So sad to hear that Jim Heubi has passed away. Jim Heubi was the person I interviewed with when I was considering where to do my pediatric residency and he helped convince me to come to Cincinnati. During my fellowship, I came to admire how he was so good at everything though it was always unassuming. He was such a kind person in addition to being a mentor and role model.
More from Aspen Webinars. This blog entry has abbreviated/summarized several presentations. Though not intentional, some important material is likely to have been omitted; in addition, transcription errors are possible as well.
Dr. Mieli-Vergani presented case report of a boy with autoimmune sclerosing cholangitis and associated colitis who presented with minimal symptoms.
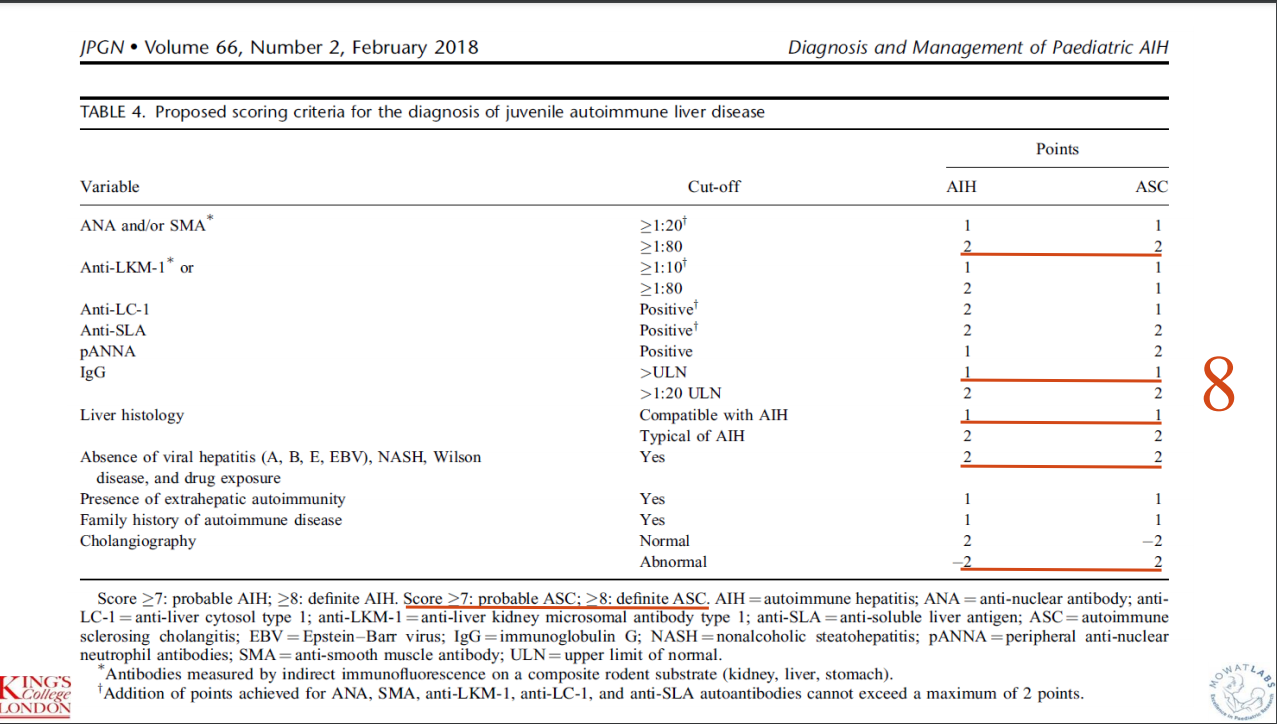
This case report highlights the evaluation and management of autoimmune liver disease hepatitis. Workup included autoimmune serology, GGT, celiac serology, calprotectin, and ultrasonography. EGD-Colonoscopy was prompted by elevated calprotectin. MRCP was prompted by elevated GGT (GGT were normal at the time of biopsy and MRCP) and liver biopsy findings.
