outcomes
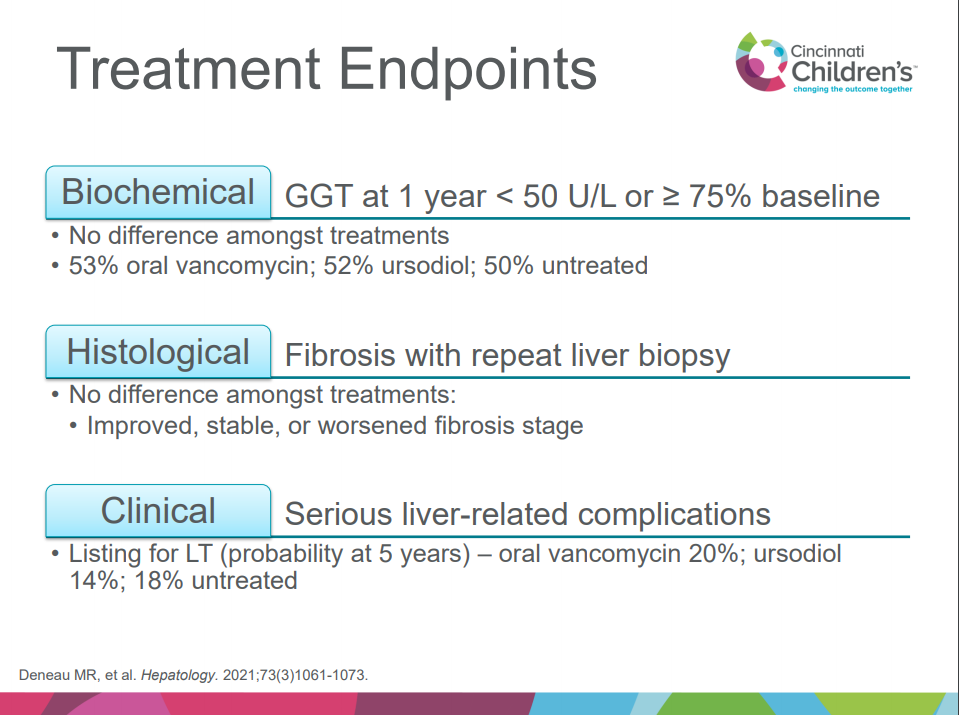
Treatment: no clear benefit of vancomycin, ursodeoxycholic acid compared to placebo but need for randomized controlled study
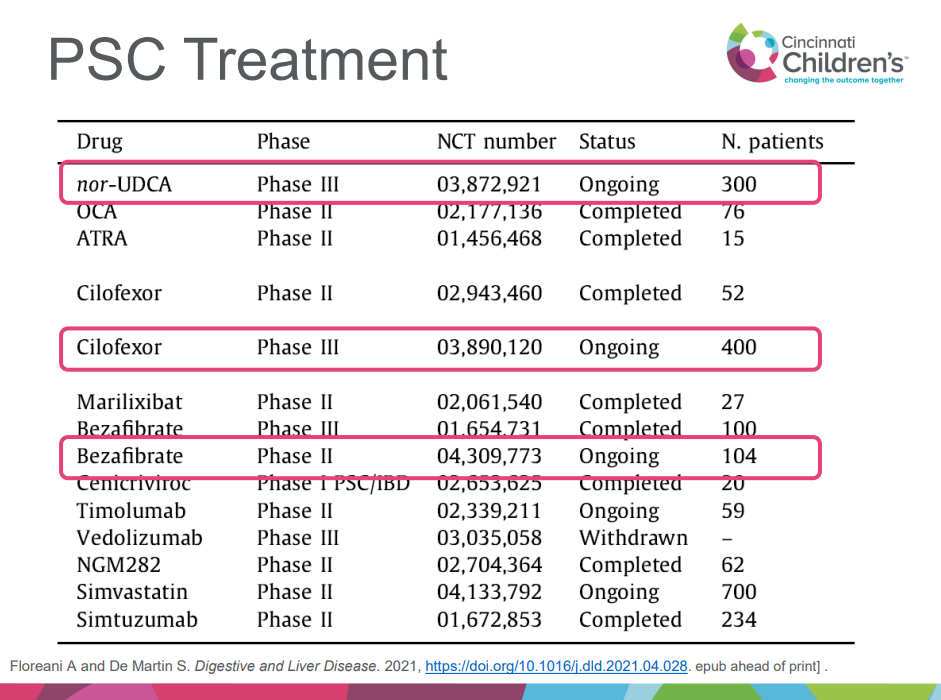
Several studies of new agents for PSC in adults are ongoing, including nor-UDCA, cilofexor, bezafibrate
Vedolizumab does not appear to be effective for PSC
Child with FTT, elevated LFTs, sporadic mild hypoglycemia, and neurologic symptoms. DDx: congenital disorders of glycosylation (CDG), mitochondrial d/o, peroxisomal d/o, urea cycle d/o and lysosomal d/o. Diagnosis was made after liver biopsy and whole exome sequencing (which showed PMM2 mutations). Diagnosis of most CDG can be made by serum transferrin isoforms. Discussion among many participants noted that liver biopsy often not needed in age of genetic testing.
