This retrospective study (n=263) examined the rate of venous thromboembolism (VTE) in pediatric patients who required parenteral nutrition for at least 90 consecutive days.
Key findings:
The cumulative incidence of VTE was 28.1%, with a rate of 0.32 VTEs per 1000 catheter-days
The number of catheters and early gestational age were noted to be independent risk factors for VTE
No patients had progression of thrombus while receiving therapeutic anticoagulation
Of those with acute DVTs (n=47), 24 (51%)resolved on repeat imaging, 14 (30%)were stable, and and 9 (19%) had decreased
4.4% (2 of 45) had a major bleed while on anticoagulation
The authors note that the true rate of VTE is likely even higher because only 42% categorized as not having a VTE had undergone dedicated venous imaging.
My take: A lot of patients with intestinal failure develop VTE. Given the risks of treatment, the role of prophylactic anticoagulation remains unclear. This is where a prospective study would be helpful.
Background: “Chronic inflammation can lead to tissue remodeling in the esophagus with fibrosis in the lamina propria that is partially responsible for symptoms and complications of EoE.3,4 At times, a firmness to the esophagus can be appreciated with a noticeable force required to obtain biopsies from EoE. This sensation has been described as the “tug” or “pull” sign.5,6“
Methods: in this prospective study with 159 patients (128 pediatric, 31 adult), the authors devised a digital force gauge to measure the force required to take biopsy specimens. The study included 88 patients with EoE and 71 controls.
Key finding:
EoE patients showed an increase in the mean force required to obtain biopsies: 14.9 Newton (N) compared to 11.6 in control group
Peak force was greater in EoE patients: 20.4 N compared to 15 N in control group.
The pediatric subgroup had higher peak force in EoE patients: 22.4 N compered to 16.1 N for control group
My take: I had not heard of the term “Tug” sign for EoE, though it is something that is intuitive for GI providers who care for these patients. This study quantifies this problem.
“When you can measure what you are speaking about and express it in numbers, you know something about it; but when you cannot express it in numbers, your knowledge is of a meagre and unsatisfactory kind” –Lord Kelvin 1883
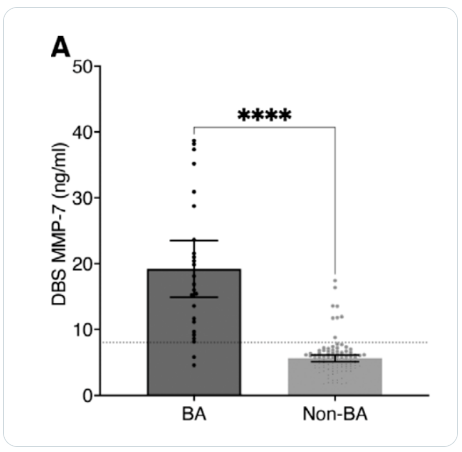
Methods: The study used stored DBS samples collected from 48 to 72 hours of life were retrieved from newborn screening centers in Taiwan (n=25 biliary atresia (BA), 107 non-BA)
Key findings:
MMP-7 levels of BA patients on the DBS were significantly higher than those of non-BA patients (19.2 ± 10.4 vs 5.6 ± 2.7 ng/mL, P value < 0.0001).
BA patients in this cohort underwent Kasai operation at a mean of 43 days. 32% (n=8) had surgery before 30 days of life, and 24% (n=6) had surgery after 60 days.
In this cohort, at time of publication, 9 (36%) of BA patients had received a liver transplantation at a mean of 2.4 years. Patients with their native liver tended to have had an earlier Kasai (38 days vs 54 days, P=0.057).
In their discussion, the authors note that BA starts very early in life. Increase in MMP-7 within 3 days of birth, supports “speculation that most BA ” may start before birth (JPGN 2019; 69: 396-403, What Is The Evidence That Biliary Atresia Starts in Utero?).
My take: Incorporating MMP-7 testing with newborn screening needs to be looked at in a bigger study. Efforts to identify BA cases earlier have largely been unsuccessful over the past several decades despite the knowledge that delayed diagnosis leads to worse outcomes.
