A Baccarella et al. Clinical Gastroenterology and Hepatology; 2025; 23: 2242 – 2252. Open Access! Outcomes of Allogeneic Hematopoietic Stem Cell Transplant in Monogenic Inflammatory Bowel Disease
This was a retrospective single-center (CHOP) study of 25 children with monogenic IBD who underwent Hematopoietic Stem Cell Transplant (HSCT) (2012-2022).
Key findings:
- Seventy-two percent of patients had Crohn’s Disease, and 28% were classified as IBD-unspecified. Ninety-two percent of patients had VEO-IBD, 56% presenting under age 1
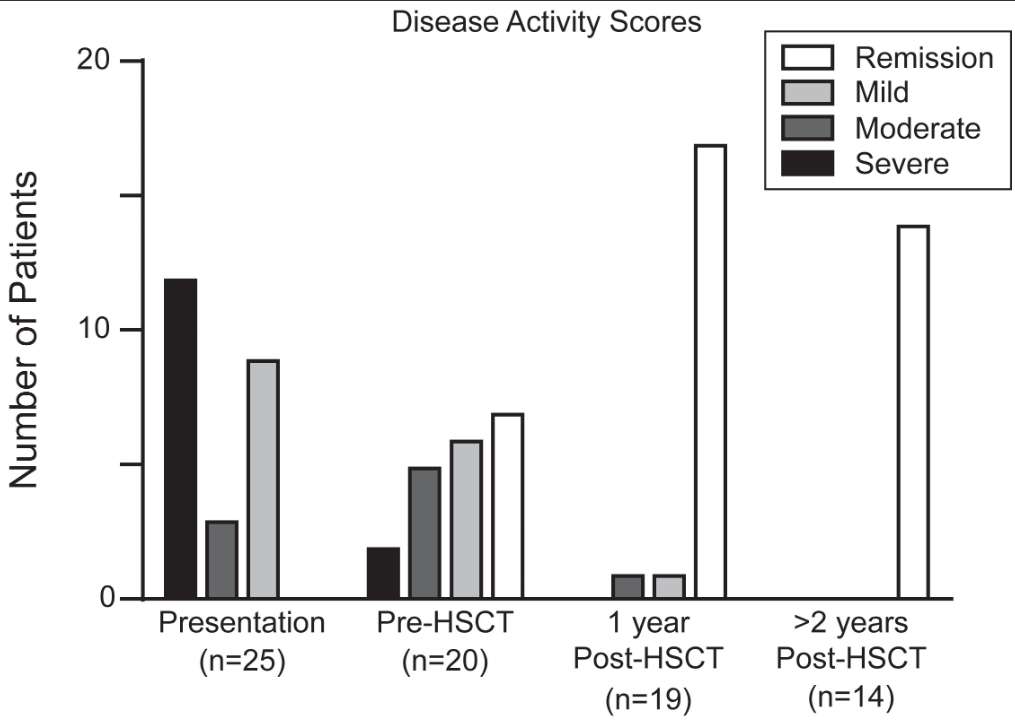
- At most recent follow-up, 92% of patients achieved sustained medication-free remission of IBD and 60% with prior ostomy underwent re-anastomosis. There was 100% survival at a median follow-up of 3 years
- There was significant improvement in growth, hospital days, and severe infections
Discussion points:
- “Delay of HSCT with the goal of obtaining remission of IBD prior to transplant may prove to be determinantal, as outcomes of HSCT are in general improved for younger patients,20 and medical remission is often unattainable for more severe forms of monogenic IBD. Within our cohort, 32% of patients had moderate or severe disease at the time of transplant despite medical optimization. None of these patients developed intestinal GVHD, which was a rare event in our total cohort”
- “HSCT is not without risk, and complications occurred in our cohort, at rates typical of other IEI cohorts”
- “The selection of patients who would benefit from HSCT requires multidisciplinary discussion.”
With regard to patient selection, one item that was not included in the discussion was the one patient excluded from their analysis who had a TTC7A gene defect. In the results section, it was explained that the patient with “TTC7A was subsequently excluded as transplant was performed for the indication of SCID alone, rather than treatment of intestinal disease.” More discussion on this point is merited as many centers would NOT have a patient with TTC7A undergo HCST specifically because it cannot correct the underlying bowel disease.
Also, it was noted that one patient with CTLA4 deficiency had undergone HSCT prior to the discovery of the genetic defect. With the more widespread use of genetic testing available now, this discovery may have obviated the need for HSCT as treatment with abatacept is typically effective.
My take: Overall, the authors present impressive results for HSCT for monogenic IBD and strengthen the need for genetic testing in those with early onset disease and those refractory to treatment.
Related blog posts:
- A Medical Wolf in Sheep’s Clothing – Monogenetic Diseases Not So Rare
- Immune Dysregulation and Inflammatory Bowel Disease
- Underlying Genetic Disease in Pediatric Inflammatory Bowel Disease
- How Very Early Onset-Inflammatory Bowel Disease is Different, Plus One | gutsandgrowth
- When To Perform Genetic Testing In The Setting Of Inflammatory Bowel Disease | gutsandgrowth
- VEO-IBD -Useful “Position” Paper Is Really A Review
- Endoscopy Complications in Hematopoietic Stem Cell Transplantation Population
- Targeted Therapy for Autoinflammatory Very Early Onset Inflammatory Bowel Disease
- Patterns and Puzzles with VEO-IBD This is a very good review and the image on this day has one of my favorite patient t-shirts.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.