More from Aspen Webinar 2021. This blog entry has abbreviated/summarized several presentations. Though not intentional, some important material is likely to have been omitted; in addition, transcription errors are possible as well. An excellent review from Dr. Sokol.
What’s New with IFALD Ronald Sokol
Key points:
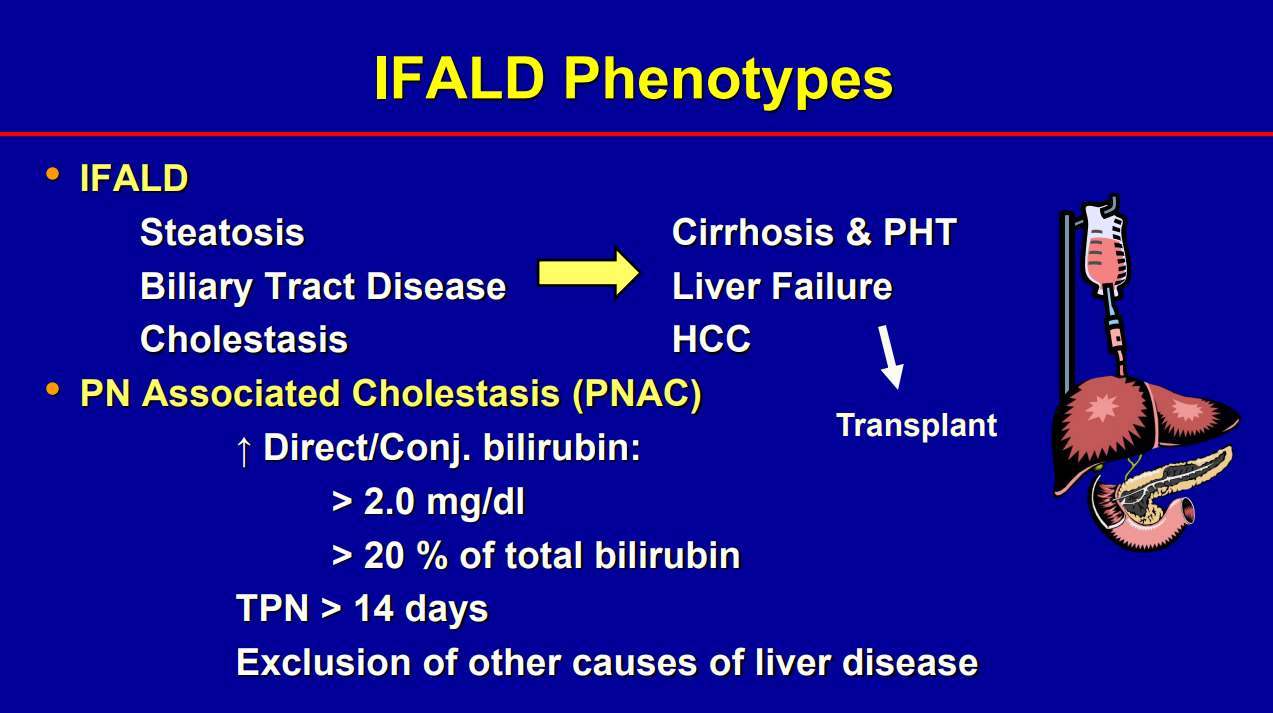
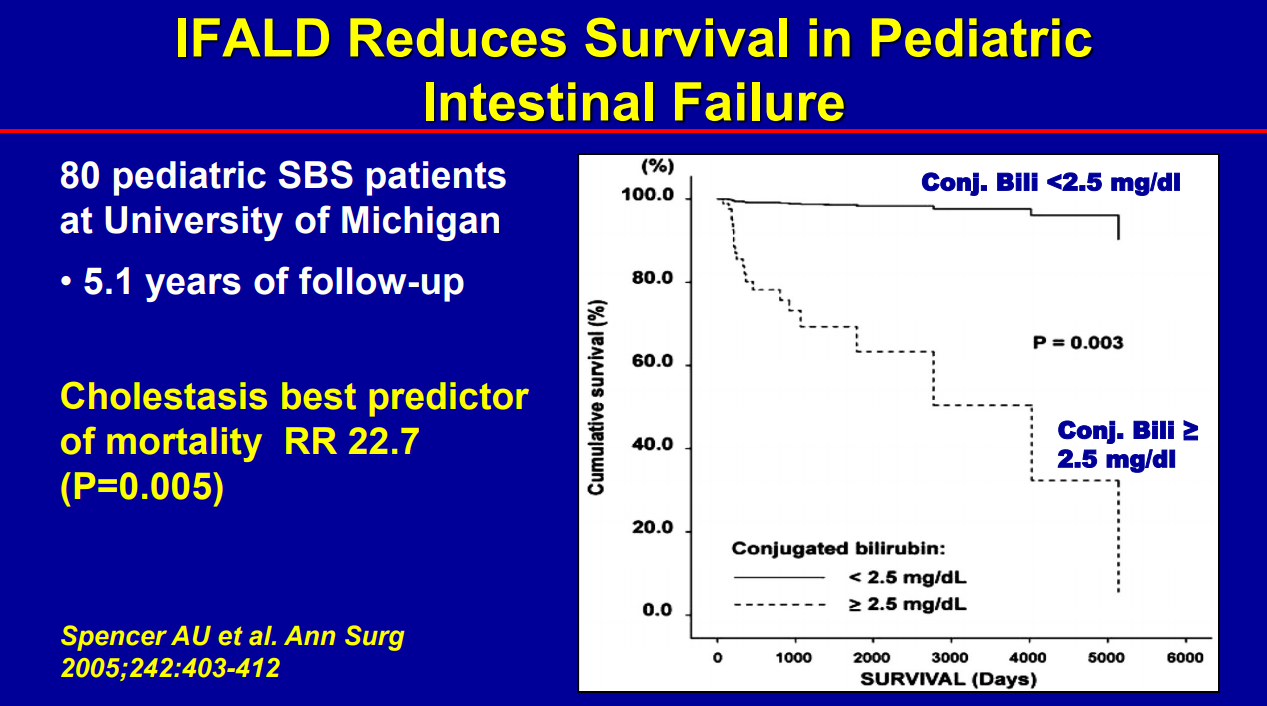
Biliary cirrhosis related to parenteral nutrition has been the major indication for small bowel transplantation/multi-visceral transplantation. IFALD presentations: Steatosis, biliary tract disease and cholestasis
Conjugated bilirubin >2.5 had RR 22.5 for mortality (prior to availability of intestinal transplantation)