Methods: This study analyzed postresection pediatric (≤18 years) CD patients (n=434) identified in the 2007–2018 IQVIA Legacy PharMetrics administrative claims database
Key findings:
Risk of surgical recurrence was 3.5%, 4.6%, and 5.3% at 1, 3, and 5 years, respectively
Postoperatively, patients were most commonly prescribed an immune modulator (33%), anti-tumor necrosis factor agent (32%), or antibiotic (27%)
My take: Current recommendations include postoperative endoscopic surveillance 6-12 months after surgery. Would the surgical recurrence rate have been lower if there had been higher postoperatively endoscopic evaluation?
This single center retrospective study reviewed 640 colonoscopies in symptomatic children.
Key findings:
Thirty-three children had isolated histologically-defined terminal ileitis. Seventeen children were diagnosed with CD and 18 children had idiopathic terminal ileitis (3 lost to followup)
Children with CD had higher prevalence of abnormal C-reactive protein levels, severe inflammation, and radiological evidence of bowel wall thickening compared with children with idiopathic ileitis.
Two children with idiopathic ileitis were later diagnosed with CD; the remaining 13 did not develop CD over a follow-up period of 83 months.
From the data presented, it appeared that the center had a low rate of ileal intubation (316 colonoscopies were excluded for this reason)
75% of those with histologic ileitis had normal endoscopic appearance
When our group looked at colonoscopies (n=374) in our outpatient endoscopy center, we identified isolated ileitis in 10% (6% grossly abnormal, 4% with only histologically abnormal) (related blog post: Our Study: Provider Level Variability in Colonoscopy Yield). Higher rates of ileal intubation (90% in our study) should be considered a quality metric given that 5-10% of children may have disease isolated in ileum.
My take: This study provides reassurance that most children with histologic ileitis will not progress to CD if the ileum is visually-normal (in the absence of abnormal blood tests and/or imaging).
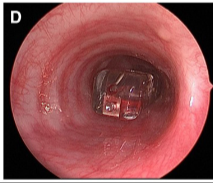
This case report describes placement of a Bravo pH capsule into the bronchus rather than in the esophagus. The complication was quickly recognized and managed by having ENT remove the capsule during the same anesthetic. It is noted that the esophageal mucosal findings included “longitudinal furrows, edema, and mucosal friability.” Biopsies “demonstrated esophagitis consistent with GER.”
Key point:
The authors note that this has led to a change in their practice: “before suction attachment, the endoscope is reintroduced into the hypopharynx to ensure the delivery system enters the cricopharyngeus. This ensures esophageal probe placement before deployment.”
My take: It has been my practice since the Bravo catheter’s inception to assure the deployment catheter is in the esophagus before releasing the Bravo capsule. However, I am impressed with this report. It is very helpful for practitioners to relay difficult experiences to help others avoid complications. This case report should be a reminder also to carefully consider whether a pH study is needed in those with erosive esophagitis.
Previously, there have been numerous posts on this blog discussing iron deficiency anemia in pediatric IBD, including an algorithm by CHOP in 2019 (CHOP QI: Anemia in IBD Pathway) and a NASPGHAN position paper in 2020 (Anemia in IBD -NASPGHAN Position Paper). A recent study from Nationwide Children’s highlights ongoing changes in the approach to this common problem.
This study focused on a quality improvement effort to improve iron deficiency screening in newly-diagnosed patients with IBD. The QI project increased screening from a baseline of 20% to more than 90%. Importantly, this article details a useful algorithm (Figure 4). Key components:
Screen with Ferritin, Iron and TIBC. If Ferritin is less than 30 or iron saturation is less than 20%, it recommends weight-based oral treatment.
If less than 35 kg, options include 3 mg/kg/day (elemental) of ferrous sulfate or Novaferrum. If more than 35 kg, then it recommends ferrous sulfate (325 mg daily=65 mg elemental), ferrous gluconate (325 mg tab bid=36 mg elemental BID), or Novaferrum Ferrex capsule (150 mg daily =150 mg elemental).
Anemia & iron indices are followed every 2-3 months (until improved) and if not resolved, options include either intravenous treatment and/or hematology involvement. For patients less than 50 kg, the authors utilize ferric carboxymaltose (FCM) 15 mg/kg/dose and for those more than 50 kg, FCM at 750 mg dosing.
For IV iron, the authors prefer FCM, which is FDA approved in children 1 yr of age and older, over iron sucrose or iron dextran as the number of infusions needed to replete iron stores is significantly reduced. FCM is a relatively costly IV iron formulation, but can be given over 15 minutes; however, due to fewer infusions, FCM is likely cost-effective.
