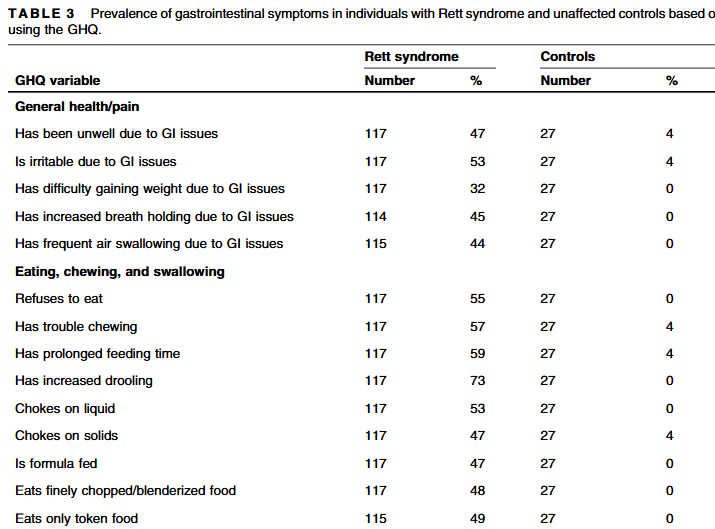
FD Ihekweazu, KJ Motil. J Pediatr Gastroenterol Nutr. 2025;80:46–56. Gastrointestinal manifestations of Rett syndrome: An updated analysis using the Gastrointestinal Health Questionnaire
Methods: Parents of 118 females with Rett syndrome (RTT) and 27 unaffected females completed the GHQ.
Key findings:
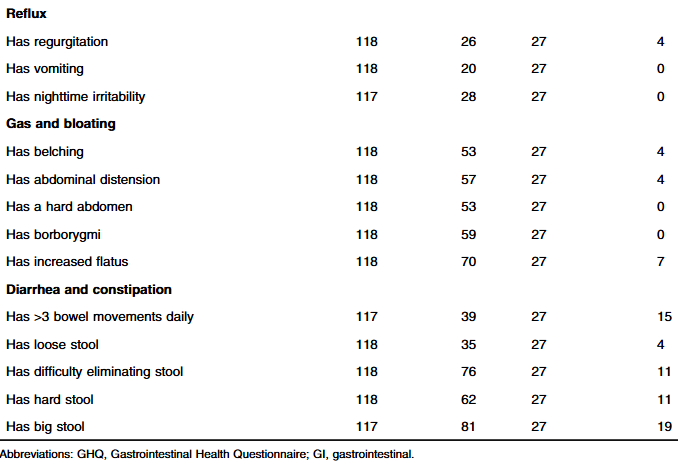
GI symptoms were common in females with RTT, including constipation (81%), gas and bloating (70%), issues with eating, chewing and swallowing (73%), and irritability because of stomach or intestinal problems (53%).
Females with RTT commonly used proton pump inhibitors (52%) and laxatives (64%).
All with p values of <0.001 with the exception of has >3 BM/day which had p value of 0.004
My take: “GI problems are common in RTT and pose a significant medical burden to caregivers.” As such, it is a good idea to screen for treatable disorders including swallow dysfunction, constipation, and reflux.
For a lot of patients with rheumatologic complaints like joint pain, treatment often consists of sending patients to physical therapy rather than using pharmaceuticals. This type of approach is under-utilized in gastroenterology. A recent study, however, suggests that an analogous approach is likely beneficial in patients with chronic laryngopharyngeal symptoms.
Background: Laryngopharyngeal symptoms such as cough, throat clearing, voice change, paradoxic vocal fold movement, or laryngospasm are hyper-responsive behaviors resulting from local irritation (e.g., refluxate) and heightened sympathetic tone. Laryngeal recalibration therapy (LRT) guided by a speech-language pathologist (SLP) provides mechanical desensitization and cognitive recalibration to suppress hyper-responsive laryngeal patterns.
Methods: Adults (n=65, mean age 55 years) with chronic laryngopharyngeal symptoms referred for evaluation of GERD to a single center were prospectively followed. Inclusion criteria included ≥2 SLP-directed LRT sessions (60 minutes sessions). “Mechanical desensitization focuses on well-known laryngeal suppression techniques (i.e. pursed lip breathing to suppress throat clearing or cough) or changing voice production by means of acoustic and aerodynamic techniques…Cognitive recalibration uses relaxation and conceptualization of symptoms to rework thought patterns around chronic laryngeal behaviors.”
Key findings:
Overall, 55 participants (85%) met criteria for symptom response. 17 (26%) had complete resolution, 19 (29%) had near-complete resolution, and 19 (29%) had a moderate response
Specifically, symptom response was similar between those with isolated laryngopharyngeal symptoms (13/15, 87%) and concomitant laryngopharyngeal/esophageal symptoms (42/50, 84%)
My take: Historically, patients with laryngopharyngeal symptoms have been difficult to treat. Many do not respond to reflux therapies. This study highlights a different approach and shows that the benefit of working with highly-skilled SLPs.
J Fritz et al. J Pediatr Gastroenterol Nutr. 2025;80:100–107. The relationship between adverse childhood experiences and disorders of the gut–brain interaction
Methods: Retrospective review of patients aged 3–18 years with ACE scores documented between October 1, 2019 and April 30, 2022. from two large primary care medical groups in Southern Maine within the MaineHealth system. ACE screening tool was taken at a routine WCC at a primary care office. From these patients, we identified from the medical record whether patients were referred to a general pediatric GI clinic in Southern Maine.
Key findings:
Four hundred and one (44.7%) were diagnosed with a DGBI.
With each additional adverse experience, patients were 1.09 times more likely to have a DGBI diagnosis (p ≤ 0.001). An anxiety diagnosis mediated 73% of this relationship (p = 0.012).
Limitations:
There are many limitations to this study. The vast majority of patients with DGBIs were likely never referred to a pediatric GI clinic. While anxiety was found to mediate the relationship between ACEs and DGBIs, perhaps an alternative explanation was that anxiety increased the likelihood of GI referral. In addition, the authors note that” patients who are perceived as anxious by their gastroenterologist are more likely to receive a DGBI diagnosis.27 The nature of a symptom-based diagnosis for DGBI was also a limitation as not all patients had sufficient documentation to apply Rome criteria for inclusion.”
My take: Despite the limitations of this study, it appears that ACEs are associated with DGBIs mediated mainly by anxiety.
Screen for thyroid disease and celiac disease (though acknowledges that the data regarding an association between celiac disease and constipation are inconsistent)
The use of an AXR in RC should be reserved for those patients unable to provide a reliable medical history and/or unable to allow for a physical exam (including a DRE), or to evaluate for mechanical obstruction or colonic distention when considering surgical interventions
A contrast enema (CE) can be used to screen for HD or to assess colorectal anatomy
There is no evidence to recommend the routine use of defecography in children
Abdominal ultrasound has a good agreement with digital rectal exam (DRE) to evaluate for fecal impaction but should not be performed in place of DRE
ARM should be used to screen for the presence of a RAIR. If anal spasms and prolonged sphincter relaxation are detected during ARM, an assessment for spinal abnormalities can be considered
An LS MRI should be performed in pediatric patients with RC associated with physical or neurological signs of spinal anomalies, signs of neurogenic bladder on urodynamics, or when the anorectal manometry (ARM) is abnormal suggesting spinal cord abnormalities
Colonic transit time (CTT) via radiopaque markers should be completed for patients with RC with equivocal medical history and to screen for the need to perform colonic manometry (CM)
Colonic manometry (CM) should be performed only after medical therapy has been exhausted and surgical therapy is being considered. CM should be used to guide the timing and type of surgery to address RC. CM should be used to guide when to perform an ostomy takedown
Rectal biopsies should not be used routinely in patients with RC and are indicated exclusively in patients with a suspected diagnosis of HD
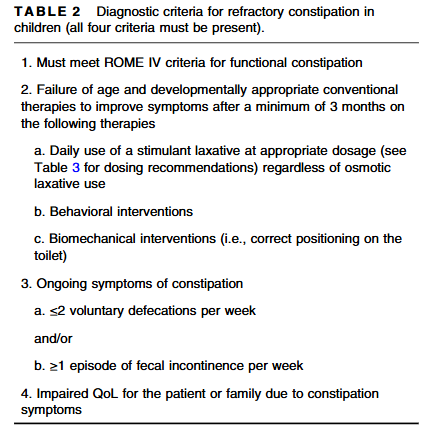
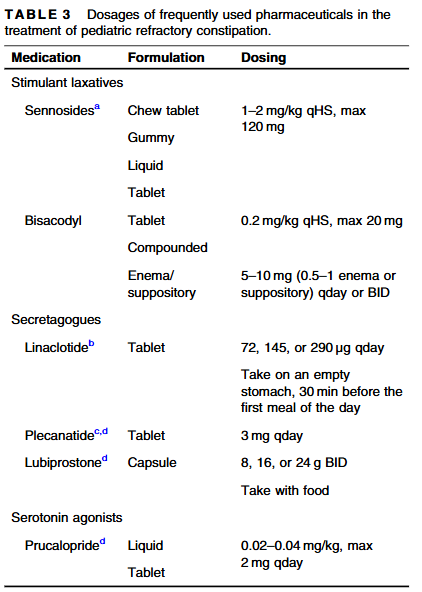
Pharmaceuticals:
High-dose sennoside (or Bisacodyl) is a mainstay of management of RC and should be optimized for the individual patient before considering further management options
A secretagogue (or prucalopride) should be considered as an adjunct to a high-dose stimulant laxative when treating RC with poor response to optimized high-dose stimulant laxatives or when high-dose stimulant laxatives are not tolerated
There is no clear role of anal botox in the treatment of patients with RC without a diagnosis of IAS achalasia
Early intervention with daily stimulant laxatives in the treatment of FC is encouraged to try to prevent the disease progression from functional constipation (FC) to RC
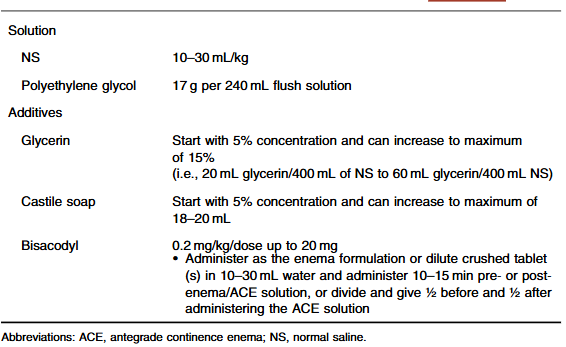
Antegrade and Retrograde Treatments:
Routine dosages of frequently used antegrade and retrograde solutions and additives
The last part of the recommendations include antegrade continence enemas, surgical approaches, and complicated algorithms (see Figure 1 and Figure 2)
My take: These recommendations address a widespread problem for pediatric gastroenterologists and are useful for those with and without an interest in motility disorders.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
PF van Rheenen et al. JPGN 2024; DOI: 10.1002/jpn3.12378. Open Access! Primary sclerosing cholangitis in children with inflammatory bowel disease: An ESPGHAN position paper from the Hepatology Committee and the IBD Porto group
Recommendations:
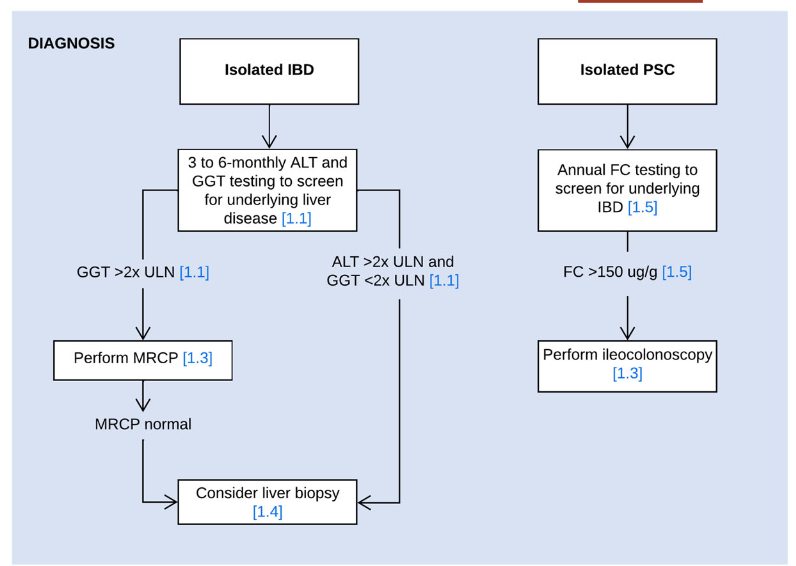
In children with suspected or confirmed IBD, screening for liver disease is usually performed at 3 to 6 months intervals and a work‐up for underlying liver disease is most commonly initiated when liver enzymes exceed 2x the upper limit of normal
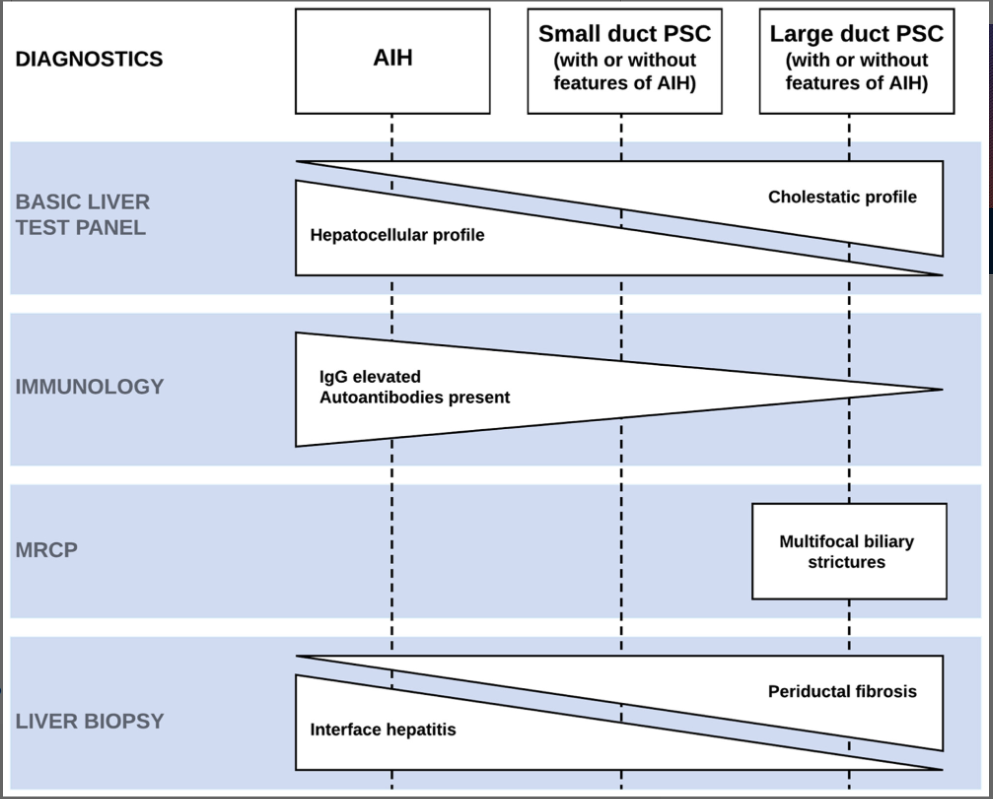
Use MRCP as the radiological modality of choice for diagnosing PSC
Consider performing a liver biopsy in children with IBD and suspected PSC in the following circumstances: i) Normal biliary tree at MRCP, ii) raised immunoglobulin G and the presence of liver-specific autoantibodies, or iii) clinical uncertainty before steroid induction therapy for IBD
Perform fecal calprotectin screening at least once yearly in children with isolated PSC and/or AIH to select patients for diagnostic endoscopy for suspected inflammatory bowel disease (panel recommends cutoff of >150 indicating need for ileocolonoscopy)
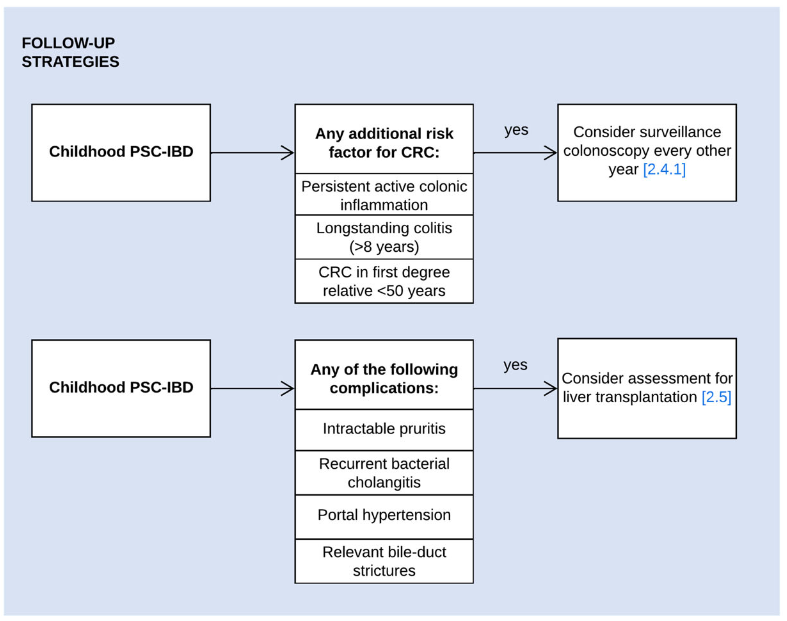
Surveillance colonoscopy should be considered in children with PSC–IBD and the following risk factors of colorectal cancer: i) persistent active colonic inflammation, ii) longstanding colitis (≥8 years), or iii) a family history of colorectal cancer in a first-degree relative <50 years. (The overall risk of colon cancer in those <18 yrs of age is very low)
UDCA may be prescribed at doses of 15–20 mg/kg/day. Despite evidence of improvement of liver enzymes, its long-term effect on disease progression has not been demonstrated. Consider a 6-months therapeutic trial of UDCA, either immediately after PSC diagnosis or when spontaneous normalization of GGT does not occur in the first 6 months postdiagnosis. Continue UDCA treatment if there is a meaningful reduction or normalization of GGT or improvement of symptoms
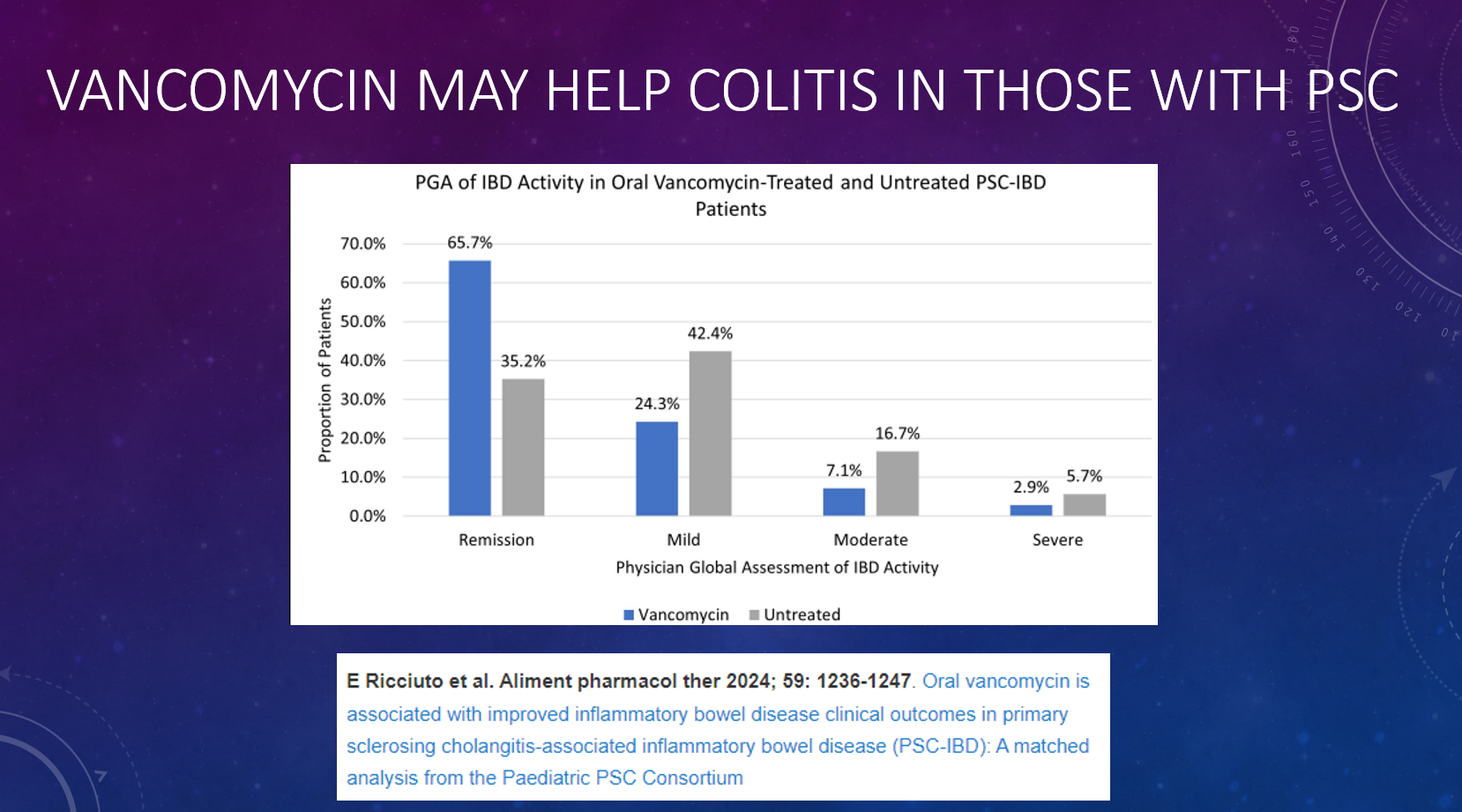
Oral vancomycin may be prescribed for a potential improvement in liver biochemistry as well as bowel inflammation. Its long-term effect on disease progression has not been demonstrated
In children with PSC–IBD and biochemical, serological, and histological features of AIH, the use of corticosteroids and antimetabolites may suppress immune-mediated hepatitis. In the absence of convincing AIH features, the use of corticosteroids and antimetabolites is not indicated to manage PSC
Children with PSC, relevant bile-duct strictures and cholestatic symptoms should be assessed for liver transplantation. When their symptoms are likely to improve following biliary intervention, ERCP can be considered
Recommended blood testing for children with PSC: At diagnosis: Autoantibodies (ANA, anti-SMA, anti-LKM-1, anti-LC1, and anti-SLA), Every 3-6 months: ALT, AST, GGT, Albumin, INR, Platelets, CRP. Every 12 months: IgG, AFP, and Fat Soluble vitamins. Consider f/u autoantibodies in those with elevated IgG at f/u lab testing
My take: This is a useful position paper; it does not have a zillion recommendations like some other ESPGHAN positions papers. Given the frequency of liver enzyme elevation in patients with IBD, mild to modest elevations may need to be observed before launching an extensive evaluation (see related blog posts below).
Aspen Webinar 2021 Part 5 -Autoimmune Liver Disease & PSC 2021. This lecture highlights studies show lack of efficacy with vancomycin, ursodeoxycholic acid and vedolizumab in altering the liver disease. Also, there is potential utility of MMP-7 for distinguishing between PSC and AIH
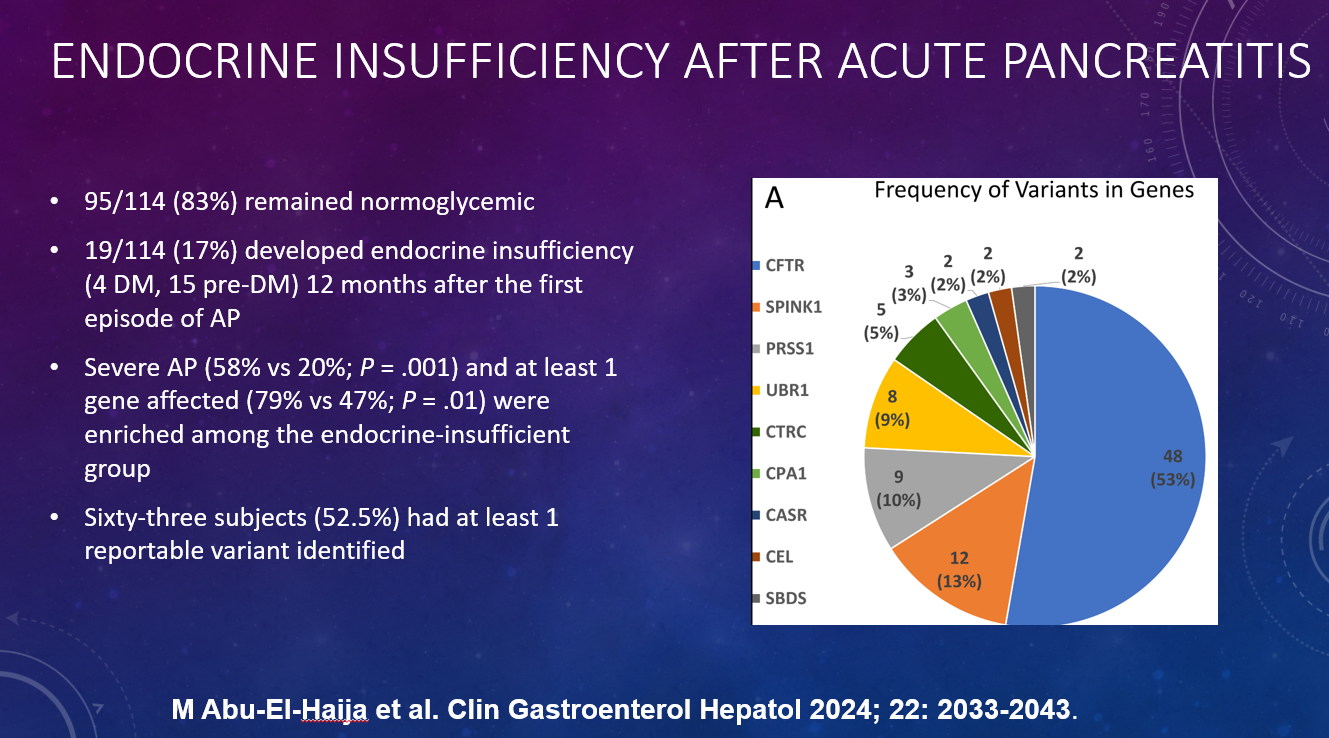
This single-center retrospective study with 227 patients (2013-2023) examined the role of liberal fluid administration/type of fluid administration and outcomes in children with acute pancreatitis. Overall, 100 patients received normal saline (NS) and 41 received lactated ringers (LR). Liberal fluid management was considered to be >1.5x the maintenance.
Key findings:
Patients who received liberal fluids were less likely to be admitted or transferred to the intensive care unit compared with those receiving conservative management (OR, 0.32)
The liberal NS fluid group with early feeding had the lower rates of moderate/severe manifestations of AP compared with other combinations of diet and fluid orders except the conservative LR group
Moderate/severe AP was highest in the conservative NS group (14/37 [38%]), followed by liberal LR (6/31 [19%]), liberal NS (9/63 [14%]); it was lowest in conservative LR group (0/10 [0%]).
In the discussion, the authors note that adult studies have supported a more moderate approach to IVFs (1.5 mL/kg/hr) given the risks of fluid overload in WATERFALL trial.
My take:
It is surprising that so few patients received LR in this study; there has been some evidence that LR is better than NS for AP since 2014 (see blog posts below)
Especially in those receiving NS, more liberal use of IVFs appears beneficial. Reasonable to start at 1.5 x maintenance (as recommended by Dr. Freeman)
Though children generally tolerate liberal IVFs better than adults due to better cardiovascular function, a prospective randomized study is needed to determine which fluid strategy is optimal.