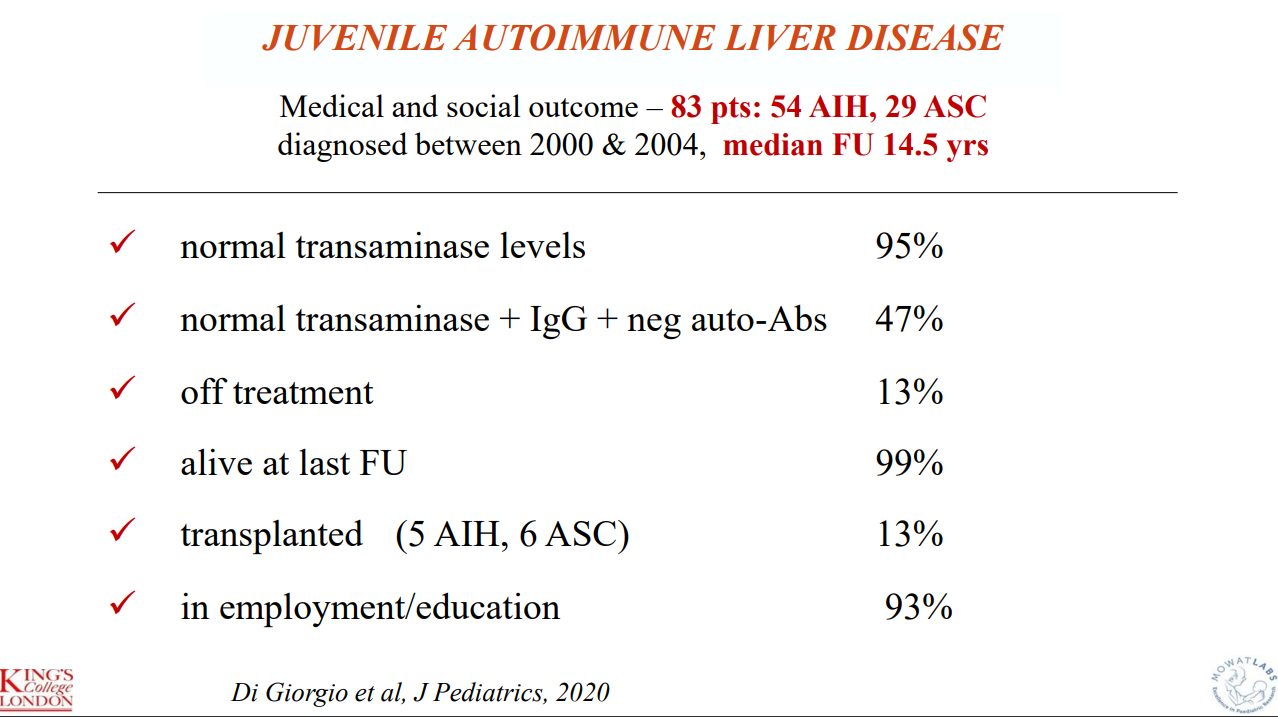
“My message is that MRCP and colonoscopy should be done in all cases of autoimmune liver disease in children and adolescents, irrespective of calprotectin levels or elevated GGT and biliary changes on histology, as both IBD and sclerosing cholangitis can be present without any of the classical symptoms and signs. Only by doing this it is possible to reach an early diagnosis which is essential for early treatment and for a good outcome.”