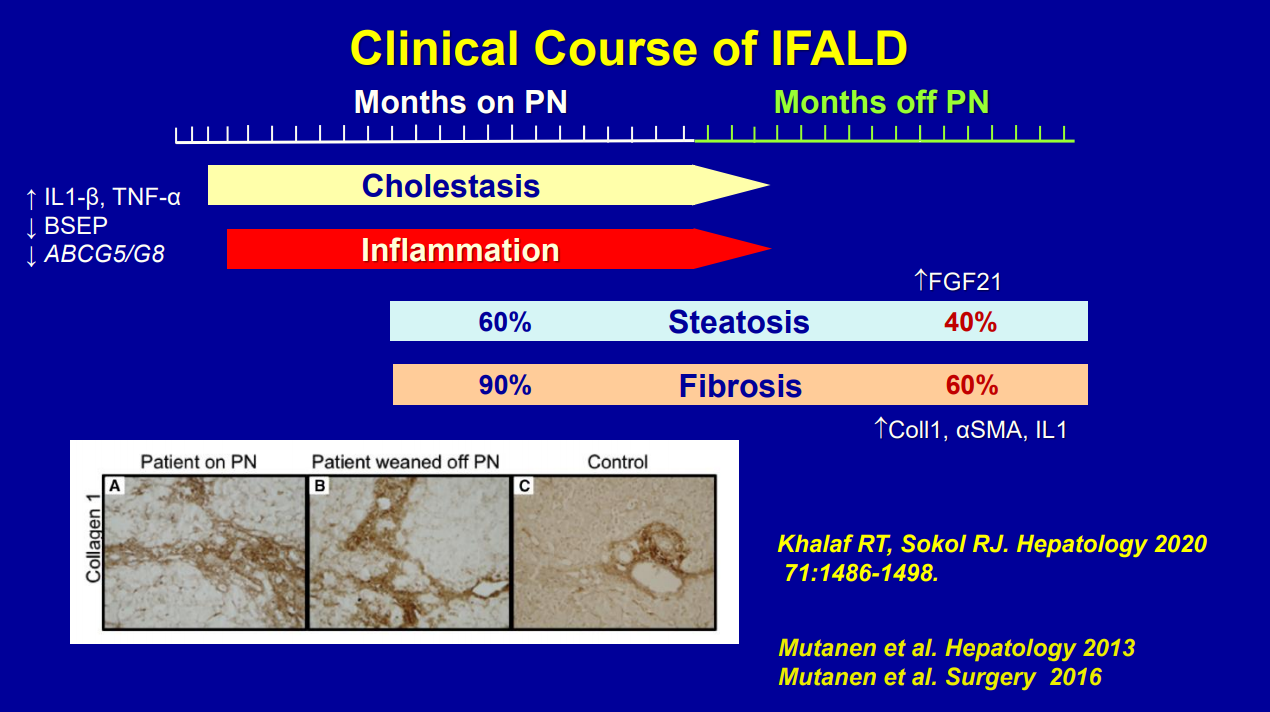
Even after weaning off PN, studies have shown long-lasting fibrosis and steatosis in more than 40% of patients (>8 yrs off PN)
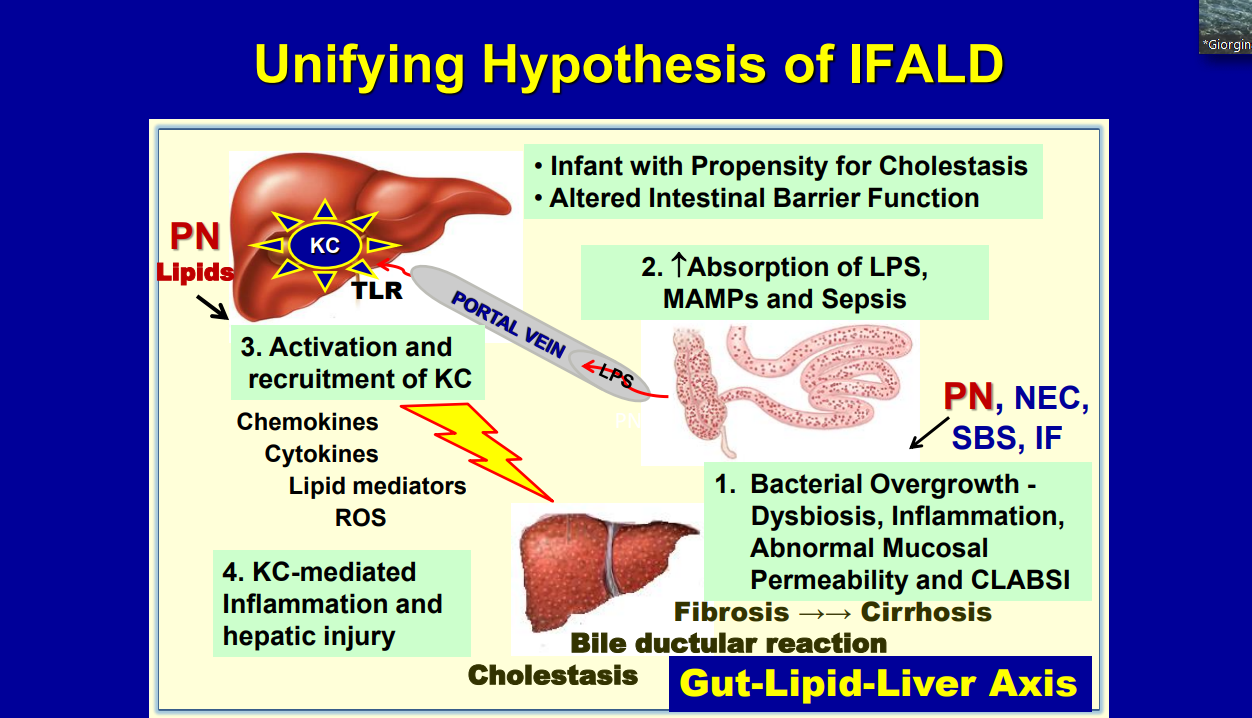
Intestinal microbiome is altered in patients with IFALD
Puder M et al. (Ann Surg 2009; 250: 395) showed that fish oil (at lower doses) was associated with improvement/resolution of parenteral nutrition associated cholestasis (PNAC)
Lipid reduction also is associated with cholestasis resolution
Caution with Fish oil (omegaven): 1. Does not prevent hepatic fibrosis progression 2. Reduction of lipid doses can have negative effects on brain growth