Early enteral feeding is beneficial in most cases
View from the Rialto Bridge, courtesy of Steven Liu who has some amazing pictures
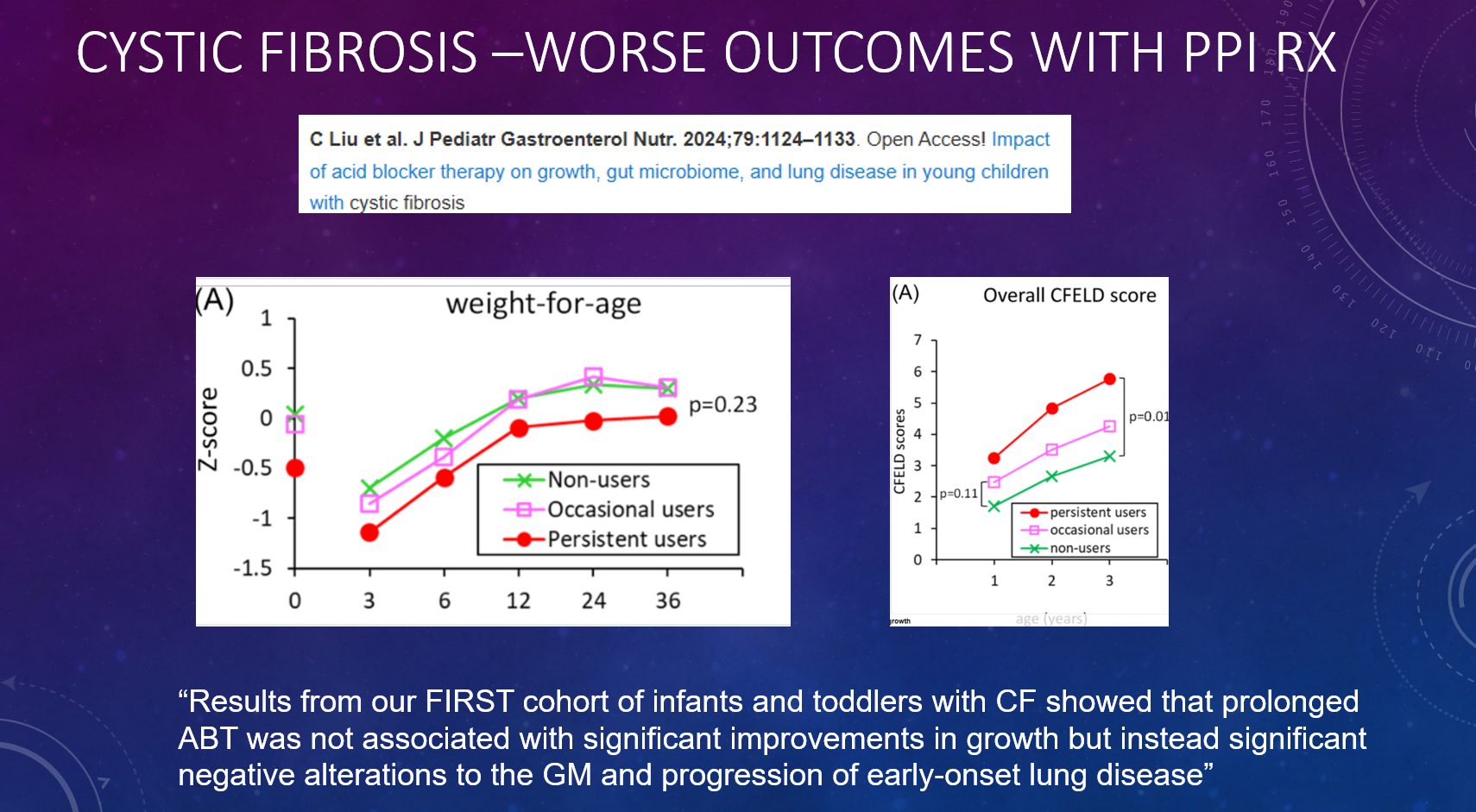
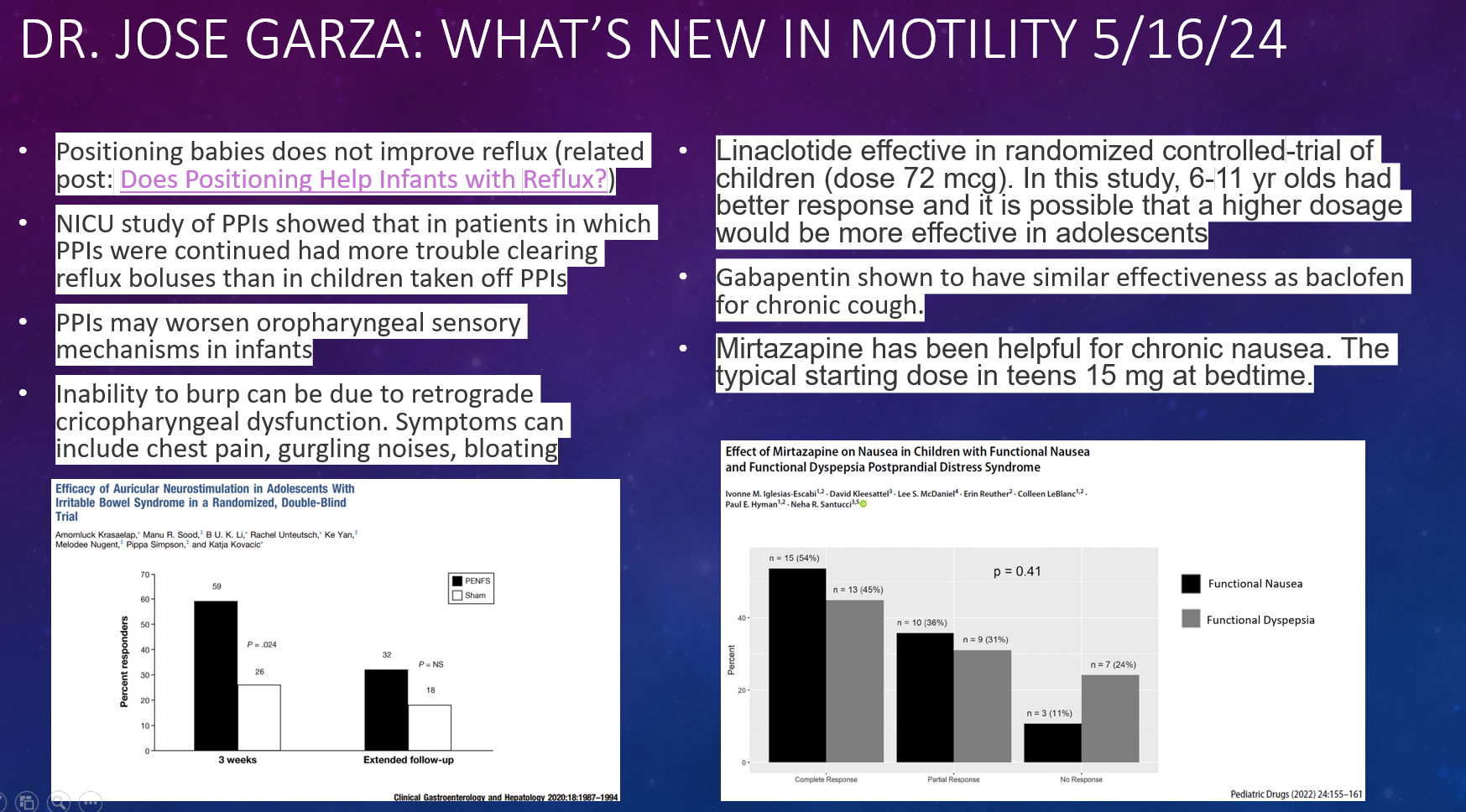
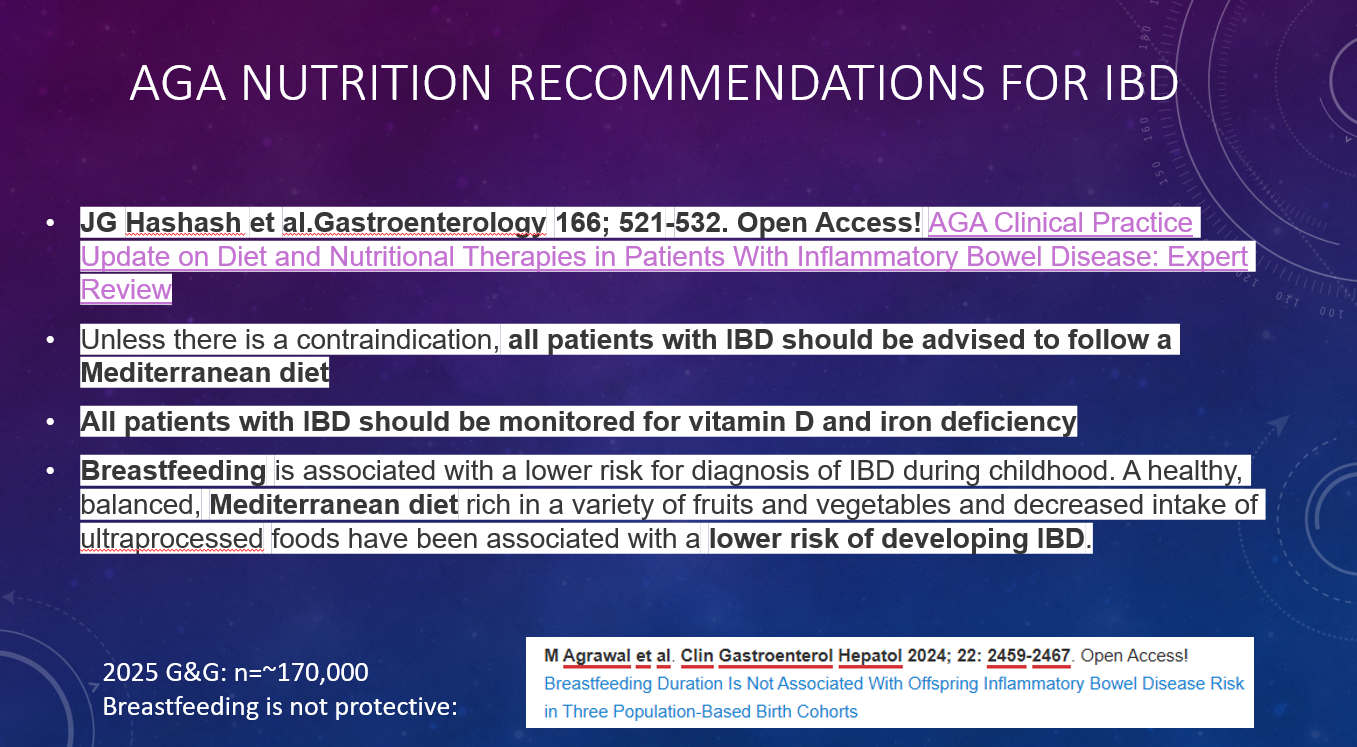
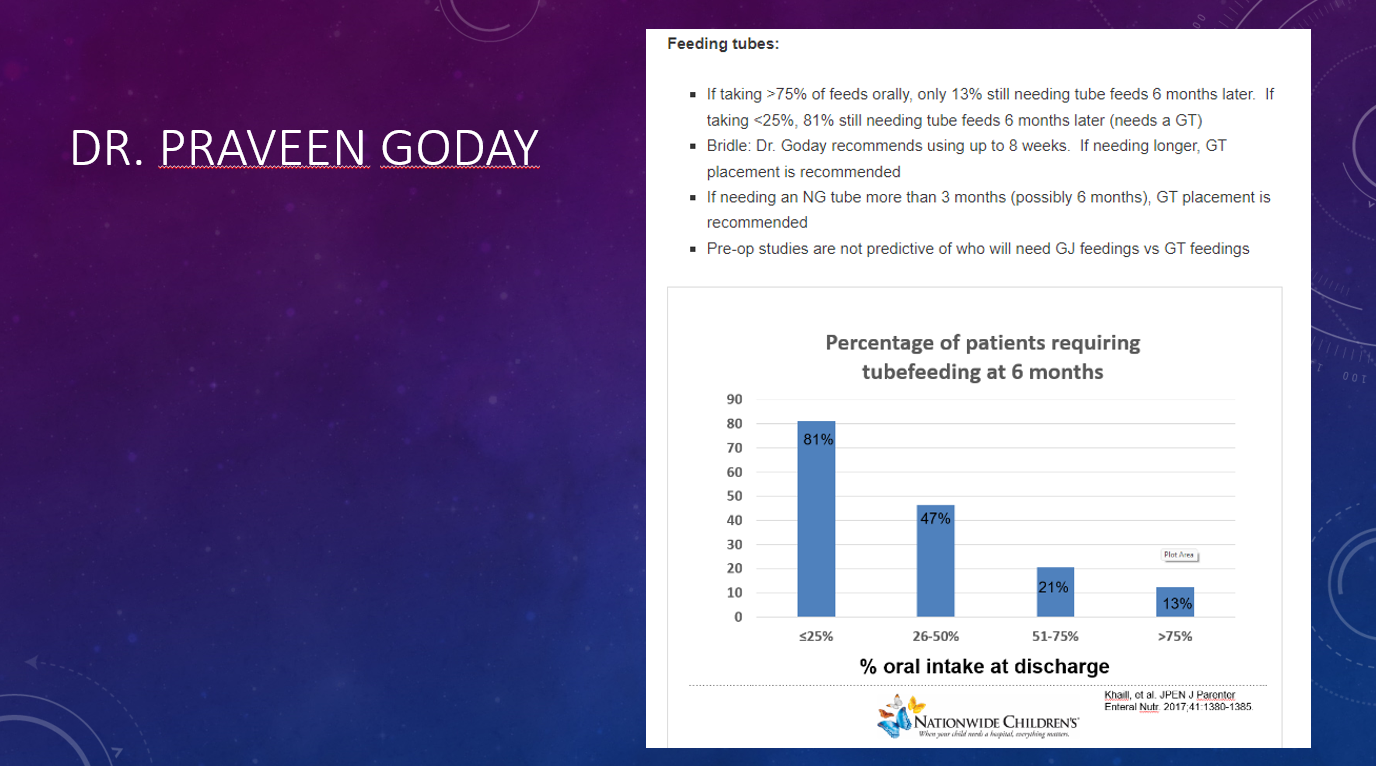
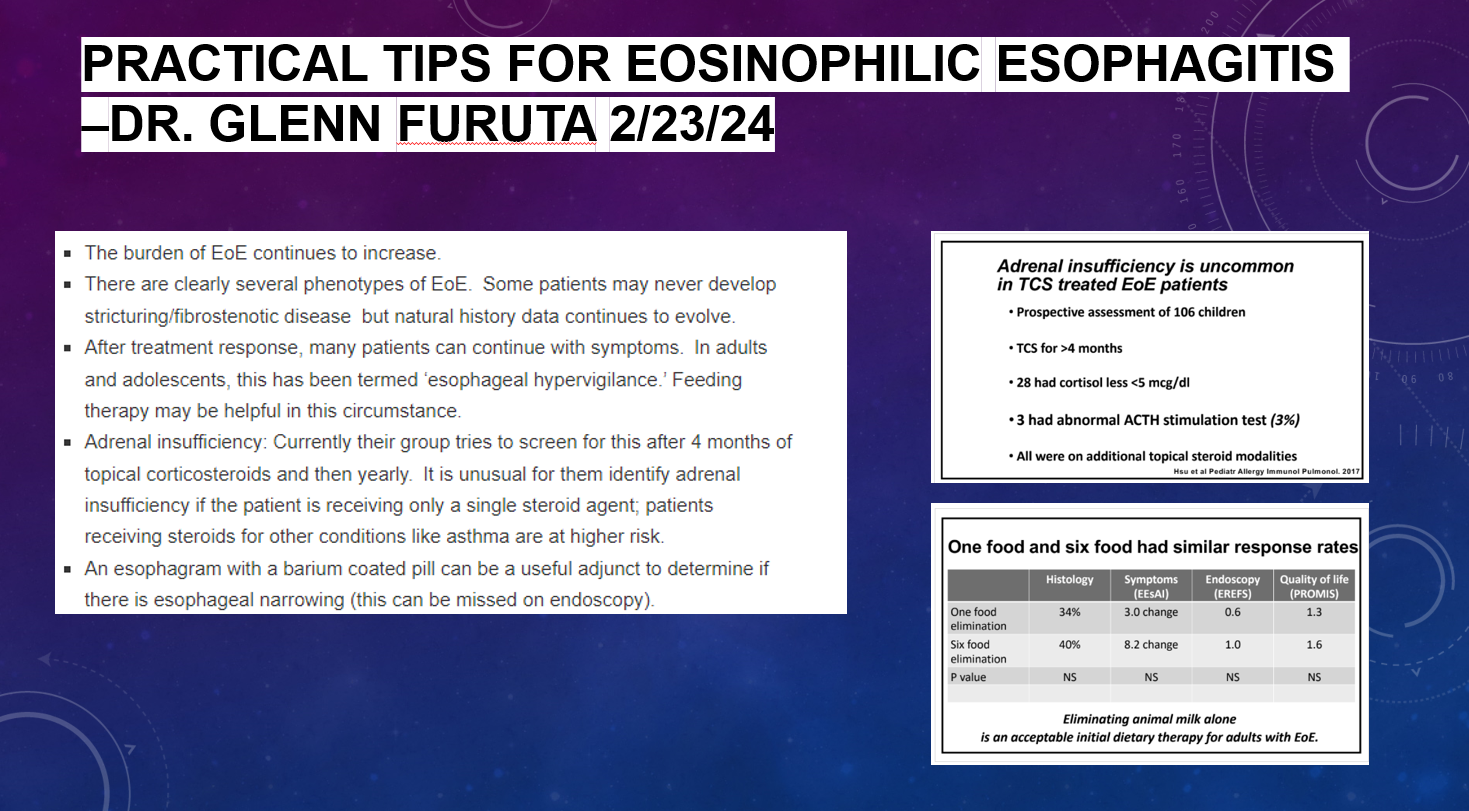
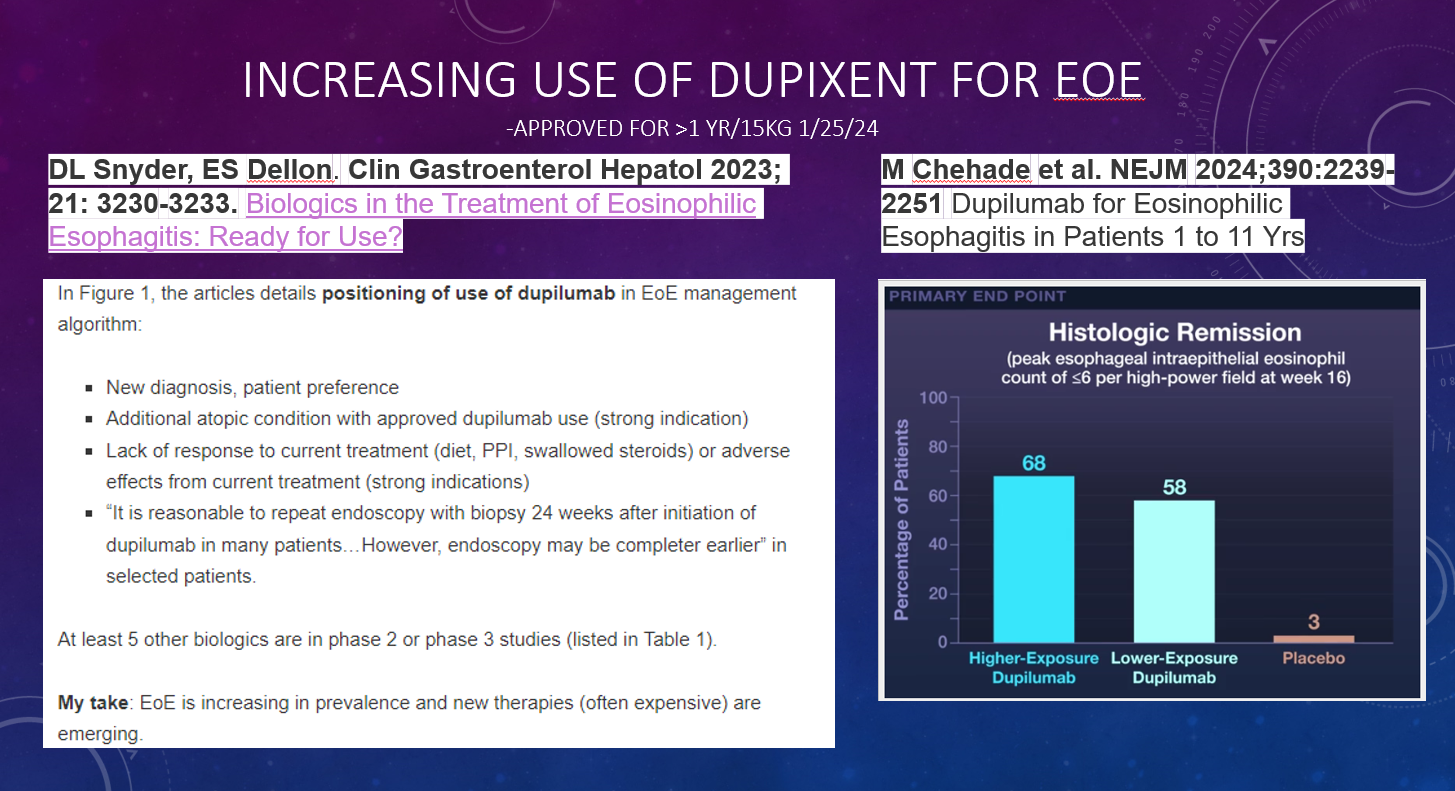
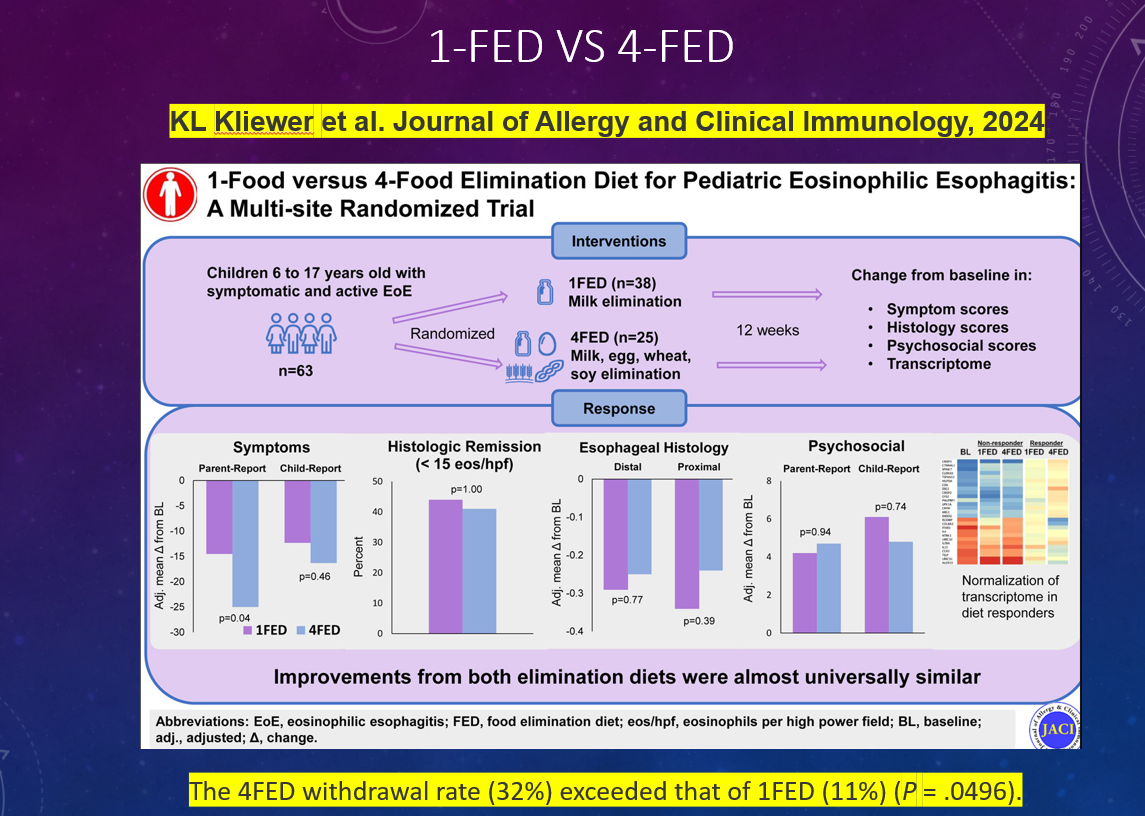