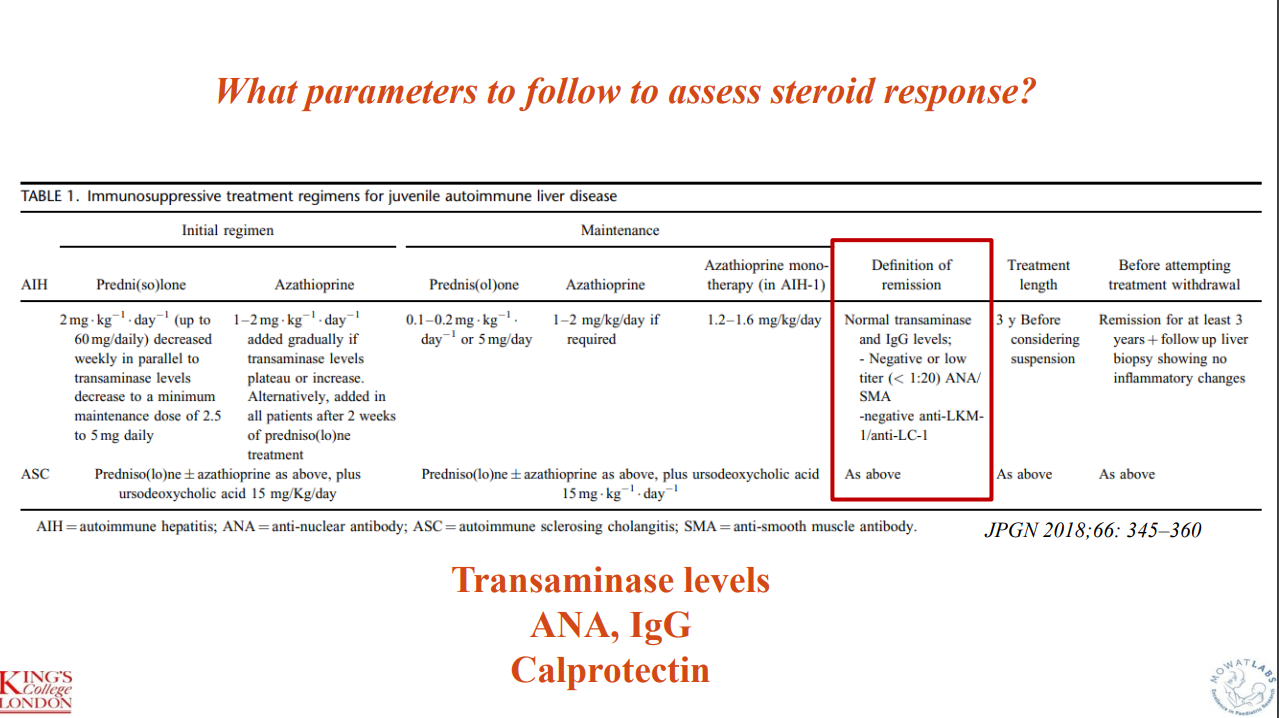
Outcome data indicate that 11 of 83 (13%, 5 AIH, 6 ASC)) required transplantation. “I have shown our long-term outcome data not to stress the number of patients who have required transplantation, but the number of patients who are well and have a normal life after over 14 years of follow-up. This can be only achieved if one thinks of autoimmune liver disease even if the child appears to have something non-specific, initiating correct treatment for the liver, and the gut if there is bowel disease, as soon as possible. At the beginning, treatment should be monitored very closely (at least weekly), to be able to decrease the dose of steroids swiftly, introduce azathioprine if needed, and avoid side affects.”