Lipid management has been crucial in reducing the number of children needing intestinal transplantation
Some of the slides:
IBAT Inhibitors Frederick Suchy
Key points:
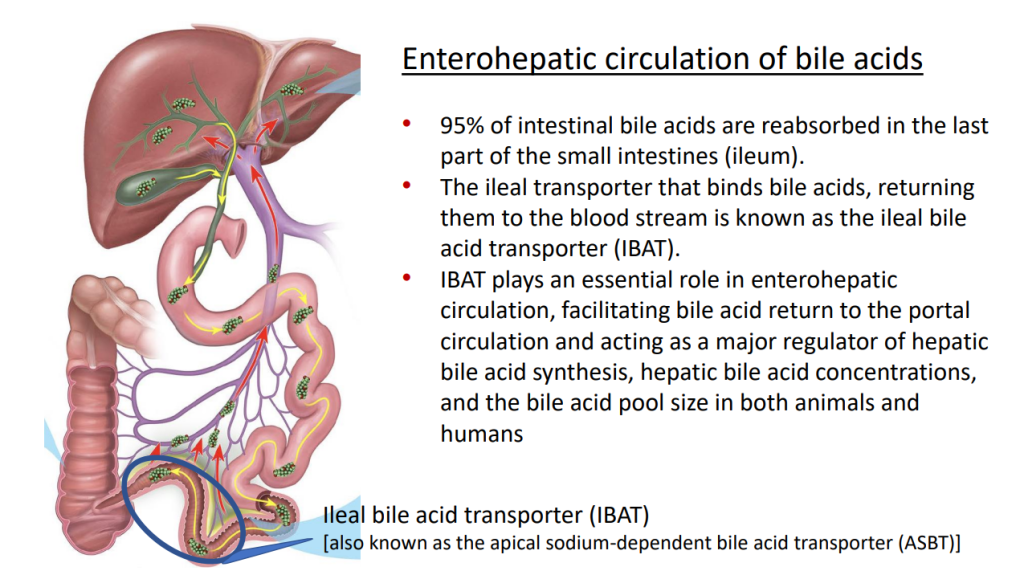
IBAT inhibitors block intestinal absorption of bile acids/disrupt enterohepatic circulation; this leads to augmented bile acid excretion in stools
IBAT inhibitors may reduce liver damage in the setting of cholestasis/accumulation of toxic bile acids
Potential diseases for IBAT inhibitors include Alagille syndrome and PFIC
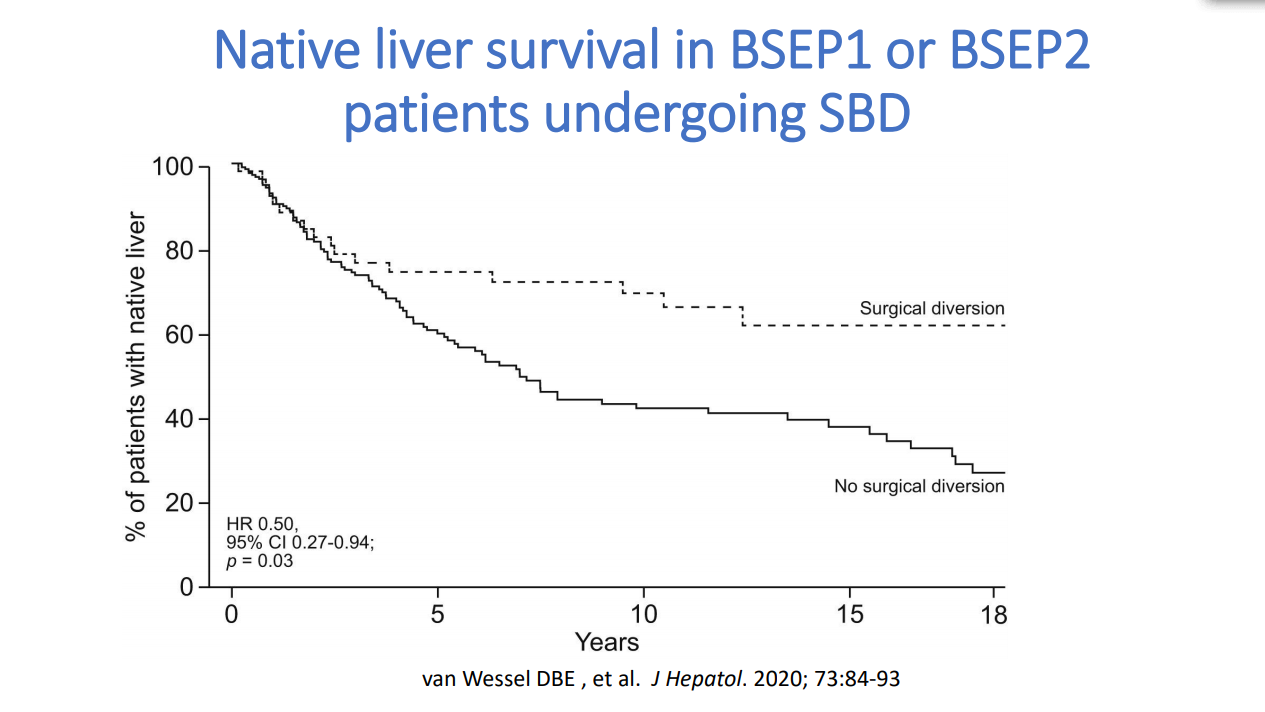
Van Wessel et al (J Hepatol 2020; 73: 84-93) correlated survival with PFIC1/PFIC2 with bile acid levels and showed improvement in survival in those with surgical biliary diversion