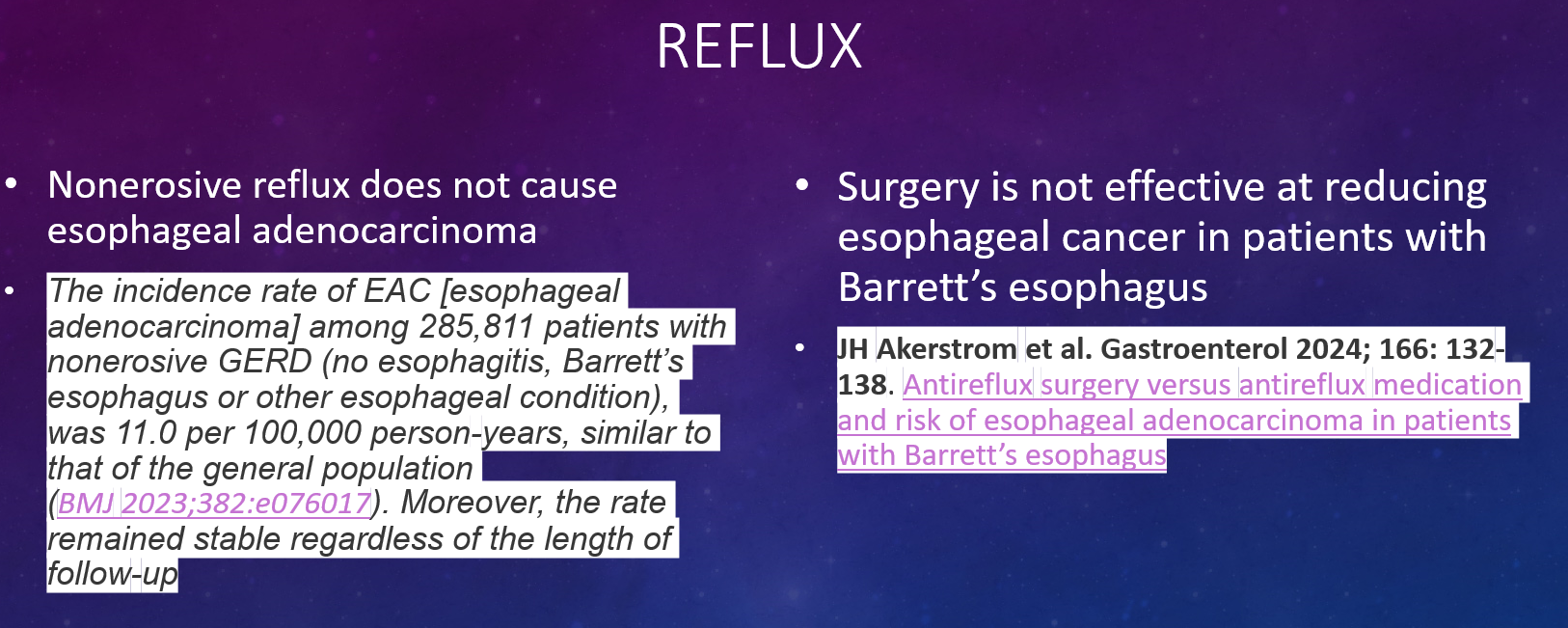
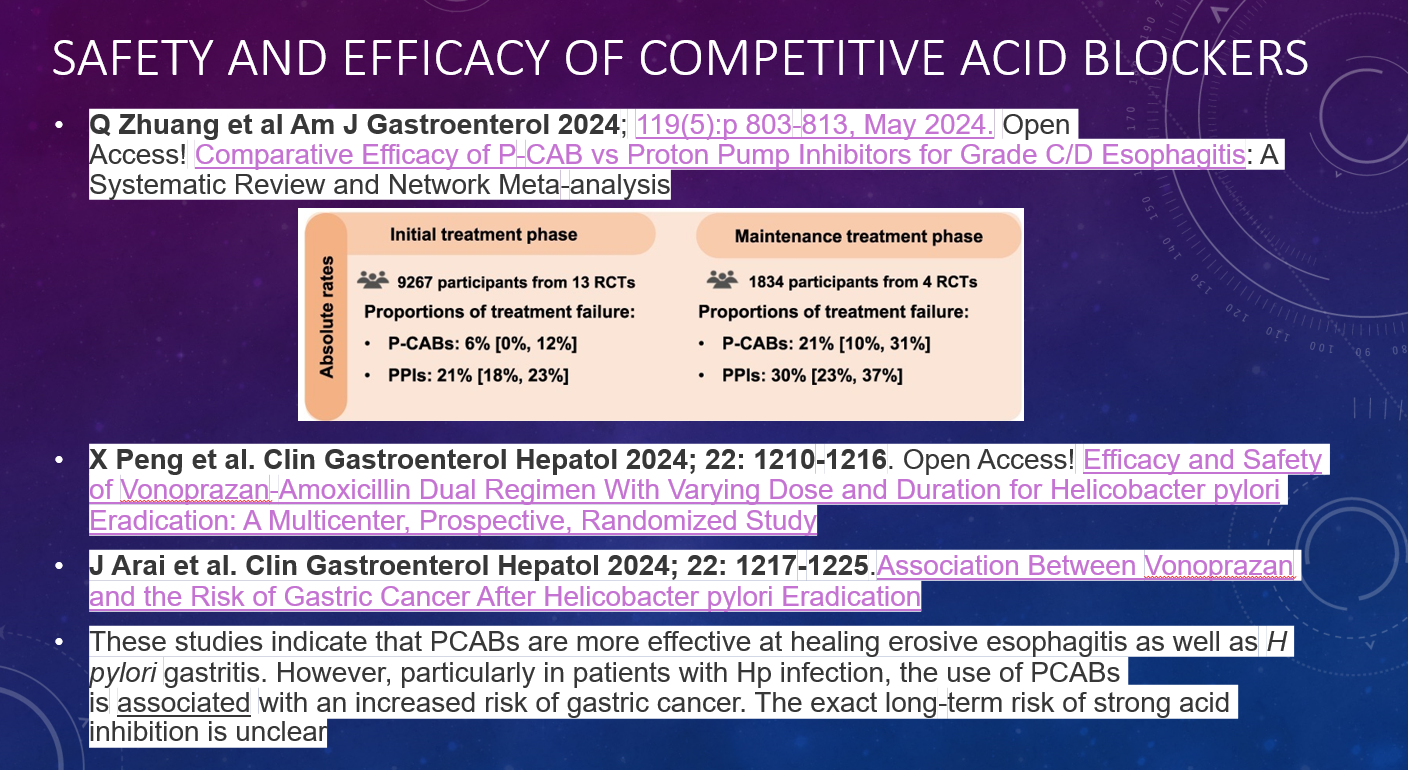
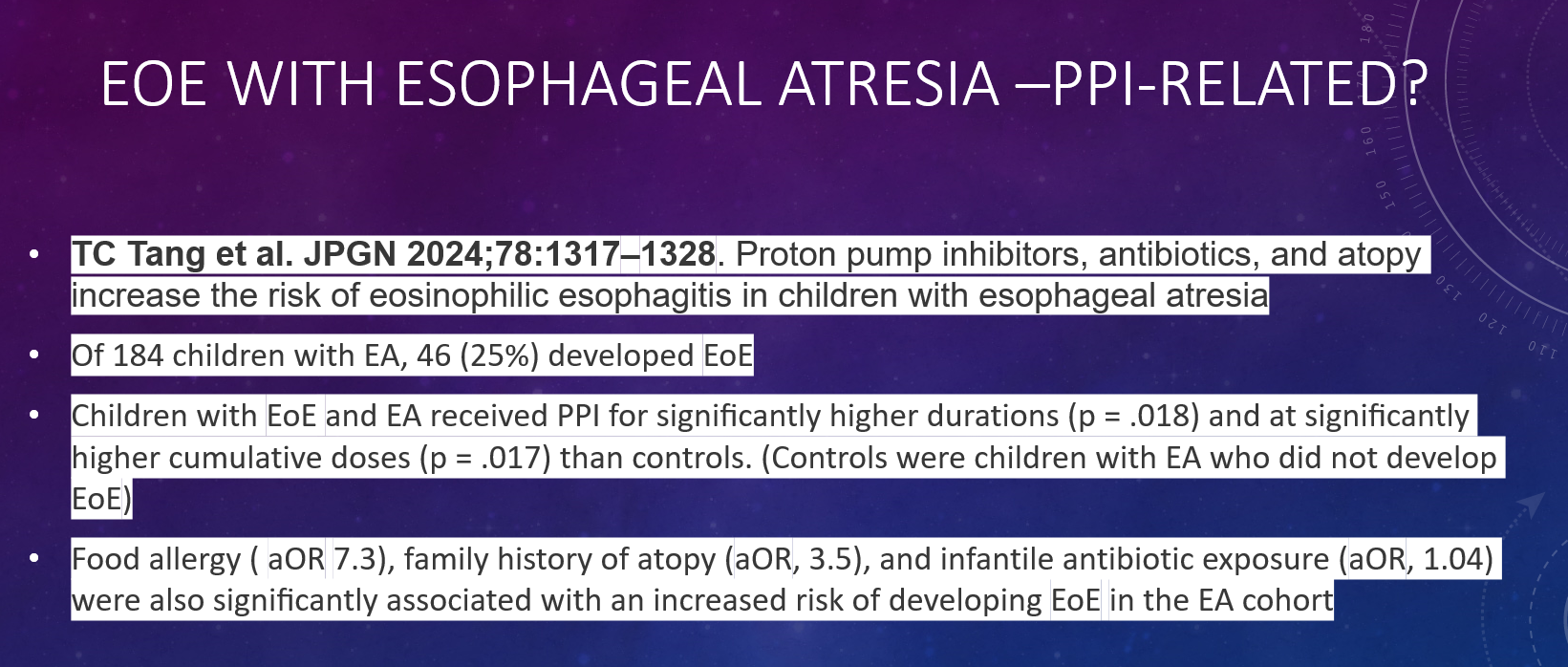
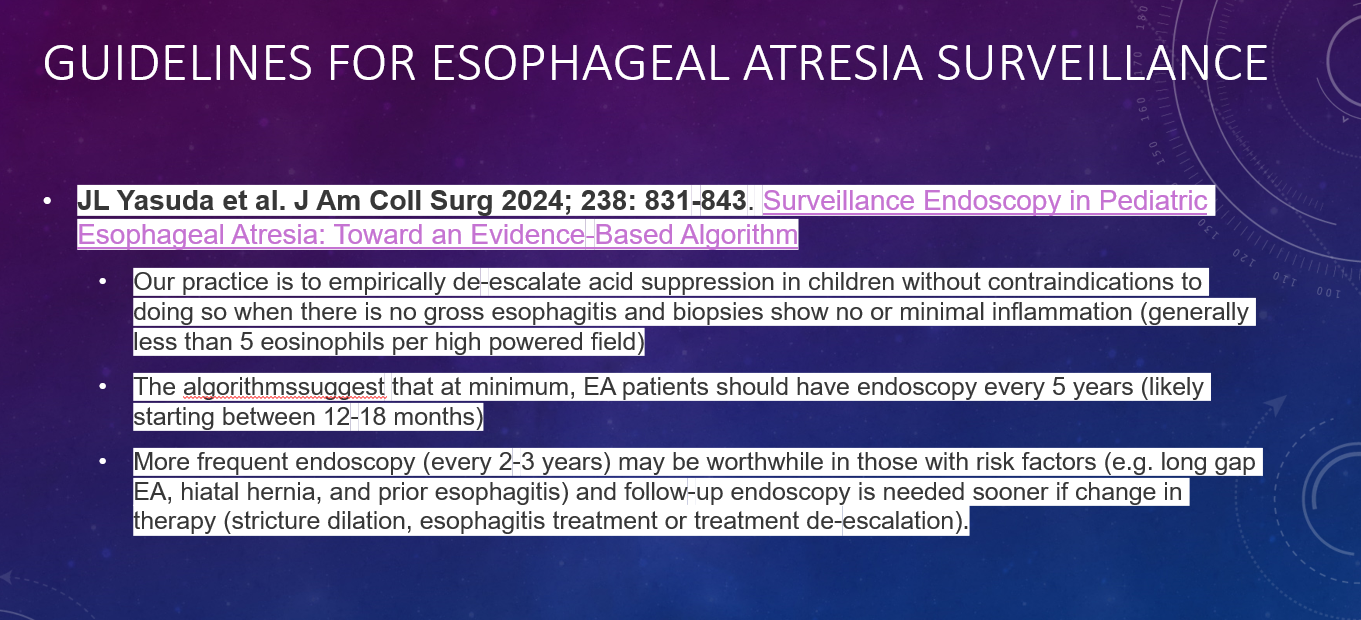
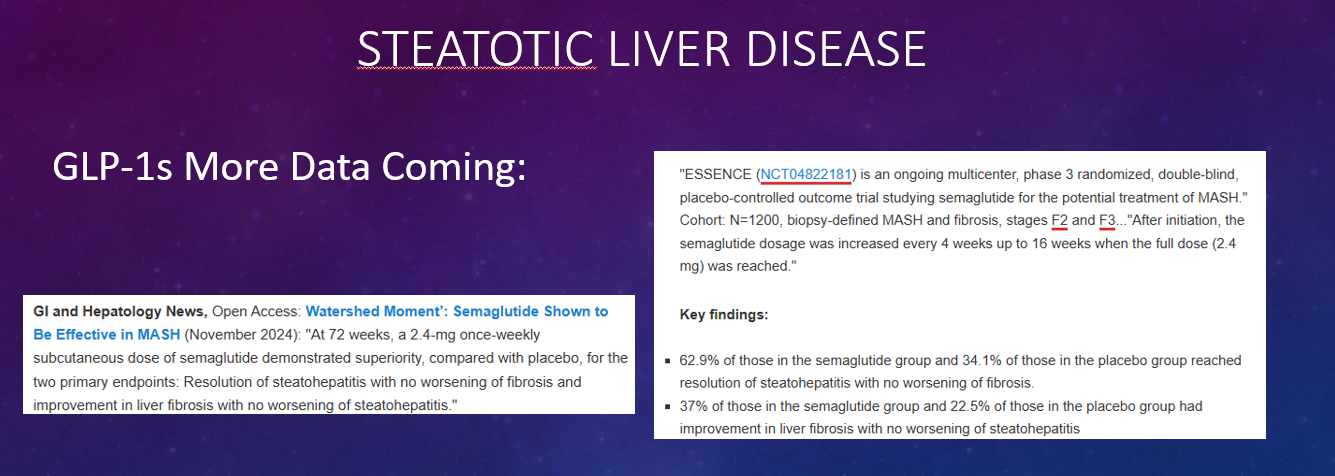
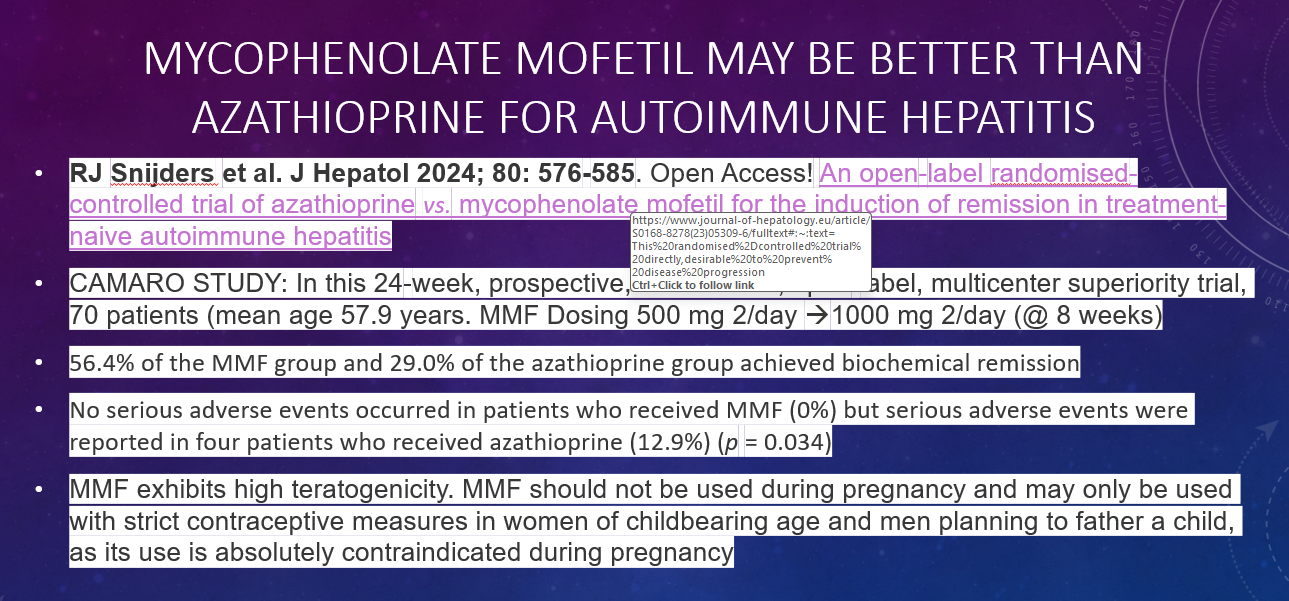
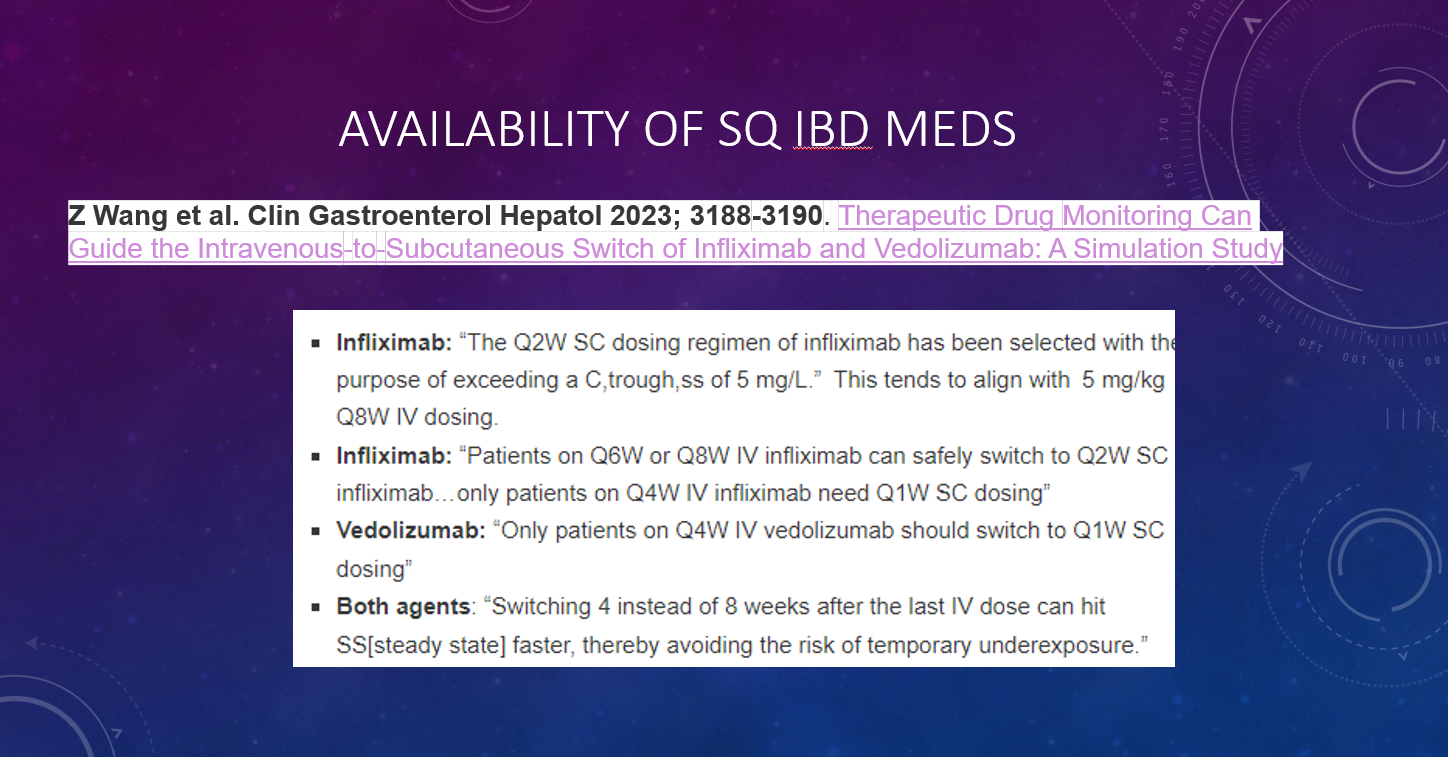
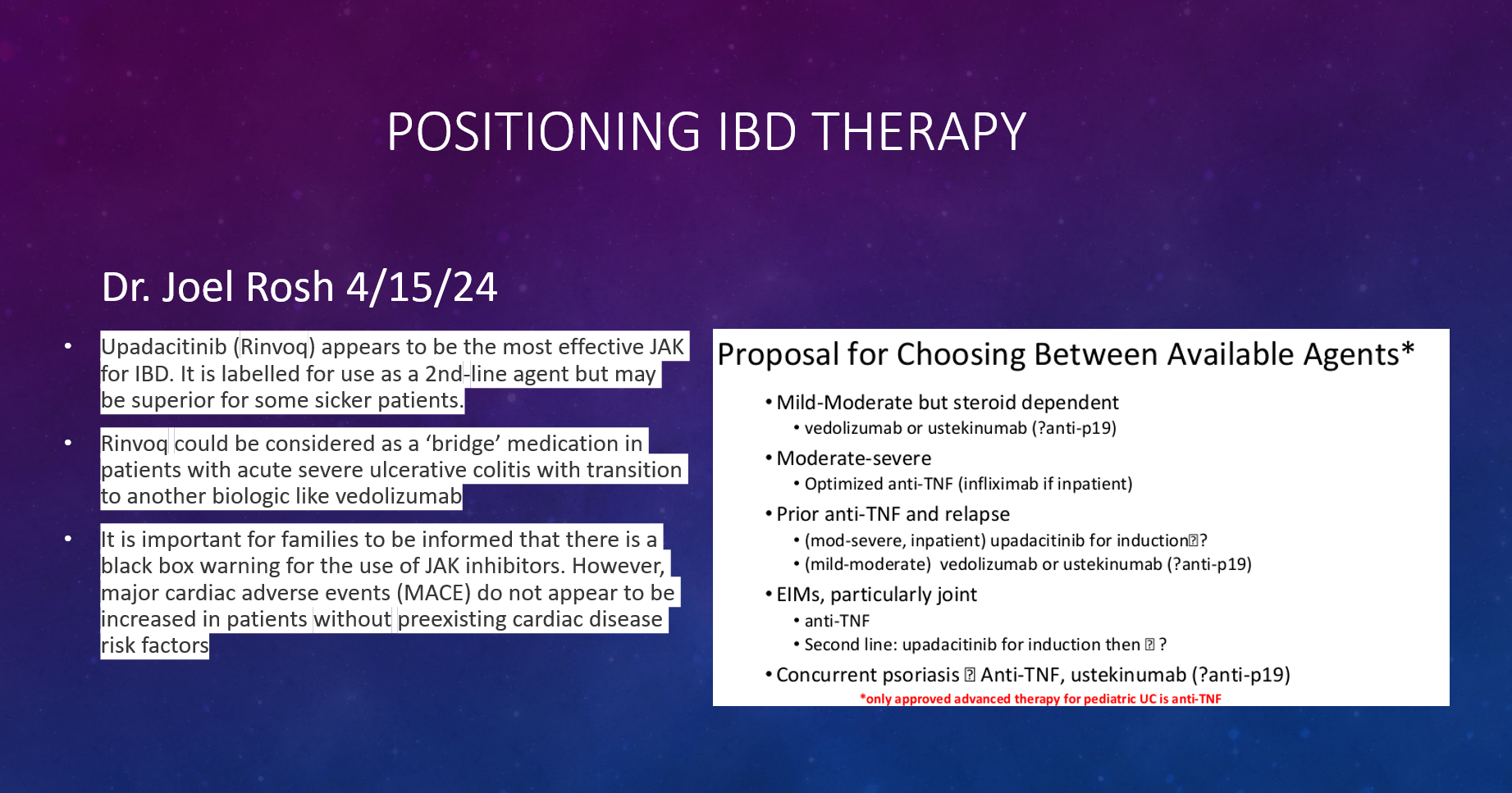
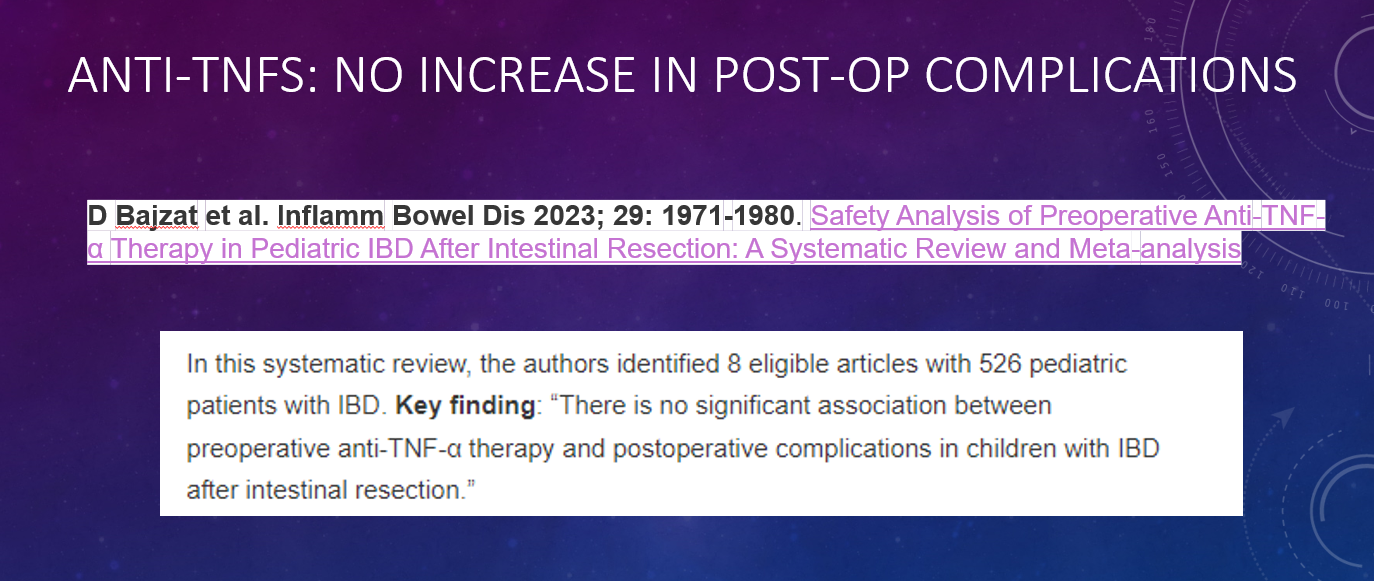
