I recently had the opportunity to review the topic of neonatal cholestasis with my neonatal colleagues. I reviewed two related conditions: parenteral nutrition associated liver disease (PNALD) and neonatal acute liver failure (NALF). Some of the material incorporates recommendations from NASPGHAN cholestasis guidelines and from NASPGHAN cholestasis slidesets. Much of the slideset information is publicly available on a YouTube lecture by Dr. Linda Book (link at bottom).
Full lecture: Neonatal Cholestasis for Neonatologists
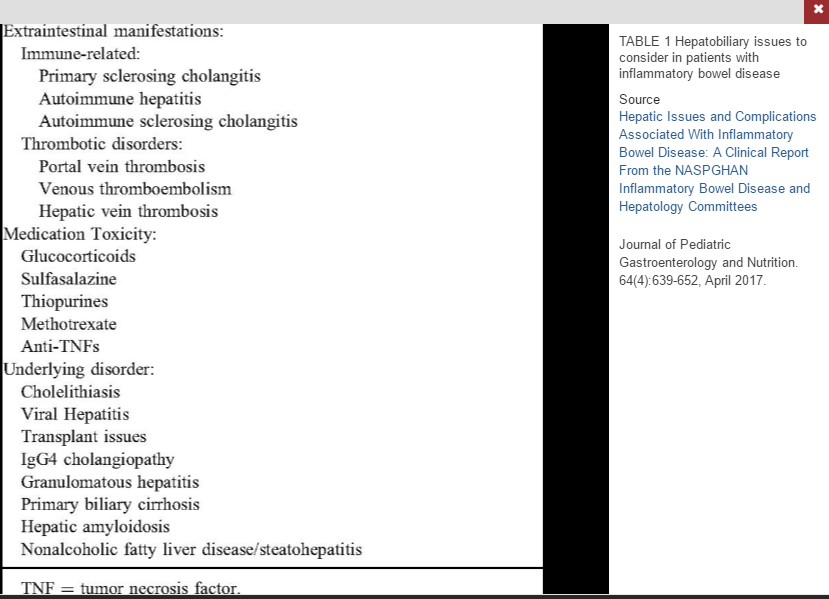
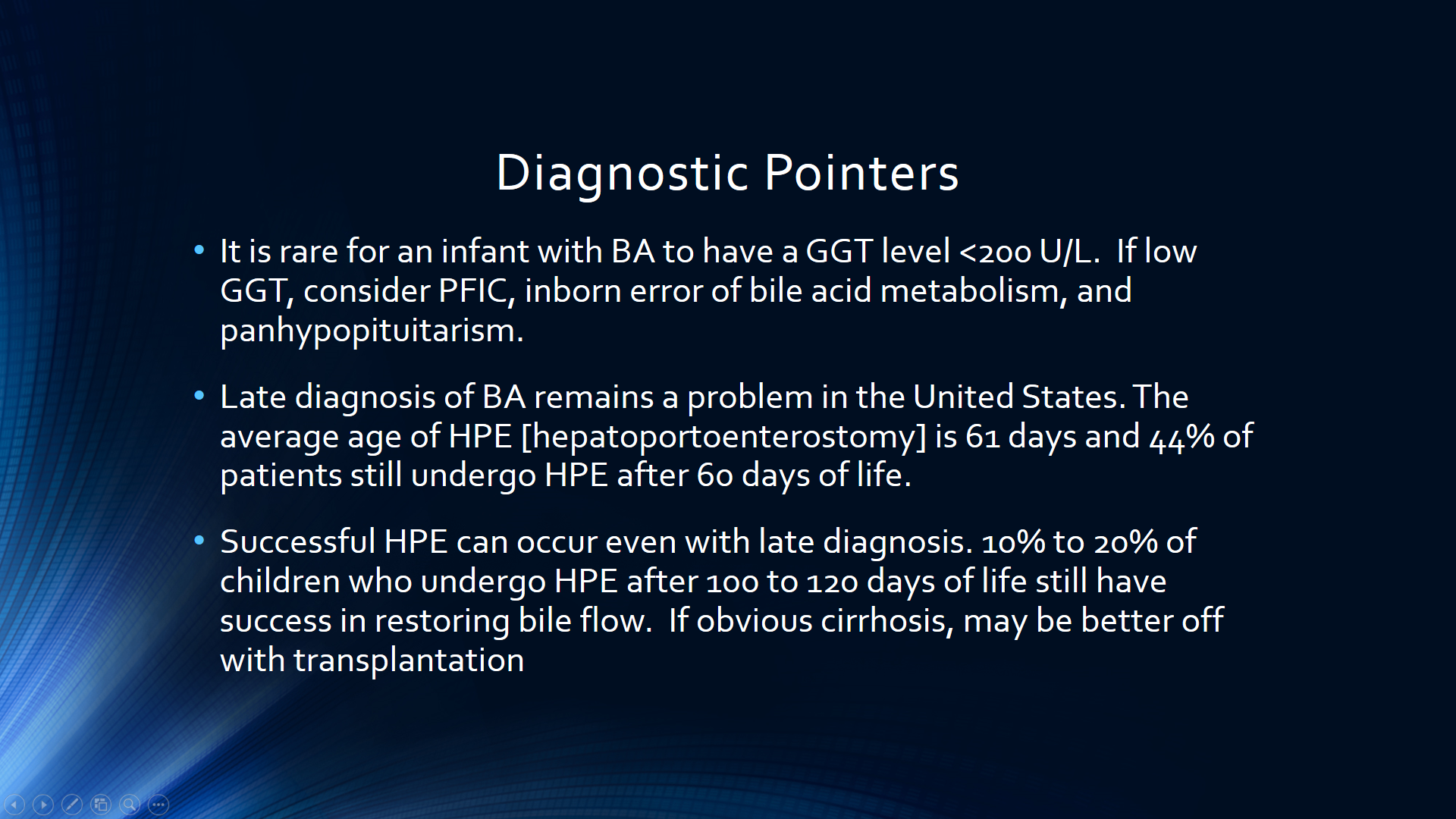
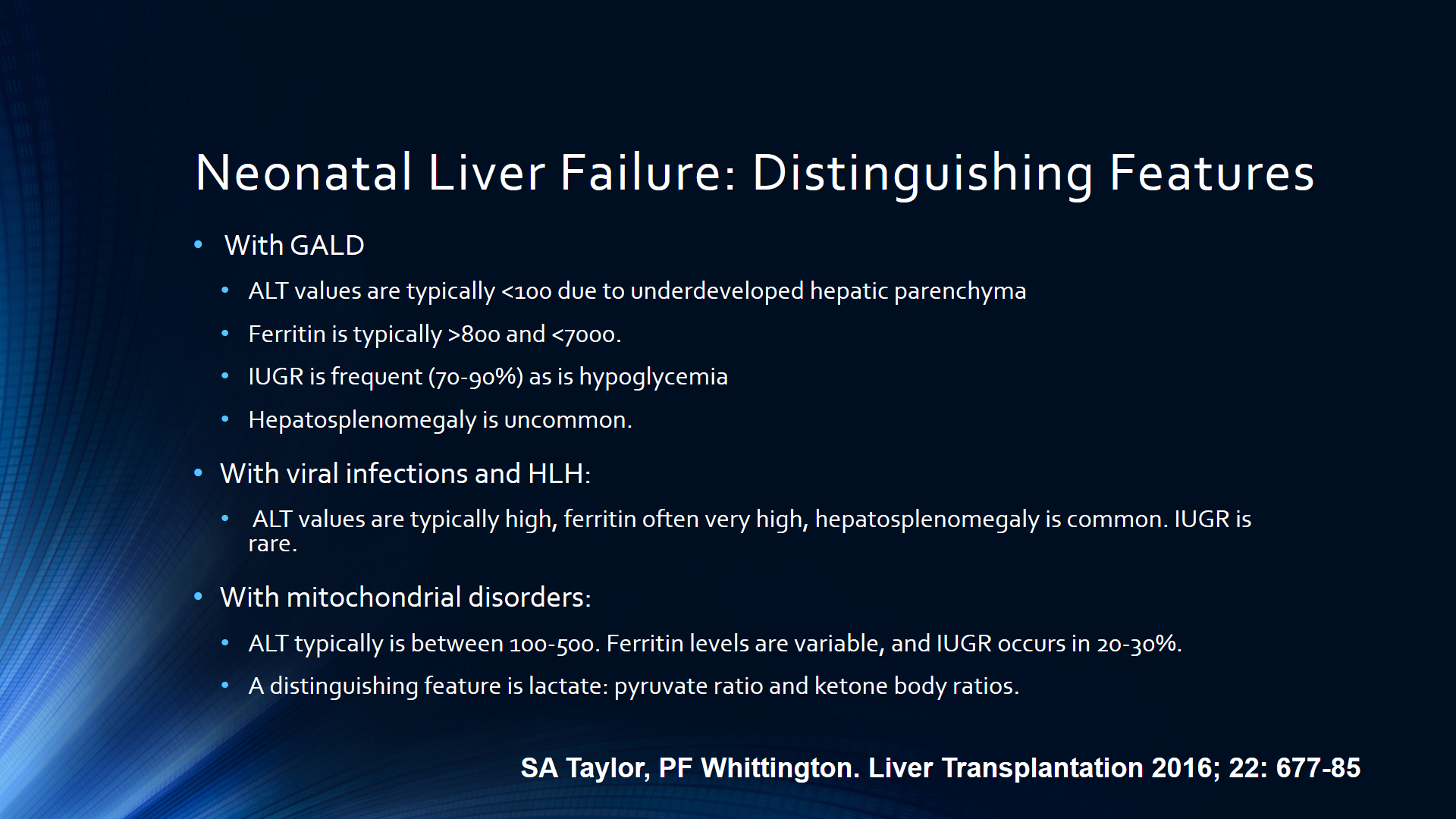
Some screenshots:






Related blog posts:
- Guideline links for TEF and Infant Cholestasis
- Neonatal Cholestasis Lecture
- Diagnosing biliary atresia earlier | gutsandgrowth
- Helpful Review on Biliary Atresia | gutsandgrowth
Disclaimer: These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.