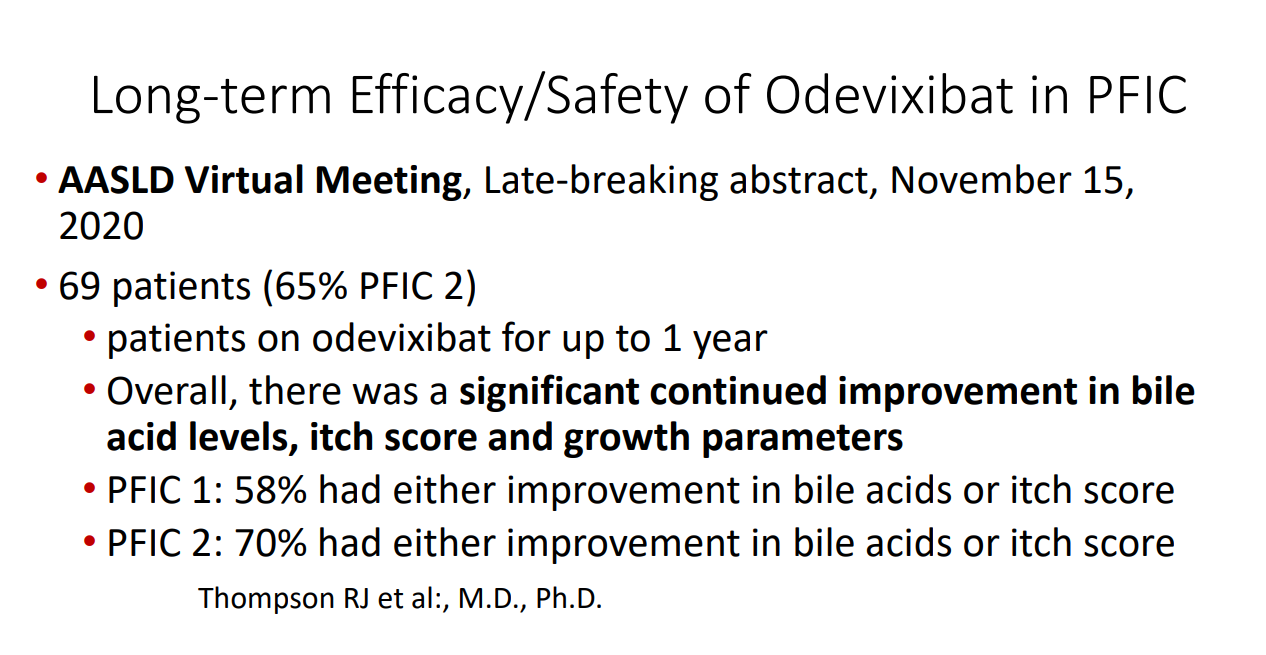
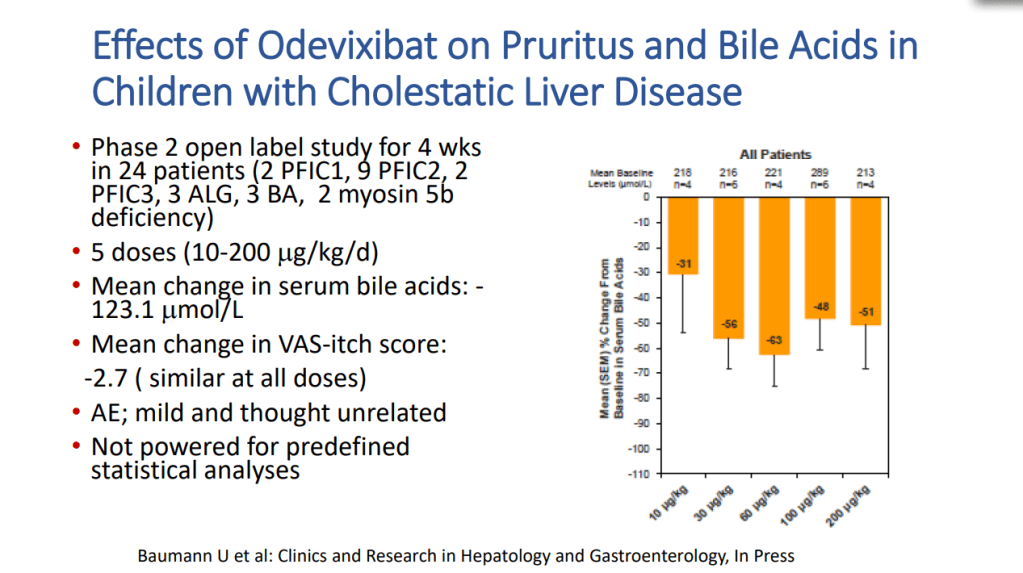
Goals for IBAT inhibitor trials: improvement in pruritus, bile acids, reduced ALT, hepatic fibrosis, HCC and need for liver transplantation
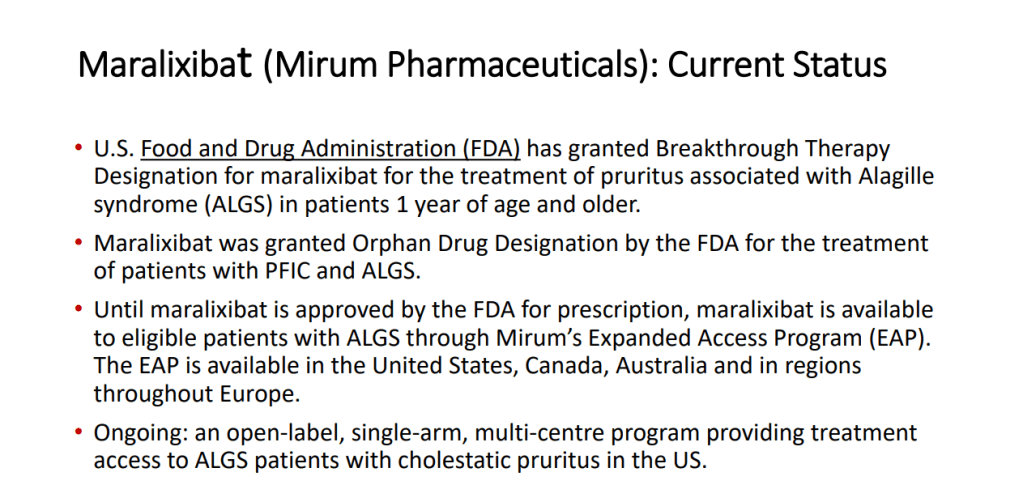
Marixibat is available for use as an FDA approved breakthrough medication for Alagille and PFIC2 in pediatric patients older than 1 year
Odexibat is designated as an orphan drug for Alagille, PFIC, PBC, and biliary atresia
Safety appears good with IBAT inhibitors. Fat soluble vitamin monitoring is needed
Case report: Alejandro Velez Lopez
3 yo presented with fatigue and jaundice, 3 weeks after COVID-19 infection. She was not taking any medications. Labs: ALT 939, AST 1321, T bili 5.5, D bili 0.9, INR 2, Plts 174, Hgb 12.8, LDH 1297. remained positive for SARS-CoV2 by PCR. Acetaminophen -no exposure. Evaluation: LKM 1:1280. Neg ANA, NL Ferritin, NL sIL2r, Other viral studies negative, NL IgG. Developed encephalopathy with NH4 317, INR peaked at 2.8. Treated with steroids, rifaximin and lactulose. Liver biopsy showed sub-massive necrosis and fibrosis (indicative of autoimmune hepatitis, likely triggered or exacerbated by COVID-19). Patient responded to medical therapy and did not require liver transplantation.