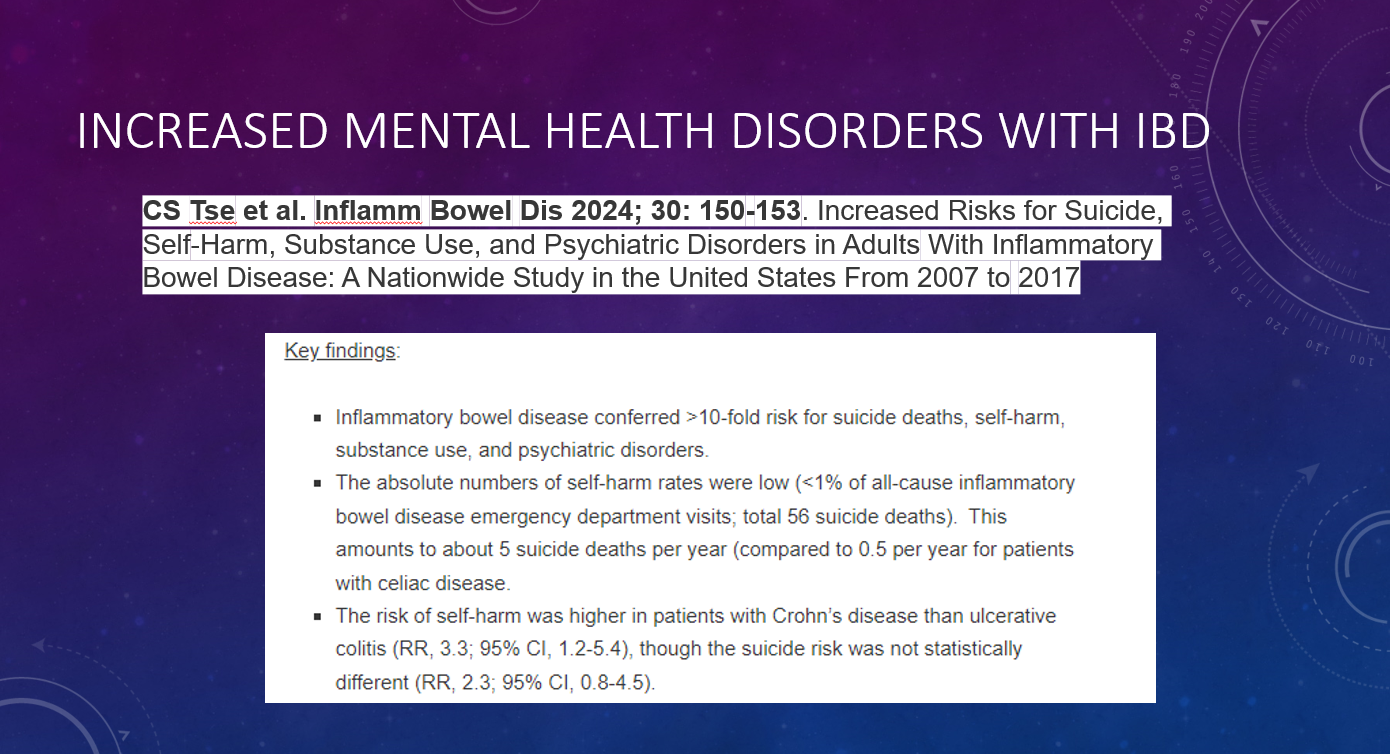
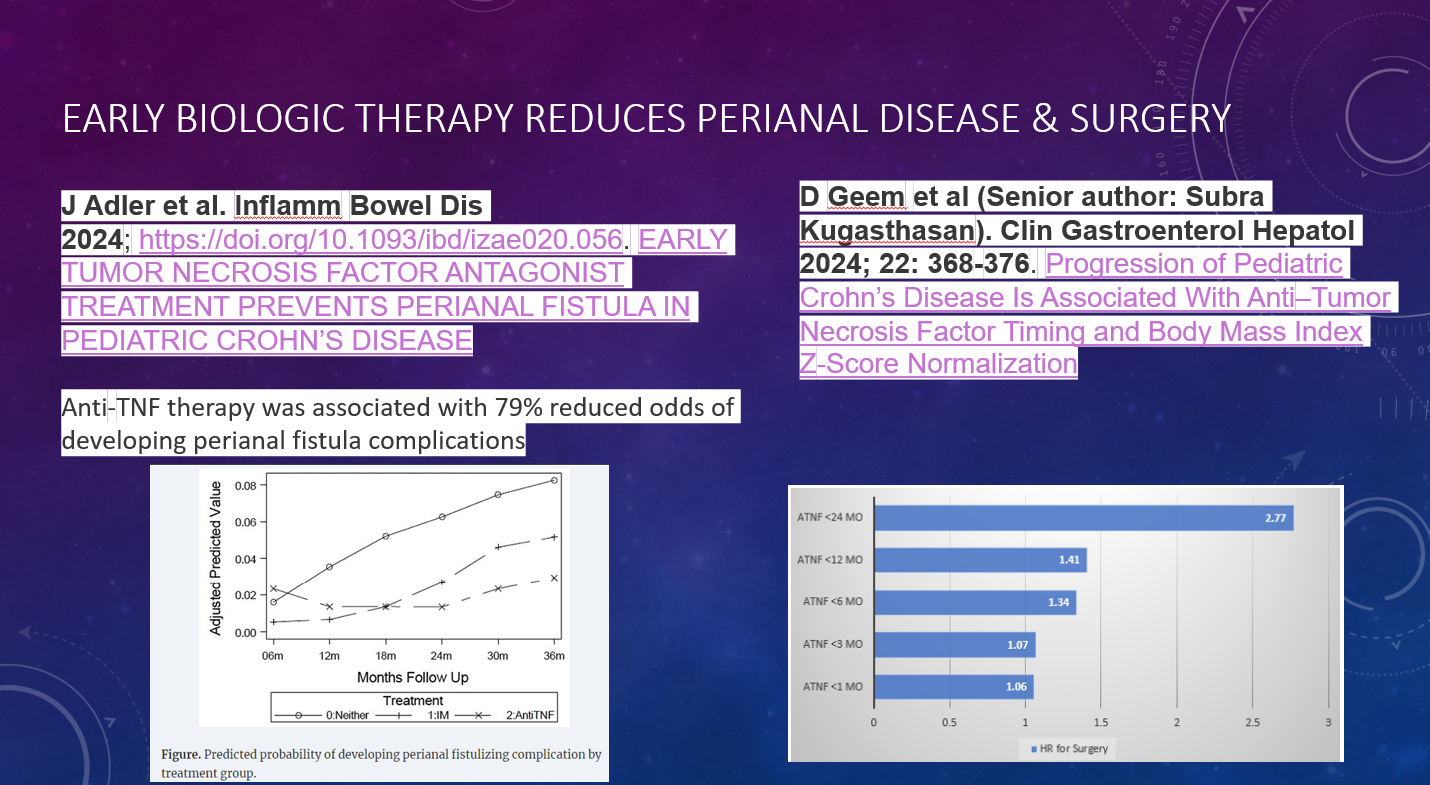
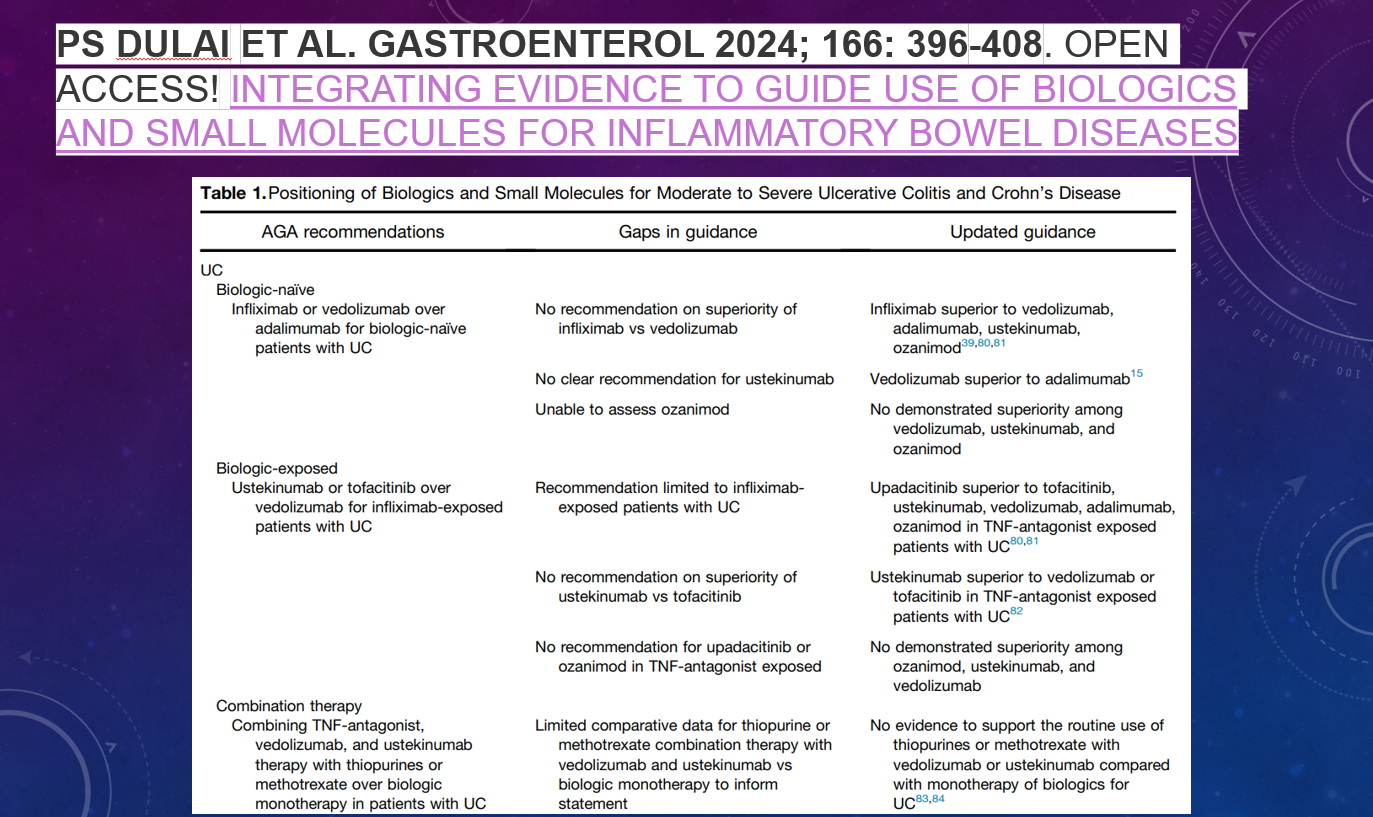
This year I had the opportunity to give a lecture to our group that reviewed much of the important advances that happened in 2024. Here are some of the slides (if you have any trouble reading the slides, you can search for the original blog post using author name).
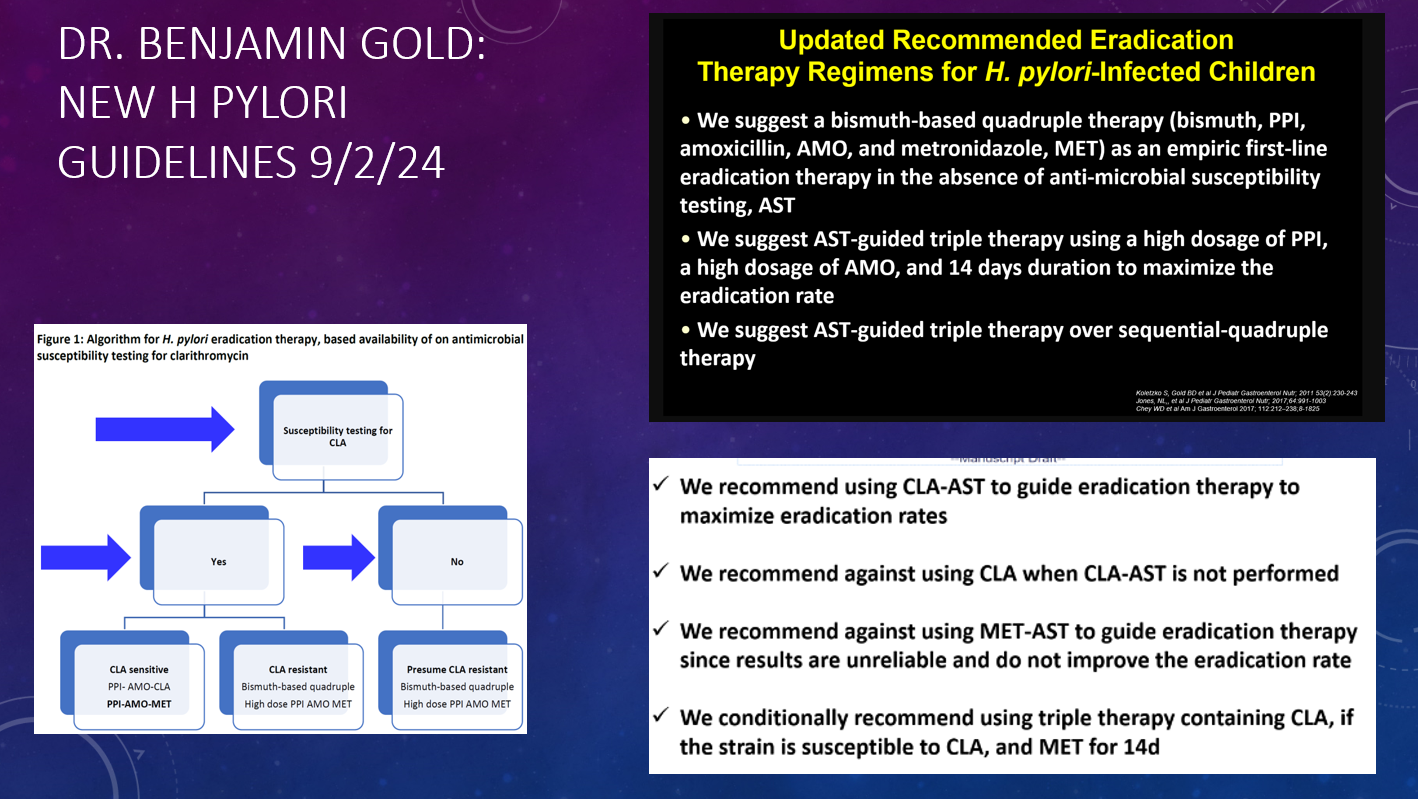