Key points:
Budesonide is not a good substitute for prednisone in autoimmune hepatitis
Mycophenolate is frequently used as a 2nd line agent
Consider calprotectin in patients with autoimmune liver disease to screen for IBD (though calprotectin can be falsely-negative)
Consider followup liver biopsy after normalization of liver enzymes for ~3 yrs (when consideration of stopping medications)
Recommends MRCP for all patients with AIH
Some slides:
Key points:
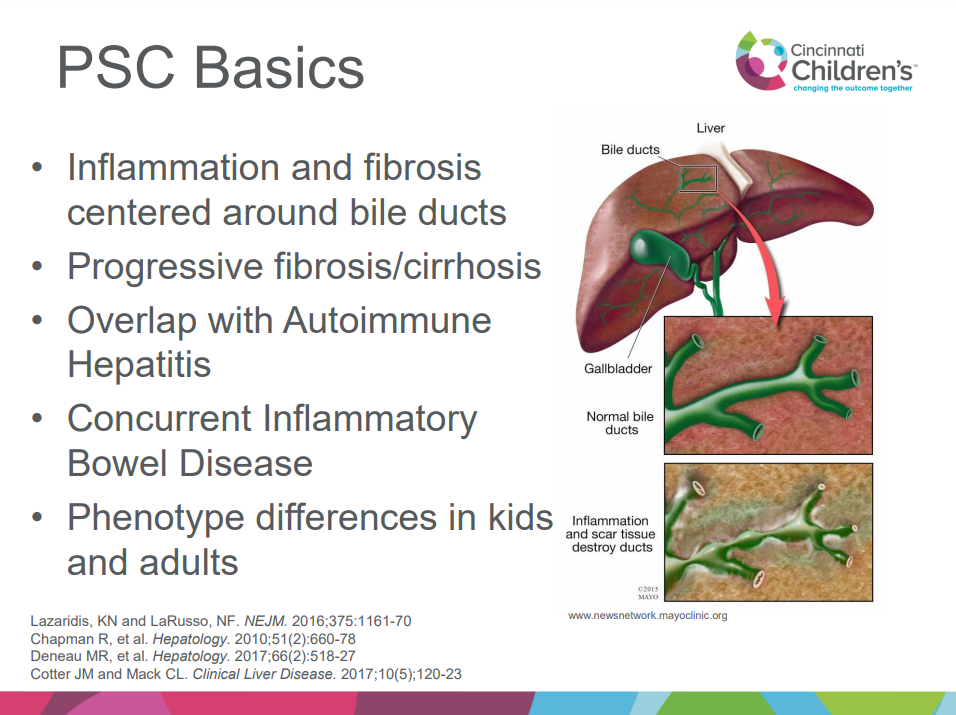
Better understanding of immune basis of PSC is developing
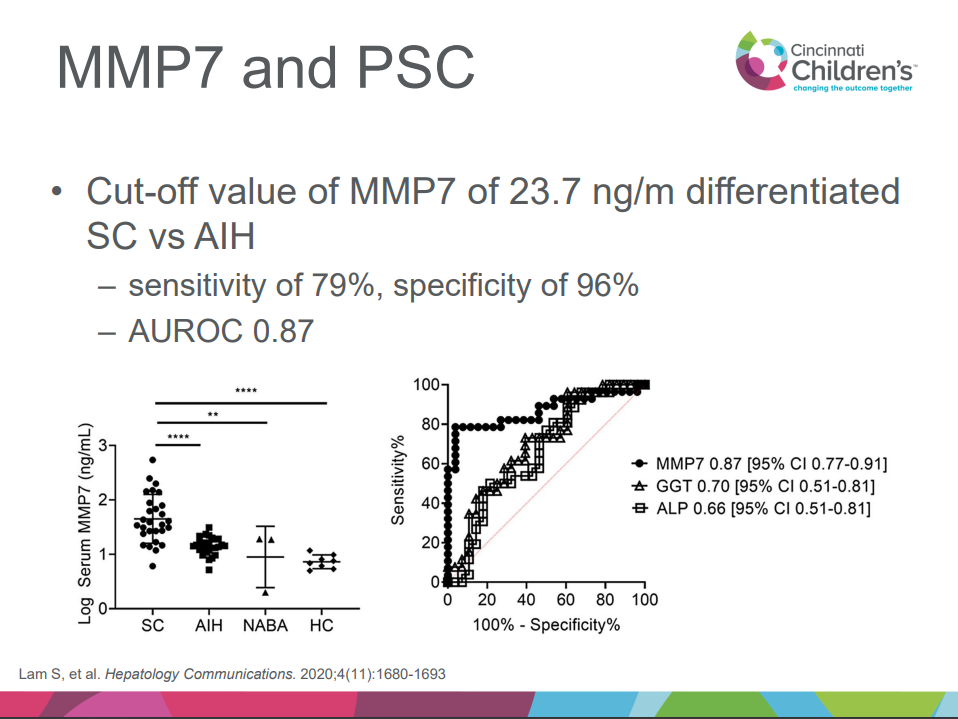
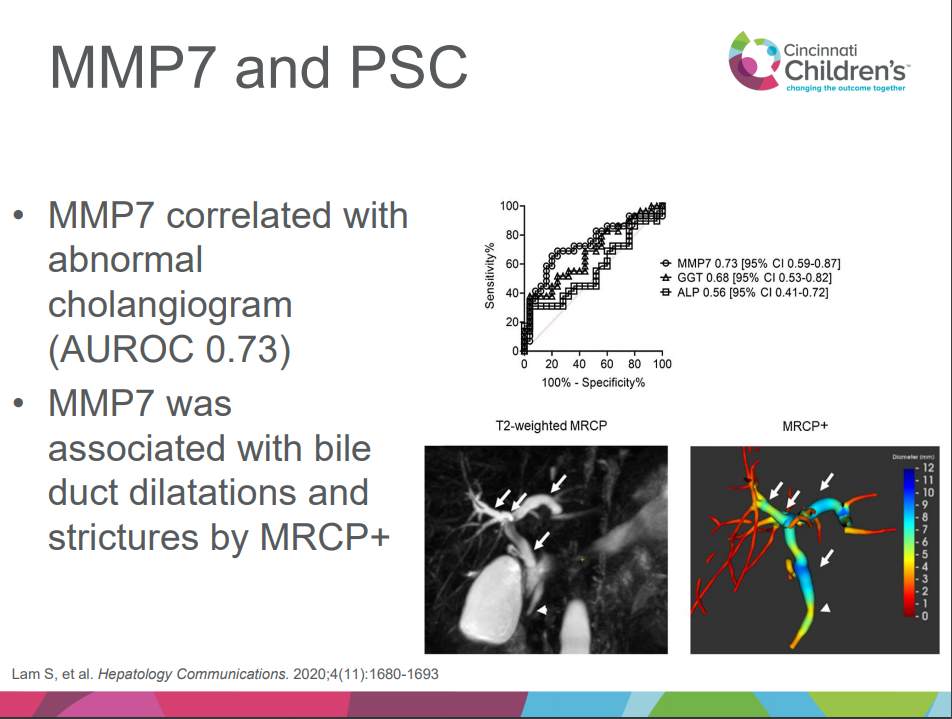
MMP-7 appears to help differentiate PSC/ASC from AIH
Small duct PSC is more common in children
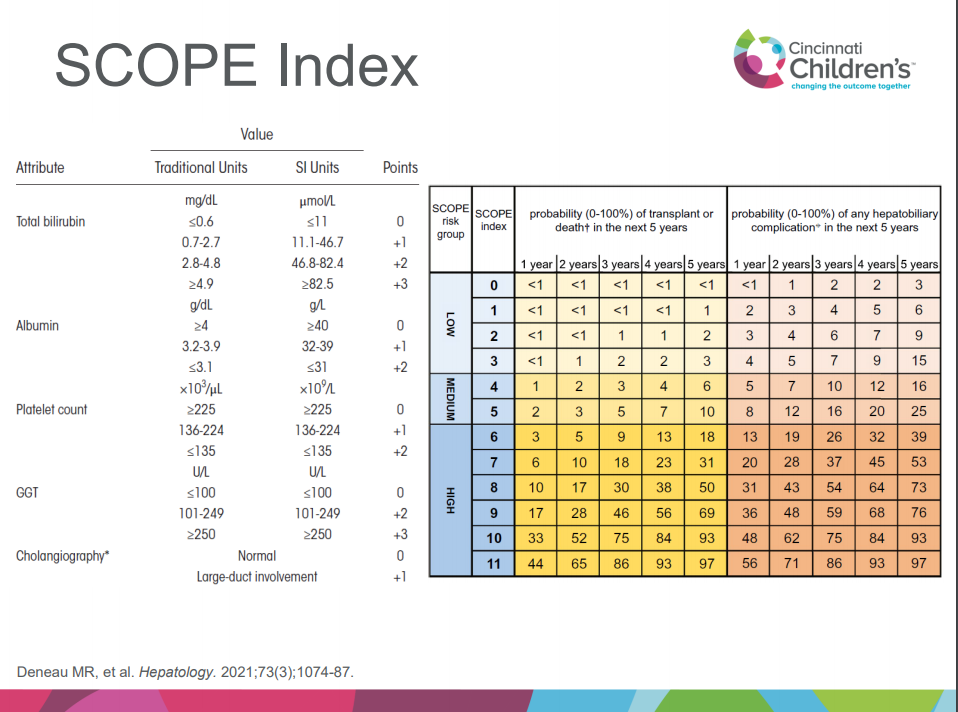
SCOPE index can help predict outcomes
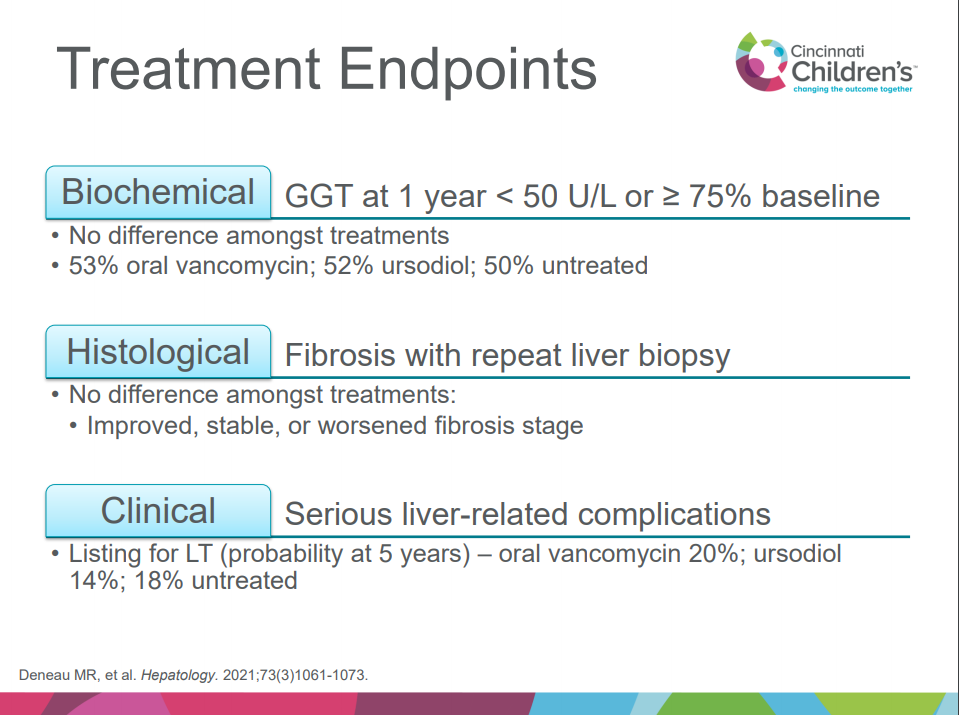
