CA Taylor et al. MMWR 3/18/22, Open Access: COVID-19–Associated Hospitalizations Among Adults During SARS-CoV-2 Delta and Omicron Variant Predominance, by Race/Ethnicity and Vaccination Status — COVID-NET, 14 States, July 2021–January 2022
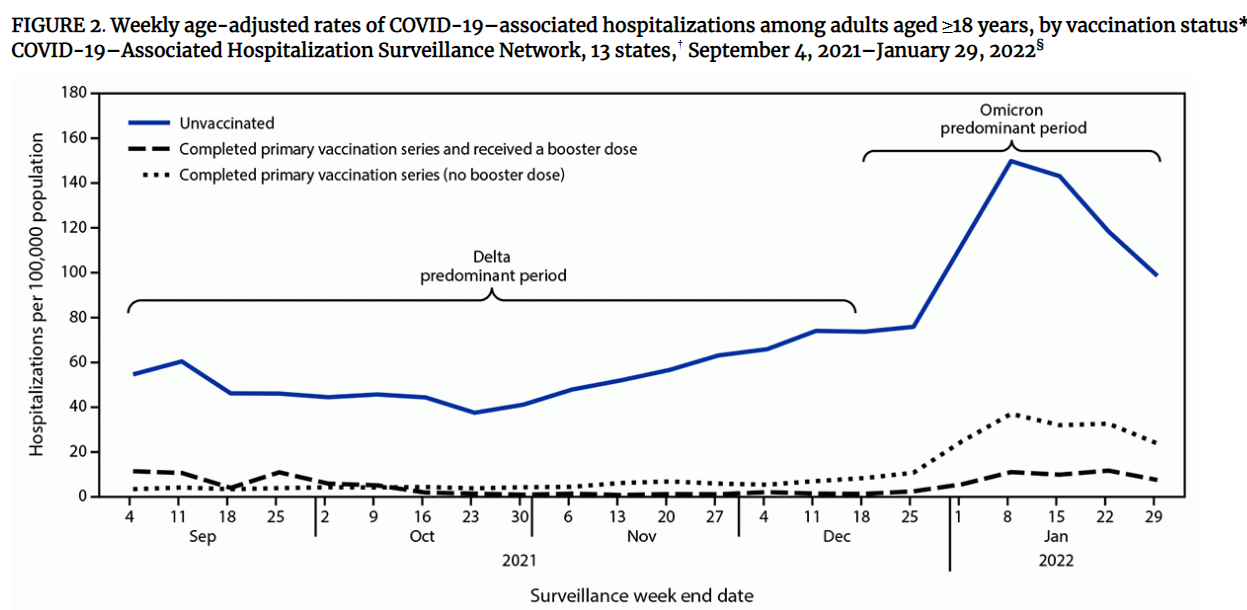
- During the omicron wave, hospitalization among unvaccinated adults remained 12 times the rates among vaccinated adults who received booster or additional doses and four times the rates among adults who received a primary series, but no booster or additional dose.
- The rate among adults who received a primary series, but no booster or additional dose, was three times the rate among adults who received a booster or additional dose

- A previous study conducted before the Omicron-predominant period that showed increased risk for COVID-19–associated hospitalization among certain racial and ethnic groups, including Black adults, and suggested the increased hospitalization rates were likely multifactorial and could include increased prevalence of underlying medical conditions, increased community-level exposure to and incidence of COVID-19, and poor access to health care in these groups
- The increase in transmissibility of the Omicron variant might have amplified these risks for hospitalization…the increased risk for hospitalization among Black adults during the Omicron-predominant period might also be due, in part, to lower proportions of Black adults receiving both the primary vaccination series and booster doses
My take: This study shows the value of getting vaccinated and booster shot. I would speculate that many of the unvaccinated have had previous infections and this further indicates that vaccination may provide greater protection than immunity following infection.