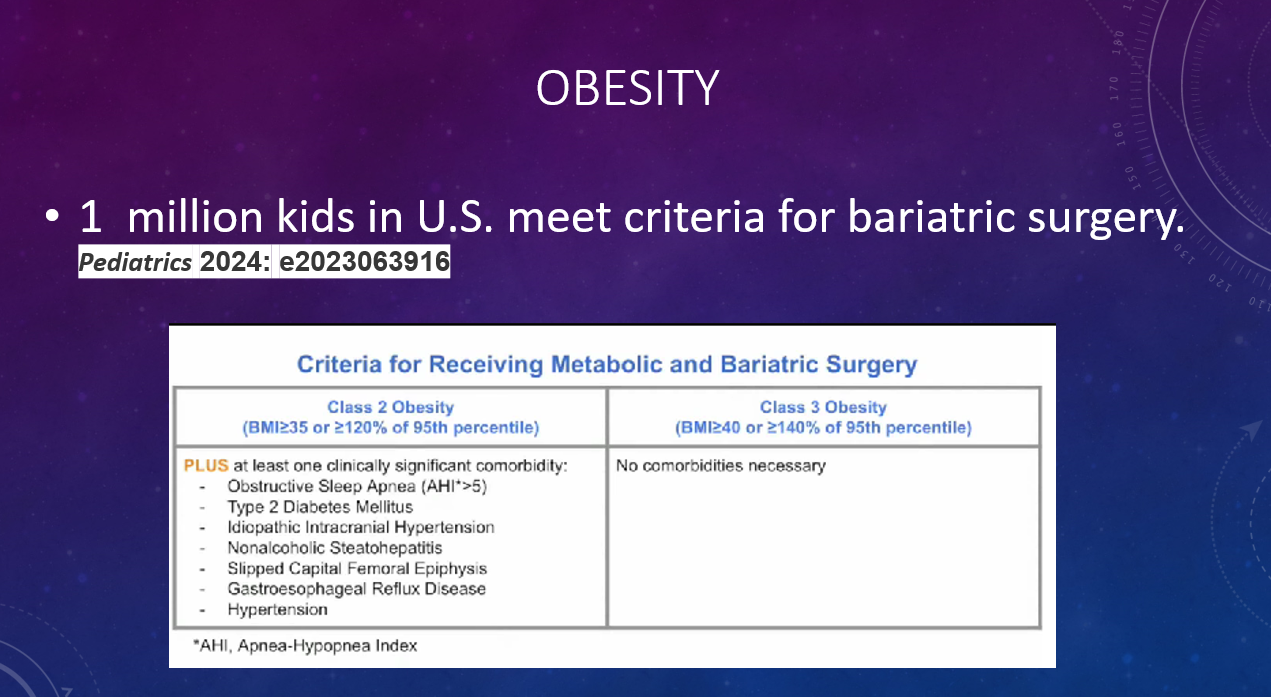
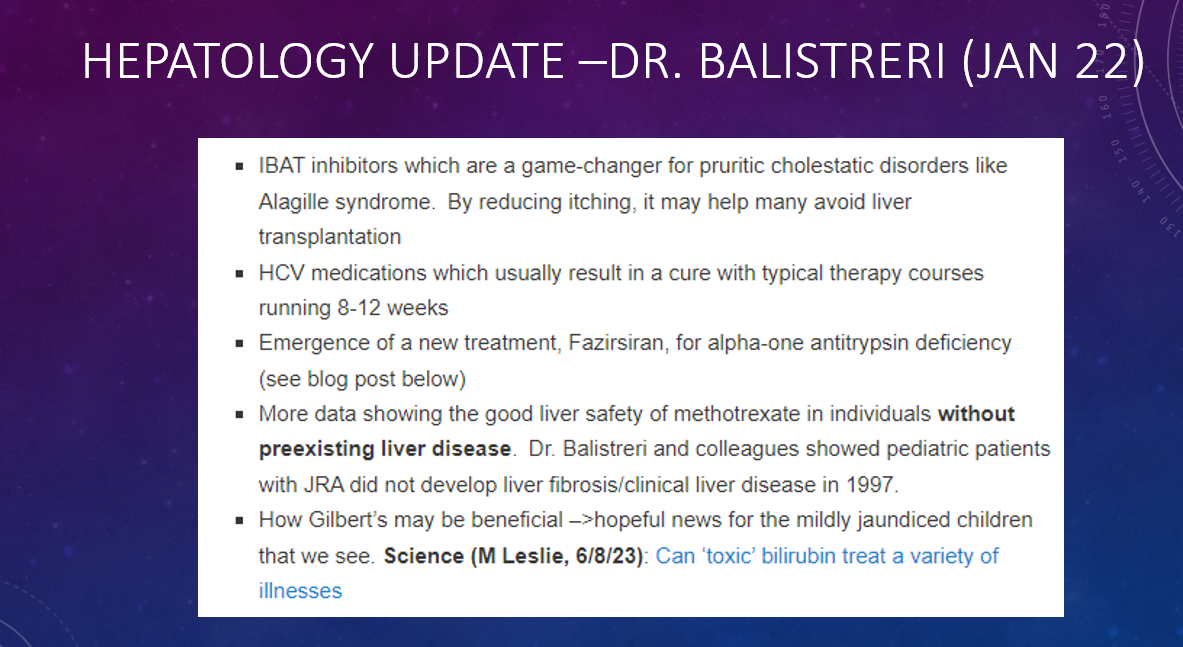
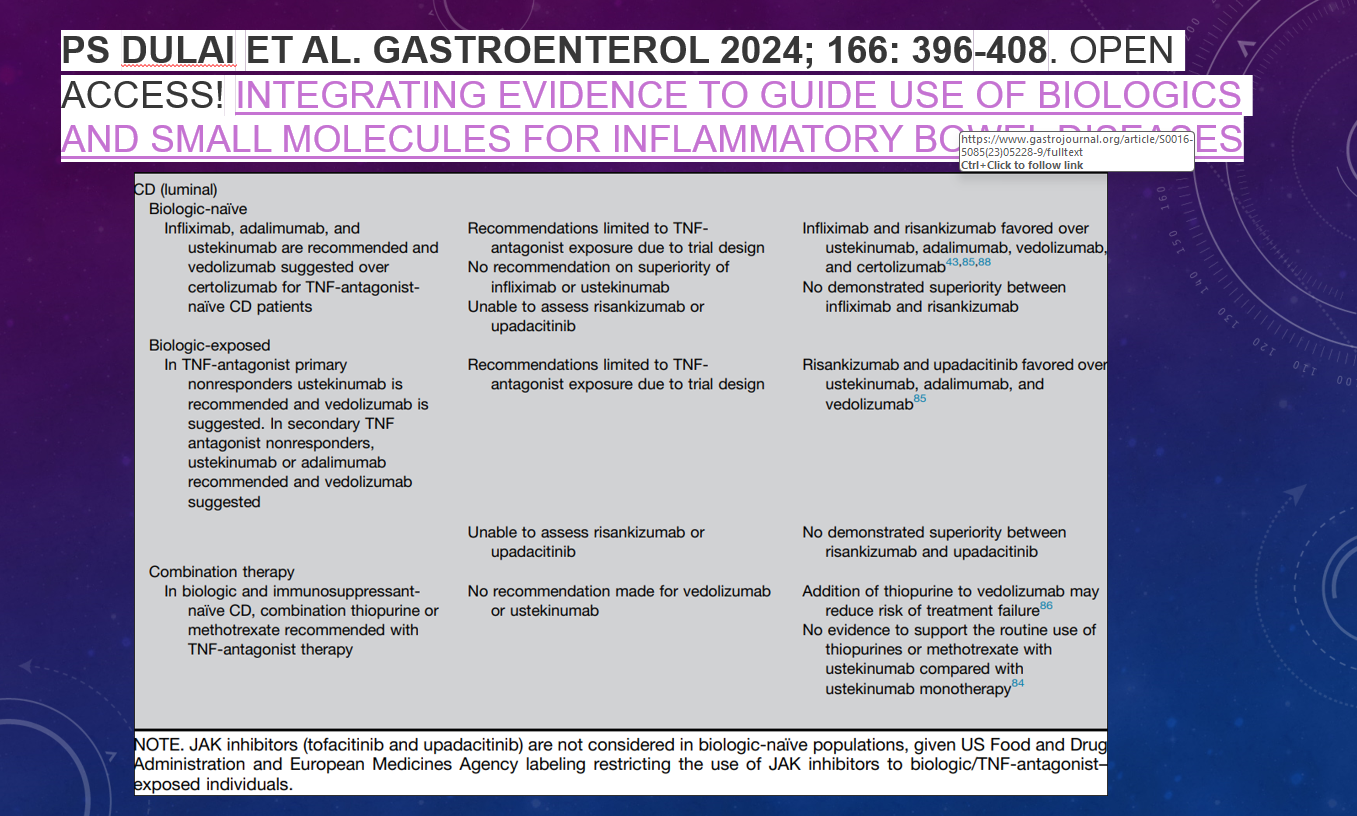
This year I had the opportunity to give a lecture to our group that reviewed much of the important advances that happened in 2024. Here are some of the slides (if you have any trouble reading the slides, you can search for the original blog post using author name).