Treatment: no clear benefit of vancomycin, ursodeoxycholic acid compared to placebo but need for randomized controlled study
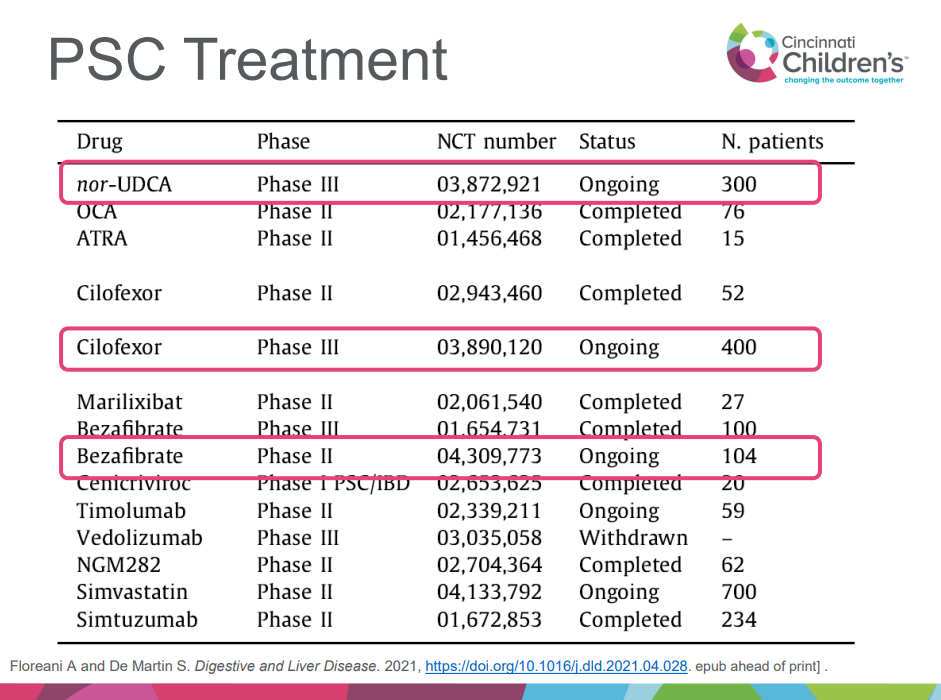
Several studies of new agents for PSC in adults are ongoing, including nor-UDCA, cilofexor, bezafibrate
Vedolizumab does not appear to be effective for PSC
Child with FTT, elevated LFTs, sporadic mild hypoglycemia, and neurologic symptoms. DDx: congenital disorders of glycosylation (CDG), mitochondrial d/o, peroxisomal d/o, urea