In the discussion, the authors caution against relying on laboratory reference values for ferritin and iron saturation which often set lower normative values (eg. Ferritin of 7 and iron saturation of 15%).
My take: This QI project provides a good strategy for dealing with iron deficiency anemia in the pediatric population.
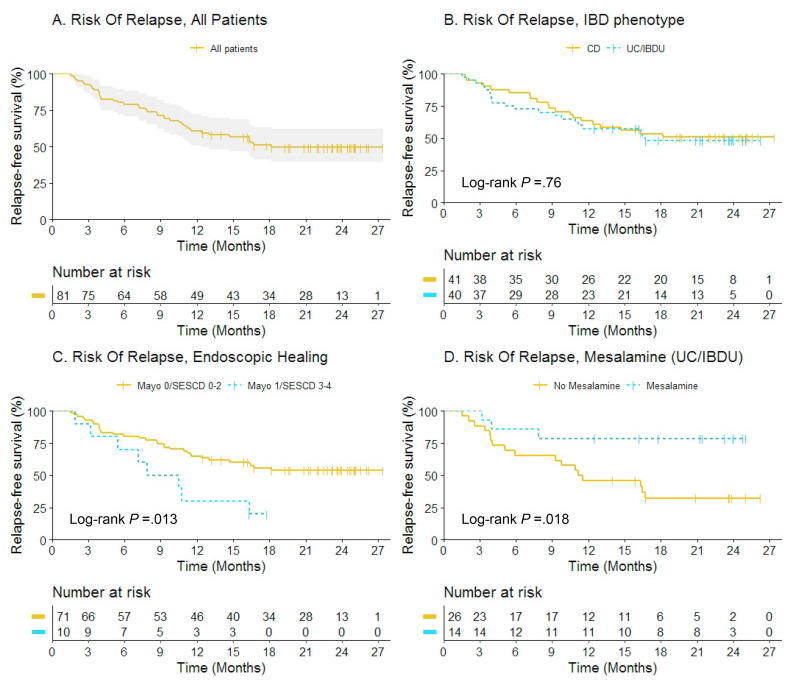
This was a prospective observational study (n=81). In order to participate, patients (all adults) had to be in confirmed baseline steroid-free clinical remission (for at least 6 months) and endoscopic healing; endoscopic healing was defined as endoscopic Mayo score <2 or Simple Endoscopic Score for CD (SES-CD) <5 without large ulcers. Endoscopic healing was subclassified as complete endoscopic healing (Mayo 0/SES-CD 0–2) versus partial endoscopic healing (Mayo 1/SES-CD 3–4).
Key findings:
At 12 months, 70% (7 of 10) versus 35% (25 of 71) of patients with partial versus complete endoscopic healing relapsed, respectively (adjusted hazard rate [aHR], 3.28; 95% confidence interval [CI], 1.43–7.50)
Mesalamine use was associated with fewer relapses in UC/IBDU patients (aHR, 0.08; 95% CI, 0.01–0.67)
Thirty patients restarted anti-TNF, and clinical remission was regained in 73% at 3 months.
The authors highlight the lower relapse rate between those with complete endoscopic healing and those with partial healing. They acknowledge that those eligible for anti-TNF de-escalation are highly selected (~7% in a prior study) and “few patients with an unfavorable IBD phenotype, such as stricturing or penetrating CD, anti-TNF for perianal fistulizing CD, young age at diagnosis, or prior biological failure, were included in this study. Therefore, our findings may not be generalizable to patients with a more severe IBD phenotype.
My take: Even in those with complete endoscopic healing, there is a high rate of relapse. In addition, stopping anti-TNF therapy likely increases risk of not responding to anti-TNF therapy when it is restarted. This study does show that transitioning from anti-TNF therapy to mesalamine therapy in those with ulcerative colitis (or IBDU) could be a reasonable consideration.
Two recent bowel sound podcasts had some useful clinical insights. Some of my summation below could be off a bit as I tend to listen to these while driving. So, it may be a good idea to hear the podcasts for yourself.
Victoria Martin discussed cow milk intolerance/allergic proctocolitis.