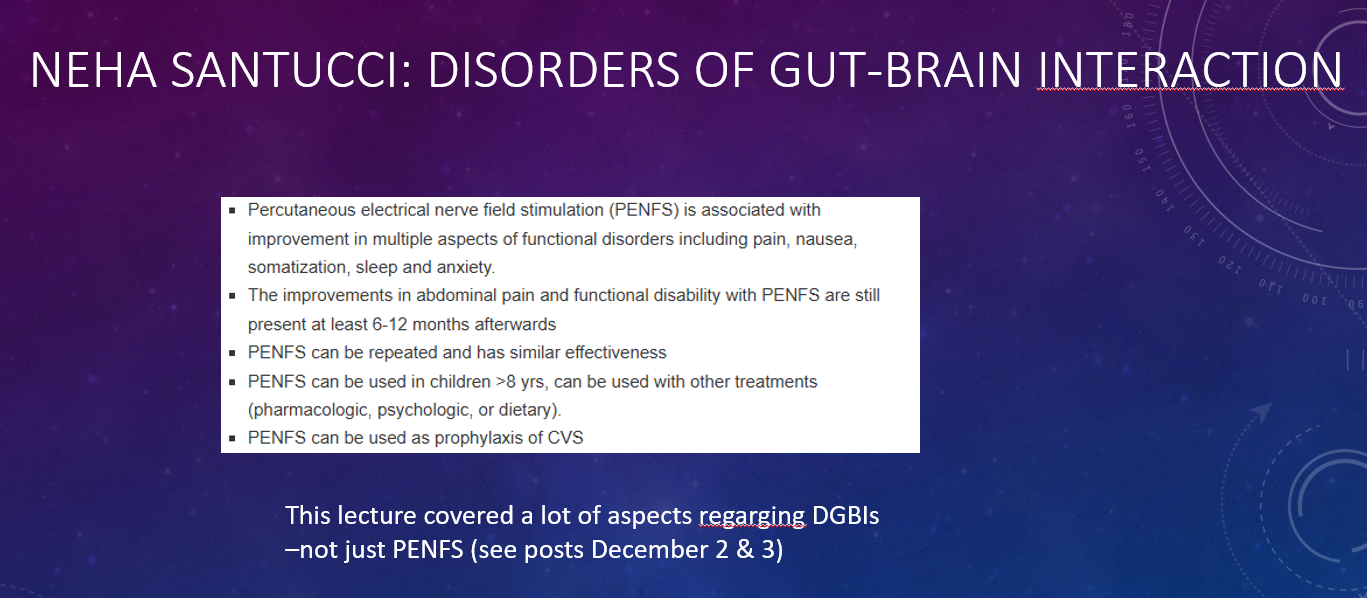
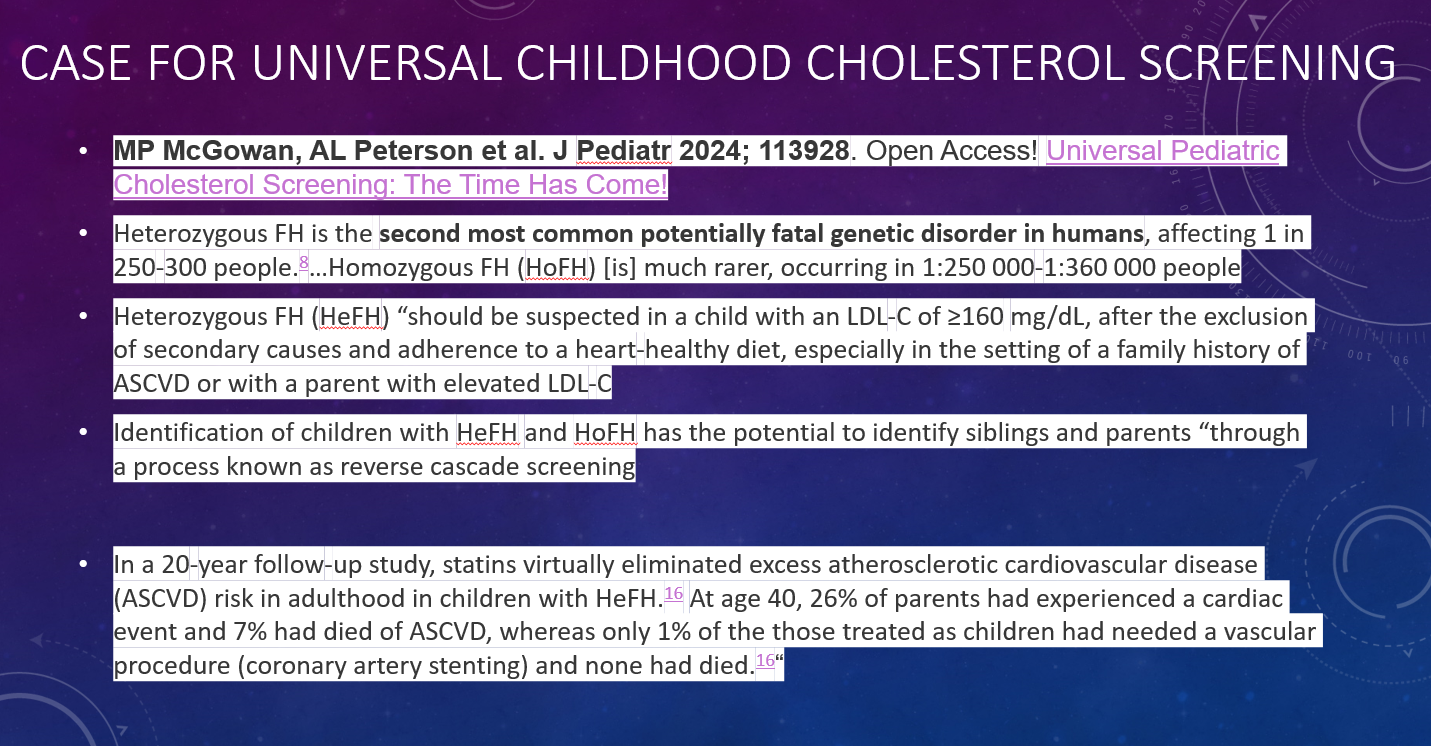
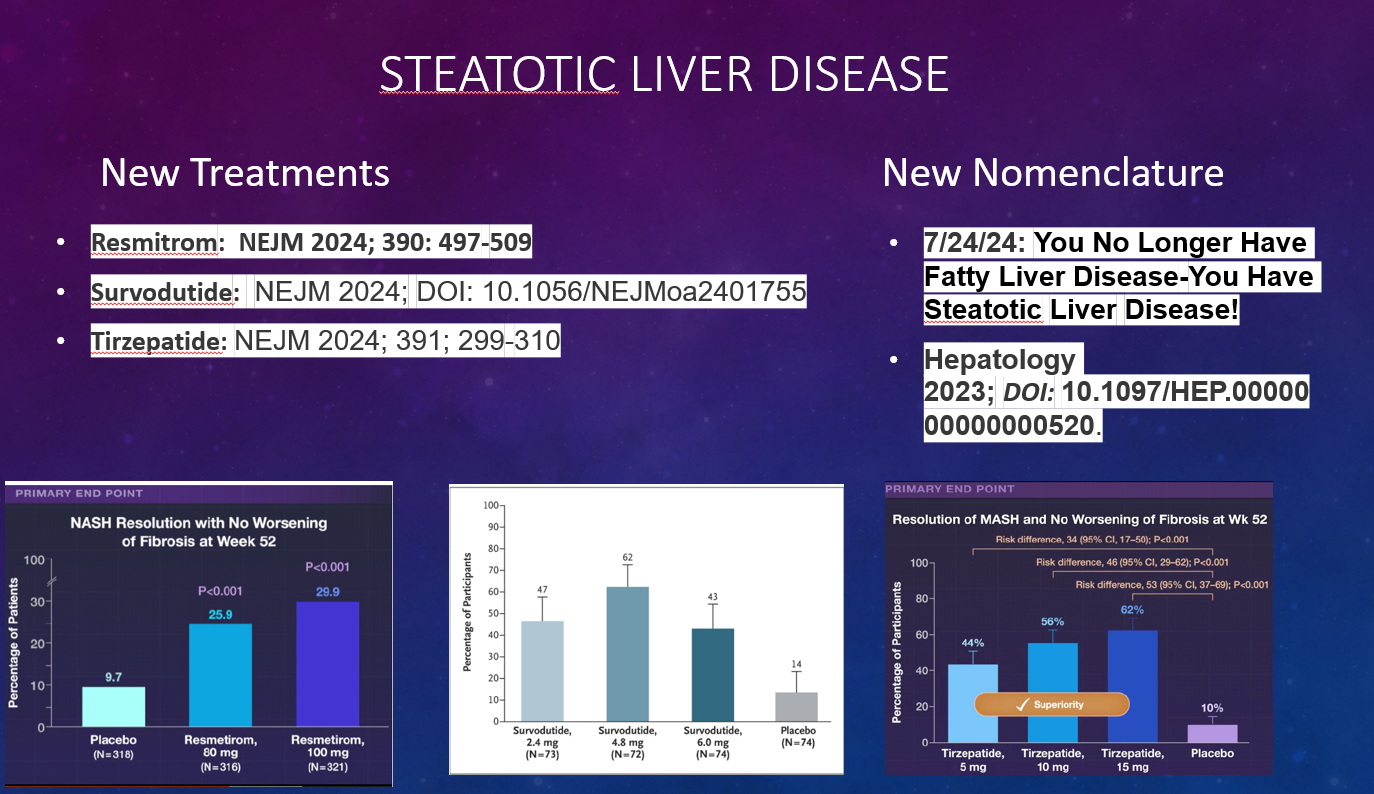
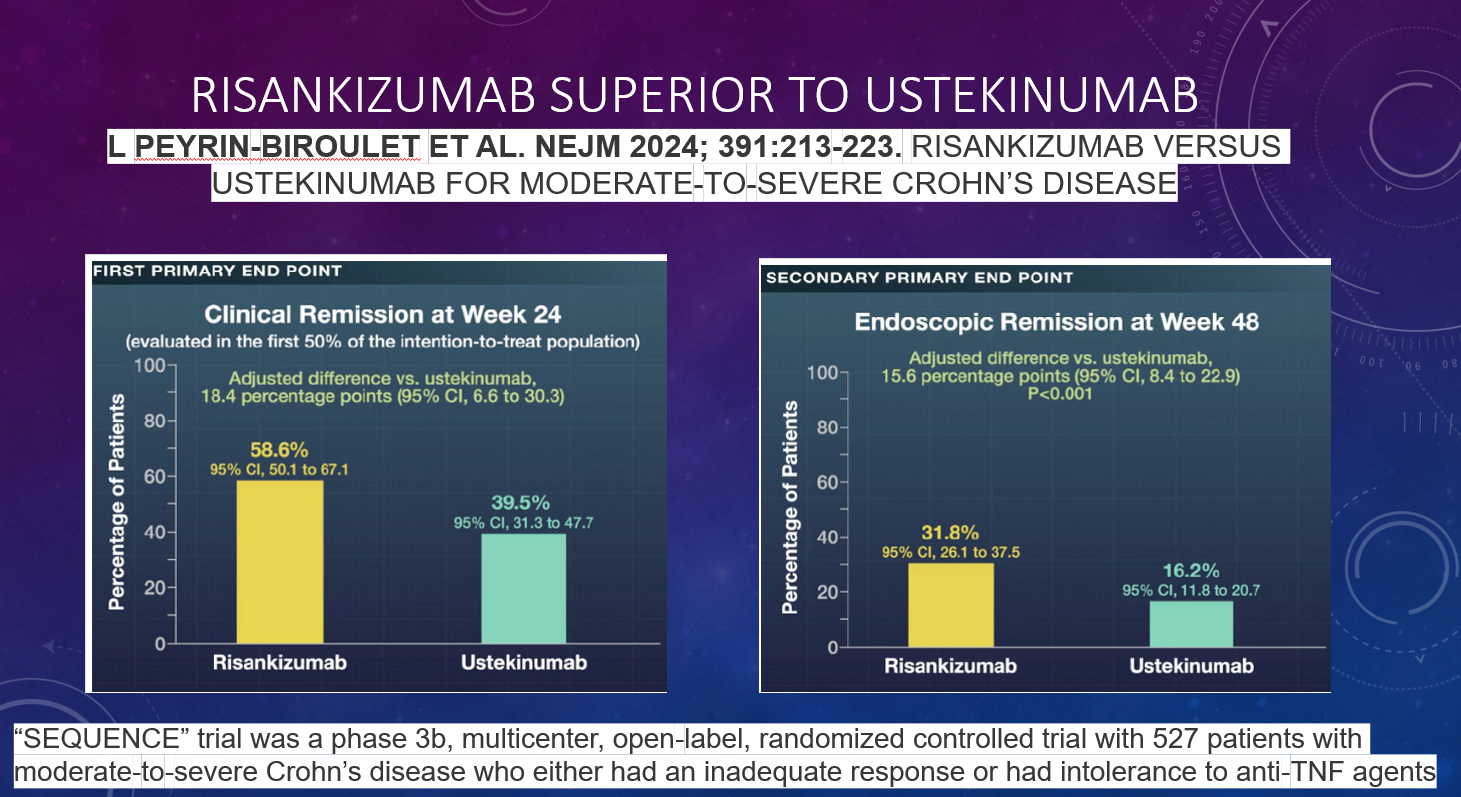
This year I had the opportunity to give a lecture to our group that reviewed much of the important advances that happened in 2024. Here are some of the slides (if you have any trouble reading the slides, you can search for the original blog post using author name).
