N Ovchinsky et al. The Lancet Gastroenterology & Hepatology, Volume 9, Issue 7, 632 – 645. Open Access! Efficacy and safety of odevixibat in patients with Alagille syndrome (ASSERT): a phase 3, double-blind, randomised, placebo-controlled trial
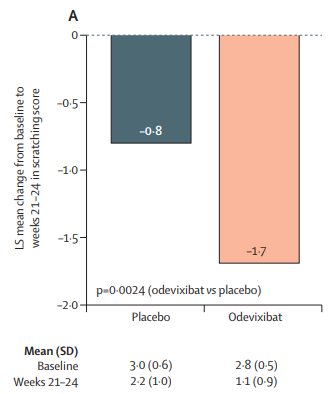
Methods: “The ASSERT study was a phase 3, double-blind, randomised, placebo-controlled trial that enrolled patients at 21 medical centres or hospitals in ten countries” with 52 patients (enrolled 2021-2022). “The primary efficacy endpoint was change in caregiver-reported scratching score (on the PRUCISION instrument; range 0–4) from baseline to weeks 21–24.” The treatment group received odevixibat 120 µg/kg per day.
Key findings:
- There were improvements in both scratch scores and bile acid concentrations
- There were improvements in sleep parameters including falling asleep and ability to sleep without a caregiver
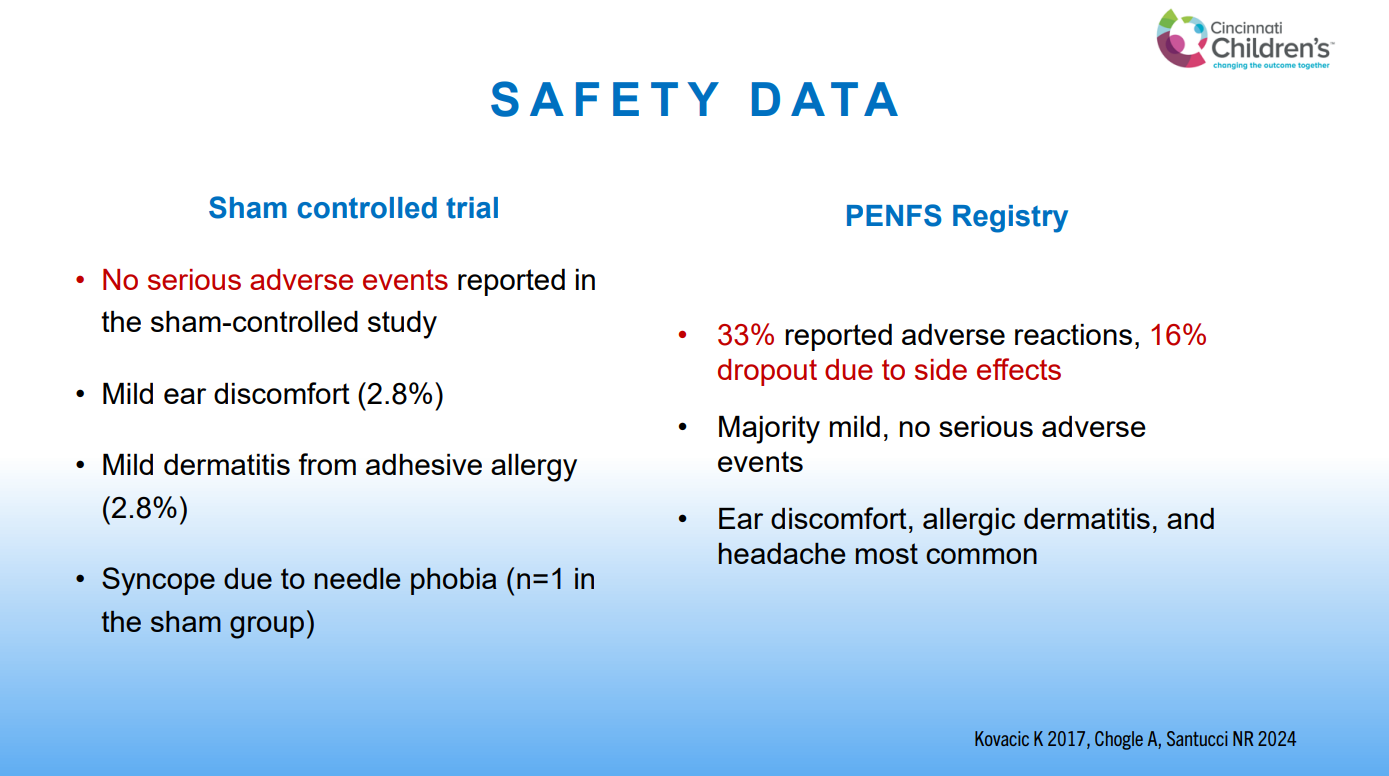
- Adverse events: diarrhea was reported in ten (29%) of 35 patients who received odevixibat and in one (6%) of 17 patients who received placebo; all cases were mild in severity and no cases of diarrhea led to treatment interruption or discontinuation
Scratch Scores:

Bile Acid Levels


Other points:
- Overall, 50 (96%) of the 52 patients chose to enter the open-label extension study
- The authors note that this is the first randomized placebo-controlled trial for Alagille syndrome
- A direct comparison of odevixibat and maralixibat in patients with Alagille syndrome is complicated by differences in study design and endpoints across the their studies
My take (borrowed in part from authors): “As pruritus is a major driver of liver
transplantation in patients with Alagille syndrome, these results suggest that odevixibat could have the potential to delay or prevent liver transplantation”
Related blog posts:
- Relooking at 6-Year Data of Maralixibat for Alagille Syndrome
- Lecture: IBAT Inhibitor for Alagille Syndrome
- Aspen Webinar 2021 Part 3-IBAT Inhibitors
- Year-in-Review for Pediatric Hepatology
- GALA: Alagille Study
- NASPGHAN Alagille Syndrome Webinar
- Intracranial Hypertension & Papilledema with Alagille Syndrome
- Explaining Differences in Disease Severity for Alagille Syndrome