This blog entry has abbreviated/summarized this presentation. Though not intentional, some important material is likely to have been omitted; in addition, transcription errors are possible as well. Another great lecture from Dr. Suchy.
IBAT Inhibitors Frederick Suchy
Key points:
IBAT inhibitors block intestinal absorption of bile acids/disrupt enterohepatic circulation; this leads to augmented bile acid excretion in stools
IBAT inhibitors may reduce liver damage in the setting of cholestasis/accumulation of toxic bile acids
Potential diseases for IBAT inhibitors include Alagille syndrome and PFIC
Van Wessel et al (J Hepatol 2020; 73: 84-93) correlated survival with PFIC1/PFIC2 with bile acid levels and showed improvement in survival in those with surgical biliary diversion
Goals for IBAT inhibitor trials: improvement in pruritus, bile acids, reduced ALT, hepatic fibrosis, HCC and need for liver transplantation
Marixibat is available for use as an FDA approved breakthrough medication for Alagille and PFIC2 in pediatric patients older than 1 year
Odexibat is designated as an orphan drug for Alagille, PFIC, PBC, and biliary atresia
Safety appears good with IBAT inhibitors. Fat soluble vitamin monitoring is needed
3 yo presented with fatigue and jaundice, 3 weeks after COVID-19 infection. She was not taking any medications. Labs: ALT 939, AST 1321, T bili 5.5, D bili 0.9, INR 2, Plts 174, Hgb 12.8, LDH 1297. remained positive for SARS-CoV2 by PCR. Acetaminophen -no exposure. Evaluation: LKM 1:1280. Neg ANA, NL Ferritin, NL sIL2r, Other viral studies negative, NL IgG. Developed encephalopathy with NH4 317, INR peaked at 2.8. Treated with steroids, rifaximin and lactulose. Liver biopsy showed sub-massive necrosis and fibrosis (indicative of autoimmune hepatitis, likely triggered or exacerbated by COVID-19). Patient responded to medical therapy and did not require liver transplantation.