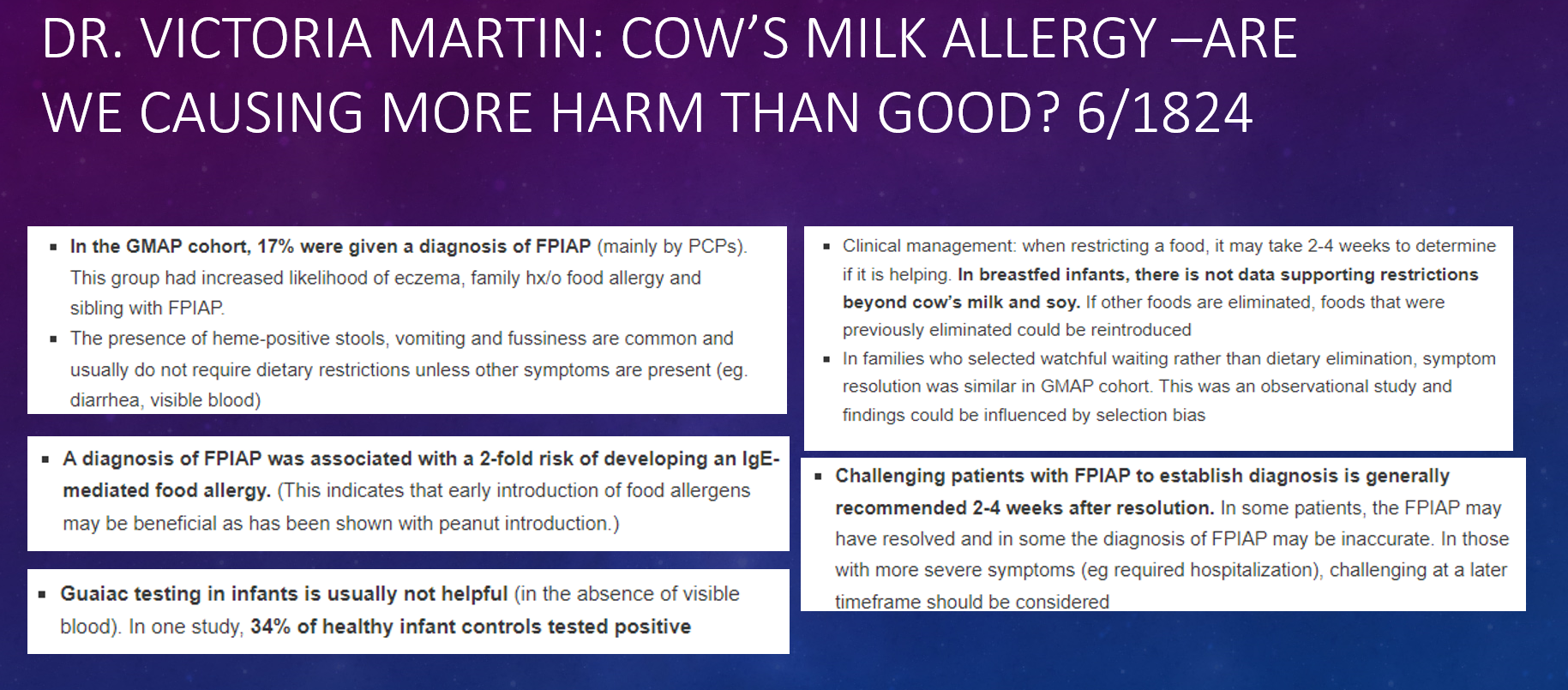
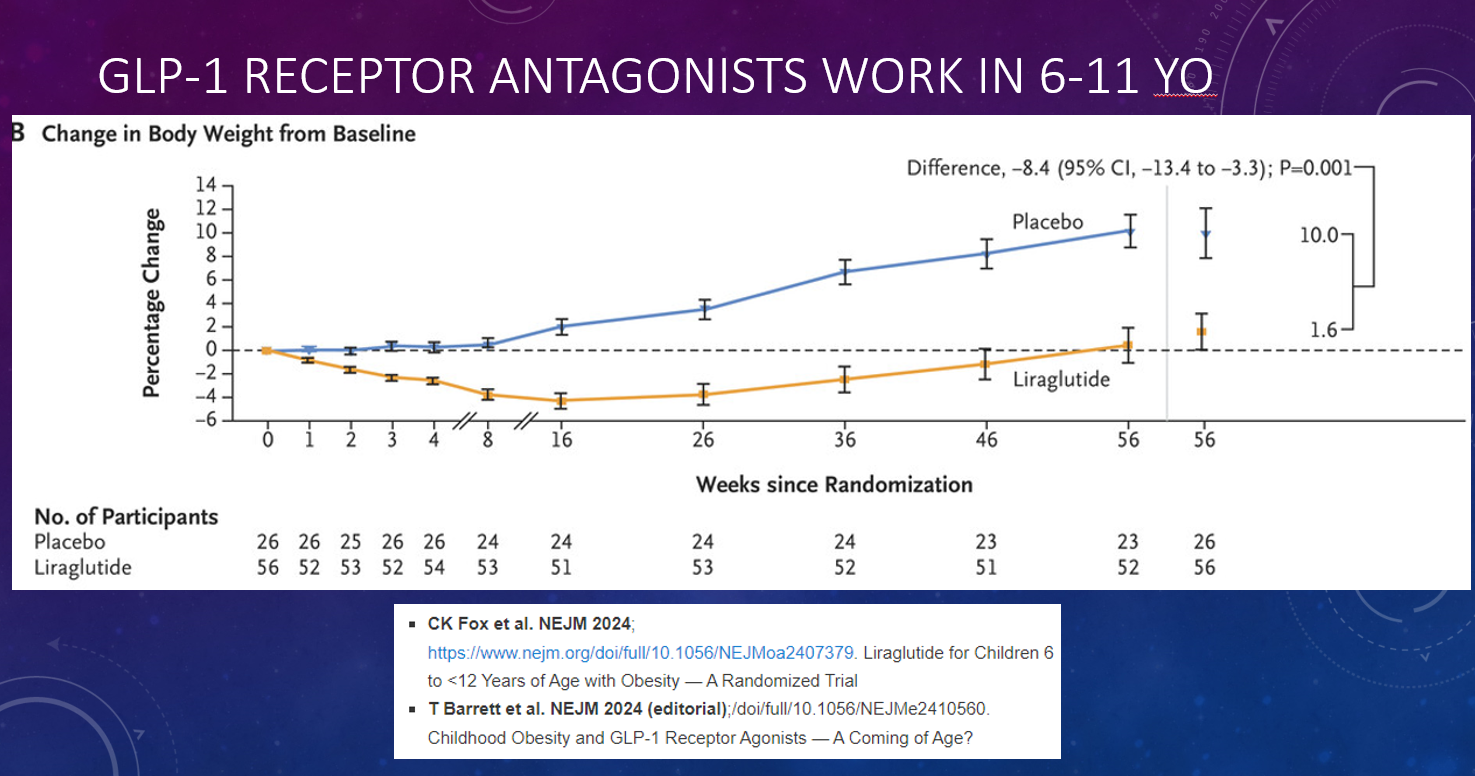
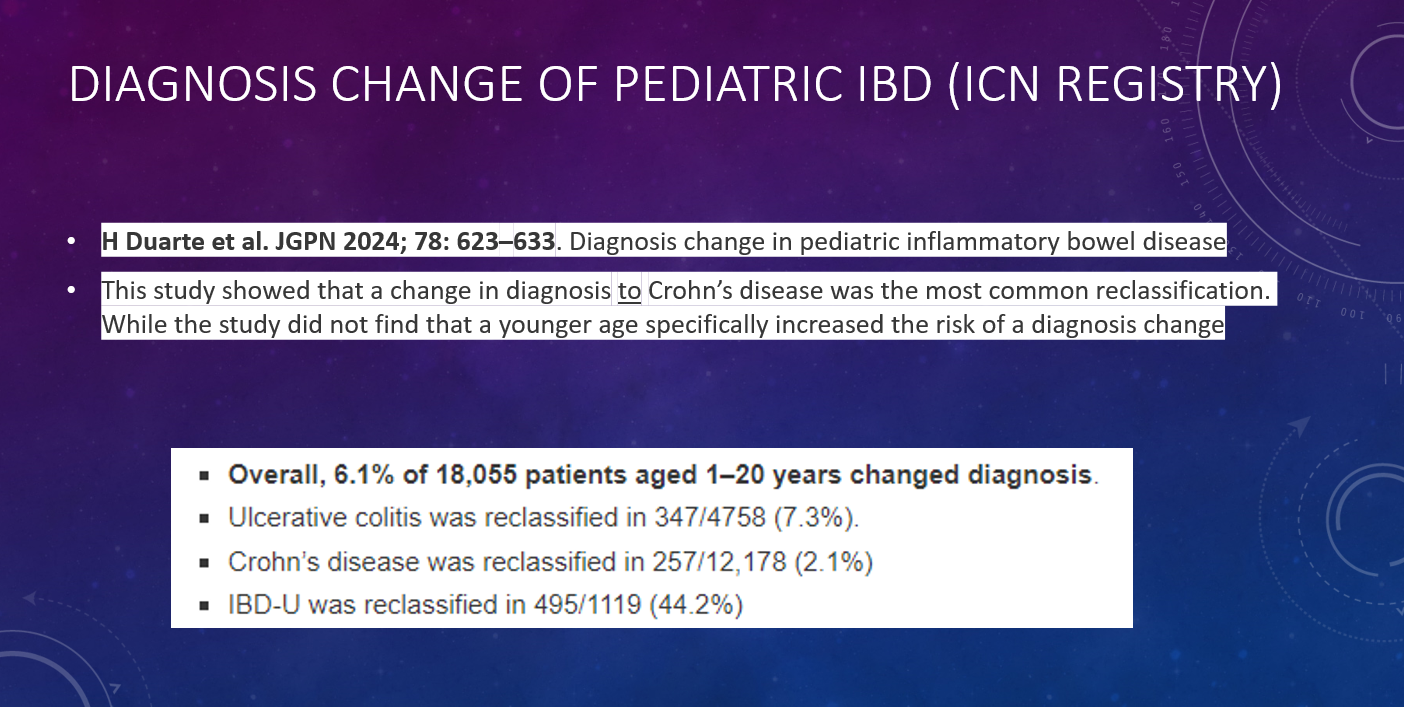
This year I had the opportunity to give a lecture to our group that reviewed much of the important advances that happened in 2024. Here are some of the slides (if you have any trouble reading the slides, you can search for the original blog post using author name).