Yesterday was “National Dog Day.” Here’s our pooch:

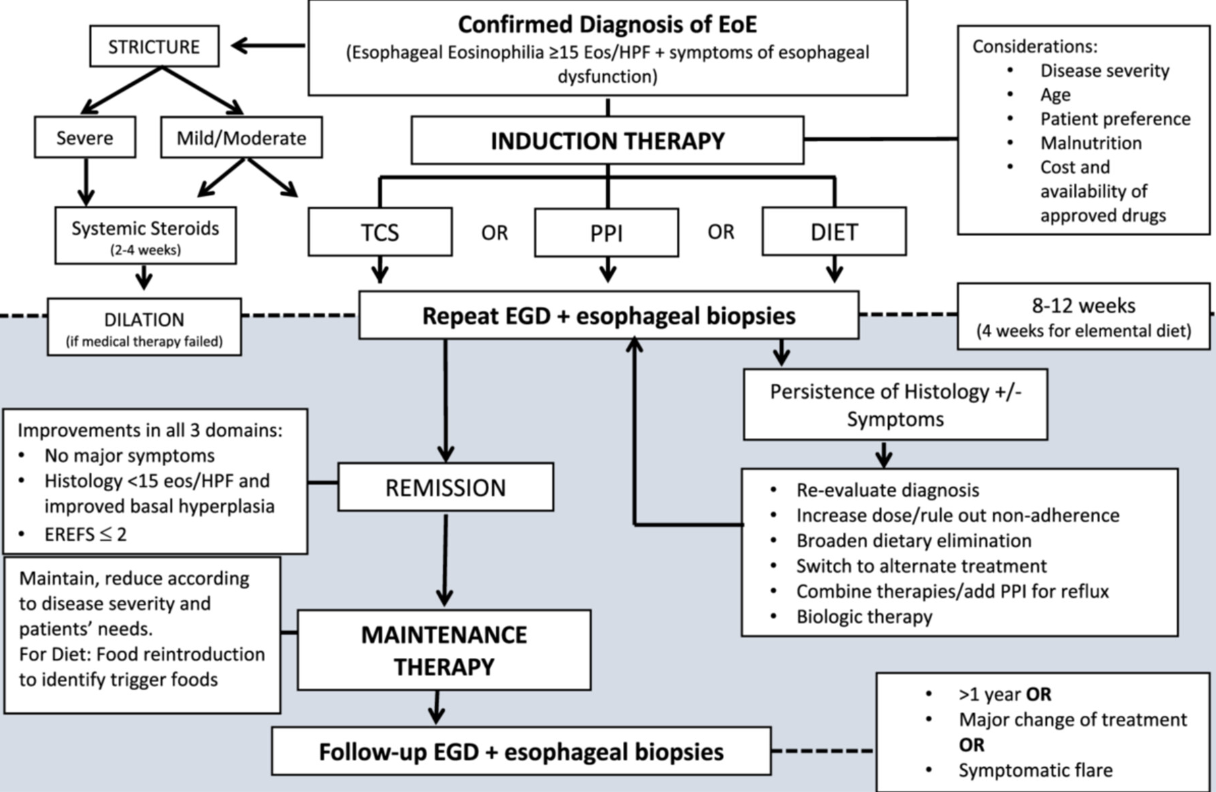
J Amil-Dias et al. JPGN;79:394–437. Open Access! Diagnosis and management of eosinophilic esophagitis in children: An update from the European Society for Paediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN)
This report makes 52 statements and 44 recommendations. Overall this is a helpful report but there are many statements and recommendations that have NO value for pediatric gastroenterologists (except for those trapped in a cave for the last 10 years). Here are a couple examples of that:
- “ESPGHAN EGID WG recommends that pediatricians should be aware of the higher incidence of EoE in relatives.”
- “ESPGHAN EGID WG recommends that a high index of suspicion for EoE must be maintained in children with concomitant atopic disease.”
- “ESPGHAN EGID WG recommends the peak value of 15 eos/HPF as the cut‐off value in esophageal biopsy specimens, for the histological diagnosis of EoE in an appropriate clinical context”
Some helpful recommendations:
- “ESPGHAN EGID WG recommends against using available allergy tests to predict dietary triggers of EoE.” This is not new information but helpful to have clearly stated in guidelines.”
- “ESPGHAN EGID WG recommends maintenance therapy to all patients after achieving histological remission” Commentary: “There are no prospective data on the best duration of maintenance therapy in pediatric EoE…[In a large study of adults} sustained untreated combined remission was seen in only 1.3% of patients who discontinued treatment.”
- “ESPGHAN EGID WG suggests endoscopic and histological re‐evaluation after 1‐3 years during the maintenance phase in cases of stable clinical remission”
- “ESPGHAN EGID WG recommends that dupilumab can be used in selected cases of children over1 year old weighing >15 kg with EoE refractory to conventional treatment and in those with concomitant atopic burden with approved indications for biologics”
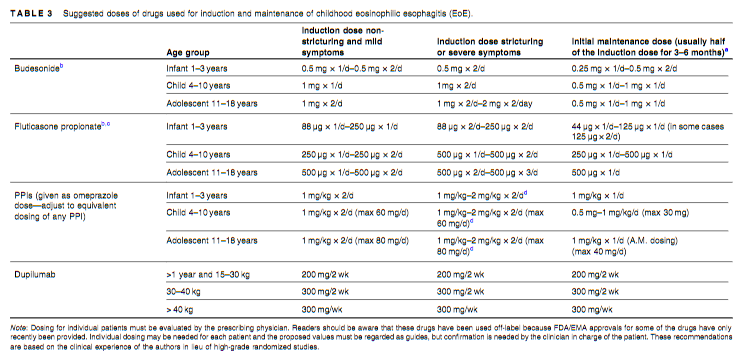
- “ESPGHAN EGID WG suggests that a short course of systemic steroids be considered as an alternative to dilation in the presence of moderate to severe esophageal strictures with severe symptoms.” “Treatment with short term systemic steroids can significantly reduce the need for mechanical esophageal dilation in moderate to severe strictures associated with pediatric EoE”
- Suggested drug dosing is noted in Table 3 (see below)
Related blog posts:
- Practical Tips for Eosinophilic Esophagitis (Dr. Glenn Furuta lecture)
- Eosinophilic Esophagitis -Up to Date Dietary Management Review
- I-SEE (Index of Severity for Eosinophilic Esophagitis) Works in Kids Too
- Long Duration of Eosinophilic Esophagitis Associated with a Stiff Esophagus
- Dupilumab (Dupixent) for Young Children with Eosinophilic Esophagitis (Published Data)
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.