Dr. Martin emphasized the importance of challenging children with these diagnoses; in many, the disorder is transient. A challenge is typically done 1 month after resolution of symptoms. In those with confirmed reactions, rechallenge 6 months later is typical. The reasons for doing this:
This is in keeping with international guidelines
Many children do not need to stay on expensive formulas or dietary restrictions (if breastfed)
This is likely to reduce the risk of developing lifelong food allergies
Other pointers: generally it is not helpful to follow stool heme testing (high number of normal infants with heme-positivity). Stool calprotectin is not helpful (wide variability in infants). Flexible sigmoidoscopy is rarely needed. In those with mild symptoms, it may be reasonable to watch without intervention, especially in breastfed infants.
In terms of diagnosis, Dr. Langer recommended use of rectal suction biopsy as 1st step in smaller kids (less than 1 yr of age) and rectal manometry as 1st step in those older than 1 yr of age. He reviewed the three main operations:
Swenson -pulldown to anus
Duhamel -pouch: with an end-to-side anastomosis is performed with the remaining rectum
Soave -cuff: strip mucosa and leave a muscular cuff
He noted that he prefers Soave but that there is not clear superiority of one operation.
Other pointers:
Enterocolitis is #1 cause of mortality. If someone is coming in sick, worthwhile to start an in-and-out irrigation promptly. Irrigation information can be found on YouTube. From Colorado Children’s: Rectal Irrigations for Hirschsprung
He pioneered the use of Anal Botox for children post-operatively. Many children with obstructive symptoms related to sphincter malfunction will improve with time and this often allows a child to avoid a myectomy
He described workup for post-operative soiling and potential pathophysiology: muscle issues (manometry), sensory issues, functional retention with overflow, and hypermotility (sigmoid propelling stool rapidly which may improve with imodium)
Dr. Langer is also a musician — you can listen to his music here.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
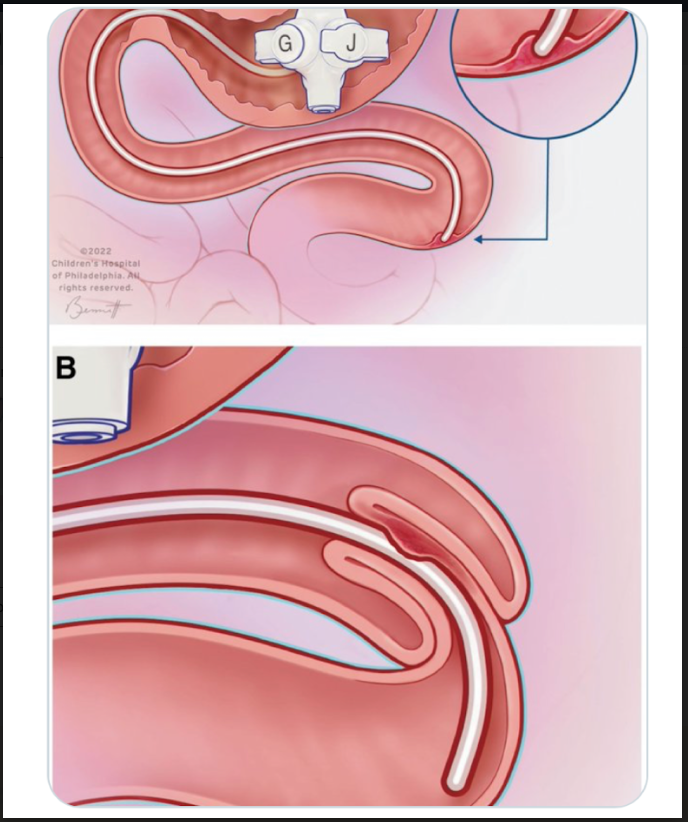
In this retrospective study, 46 GJ intussusceptions were identified; patients had a median age of 2.8 years. Key findings:
There were 7 recurrences (15.2%).
There was no difference in recurrence based on time of bowel rest (5 days in those without vs 6 days in those with, P = 0.30) nor a difference in recurrence with <72 hours of bowel rest compared to >72 hours (1/15, 6.7% vs 6/31, 19.3%)
In 15 patients who had a smaller GJ tube replaced, there were no recurrences compared with 7 recurrences among 29 (24%) that had the same caliber GJ tube replaced (P=0.08)
My take: This study indicates that prolonged removal of GJ is not needed with GJ intussusception and if feasible, consider replacement with a smaller (or shorter) GJ tube.