From the 2nd lecture of the Aspen Webinar. This blog entry has abbreviated/summarized this presentation. Though not intentional, some important material is likely to have been omitted; in addition, transcription errors are possible as well. This was a terrific lecture!
NASH Update Stavra Xanthakos
Key points:
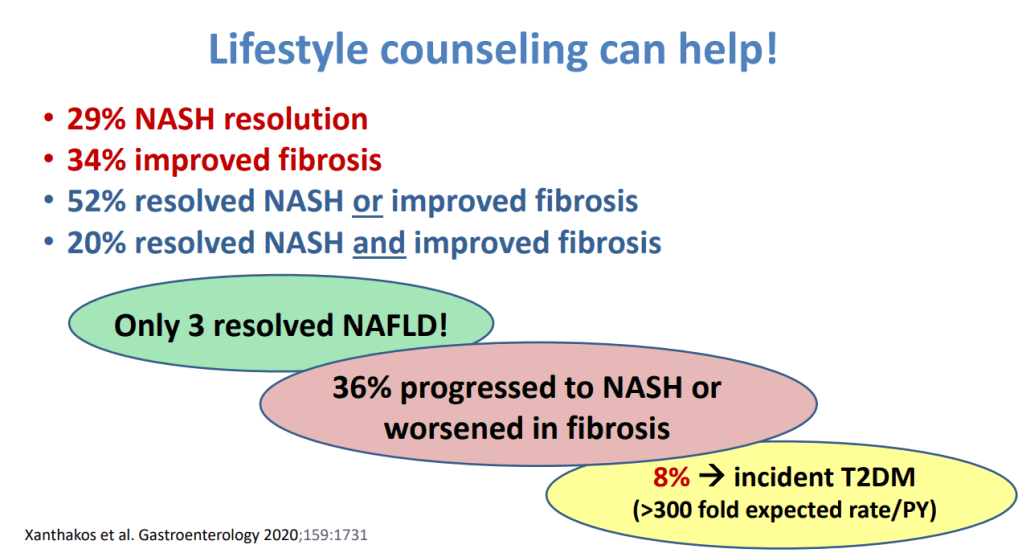
Lifestyle intervention is 1st line Rx (especially avoiding sugary beverages, and processed foods). This may lead to resolution of NASH in ~29%, fibrosis resolution in 34%; though, only 3% resolved fatty liver
Many have progressive disease despite lifestyle treatment recommendations
Consider adjunctive treatments if not improving with lifestyle intervention
Vitamin E for biopsy-confirmed disease (often for 1-2 years of therapy)
Pioglitazone -off-label for adults (18+). Can increase weight; a lot of trials in adults
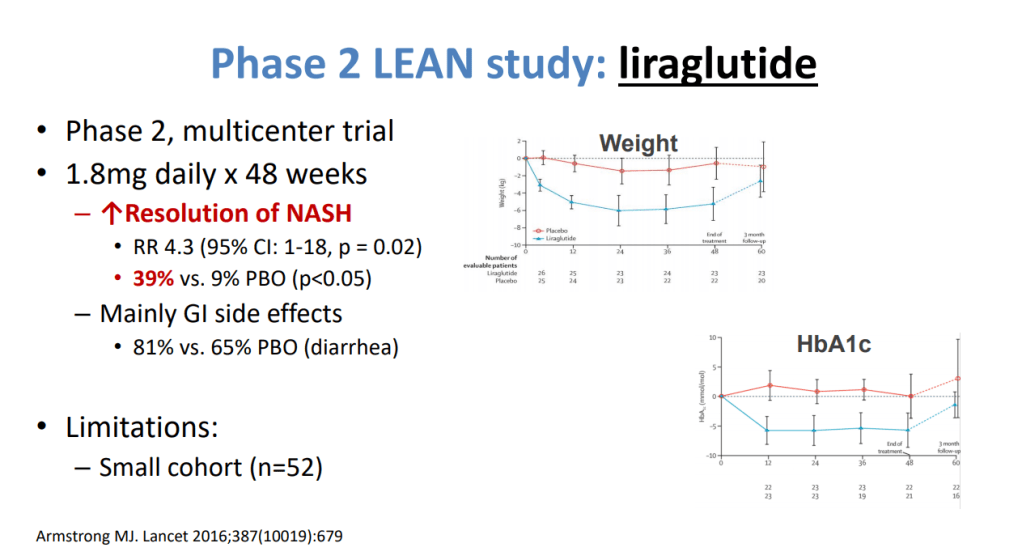
Several phase 3 trials in NASH -GLP1 agonists promising in phase 2 trials
GLP1 agents being used in adolescents with T2DM who may also have NASH – monitor liver outcomes
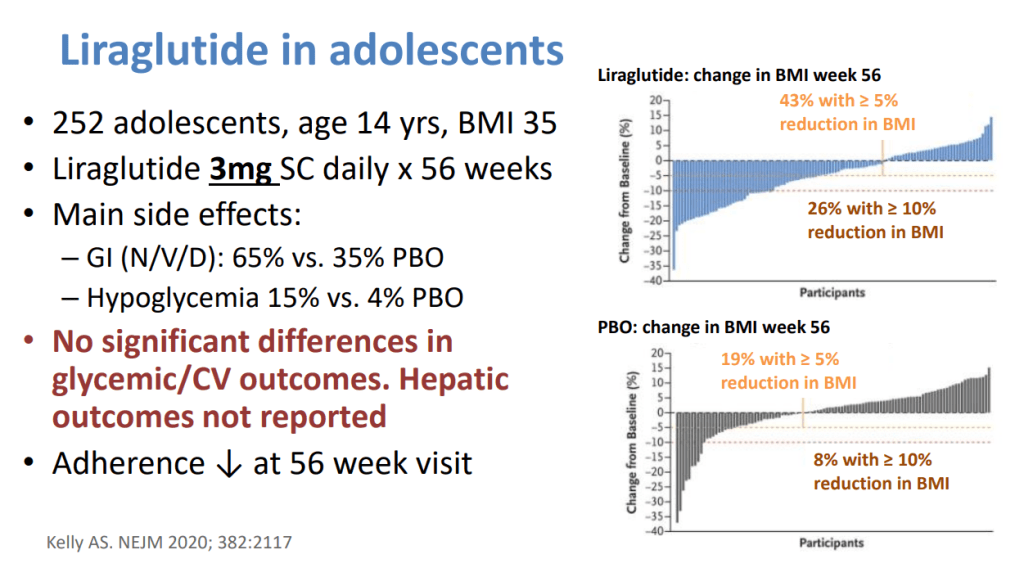
Anti-obesity medications may help with weight and perhaps the liver. Approved agents for adolescents include 1) Orlistat -safe, but frequent side effects (eg. Diarrhea, greasy accidents) and 2) Liraglutide -daily SC. Insurance coverage is limited.
Biopsy is important before implementing medications and may influence decision to pursue bariatric surgery.
Fibroscan, if shows no significant fibrosis, can help limit biopsy.