cycle d/o and lysosomal d/o. Diagnosis was made after liver biopsy and whole exome sequencing (which showed PMM2 mutations). Diagnosis of most CDG can be made by serum transferrin isoforms. Discussion among many participants noted that liver biopsy often not needed in age of genetic testing.
More from Aspen Webinar 2021. This blog entry has abbreviated/summarized several presentations. Though not intentional, some important material is likely to have been omitted; in addition, transcription errors are possible as well. An excellent review from Dr. Sokol.
What’s New with IFALD Ronald Sokol
Key points:
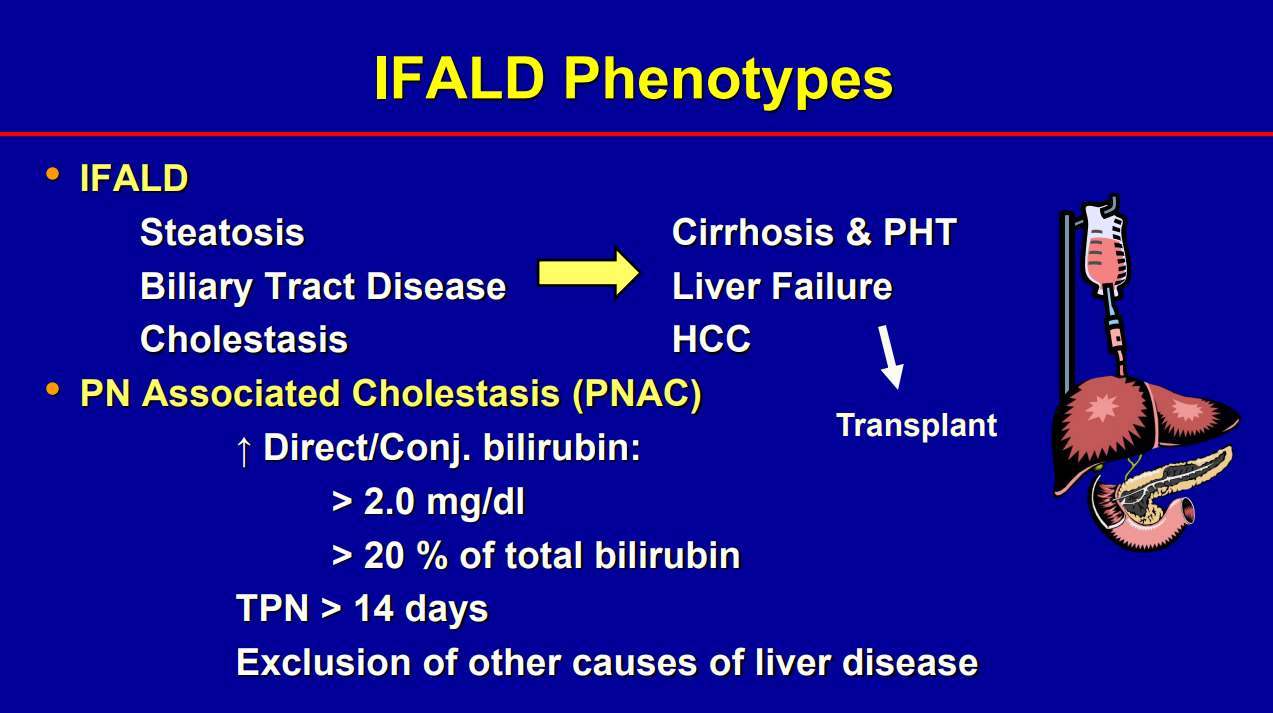
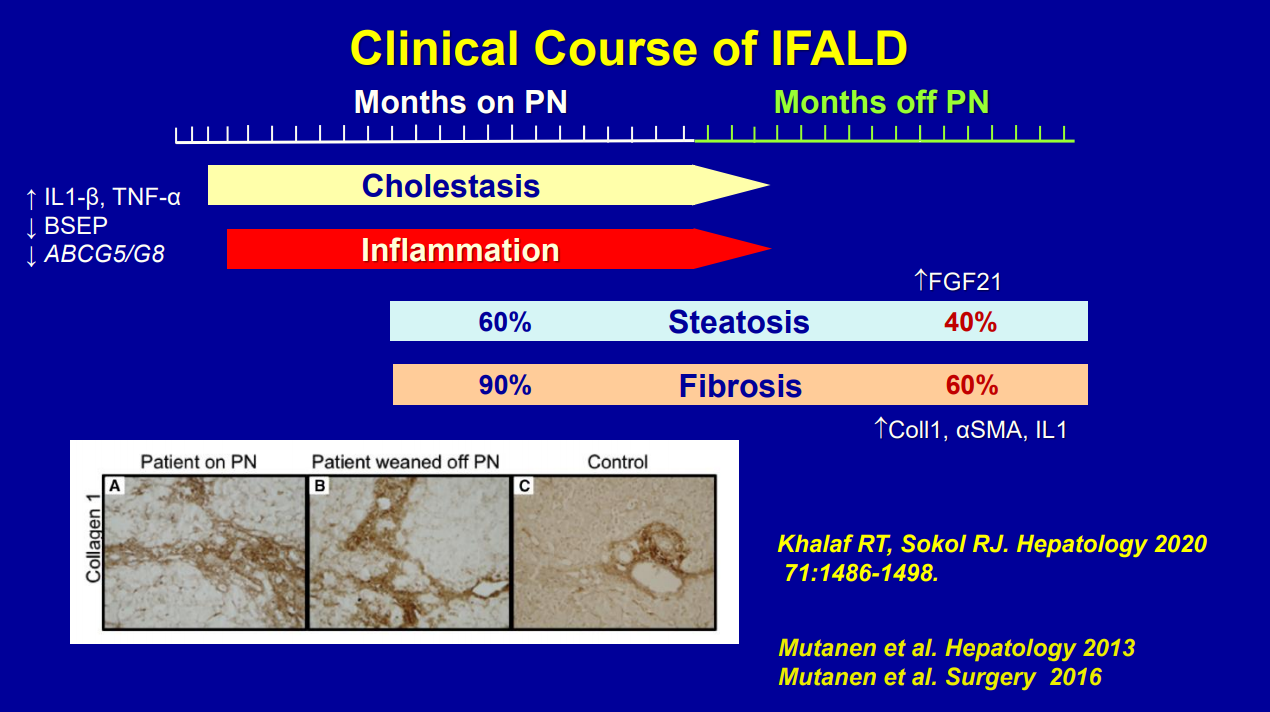
Biliary cirrhosis related to parenteral nutrition has been the major indication for small bowel transplantation/multi-visceral transplantation. IFALD presentations: Steatosis, biliary tract disease and cholestasis
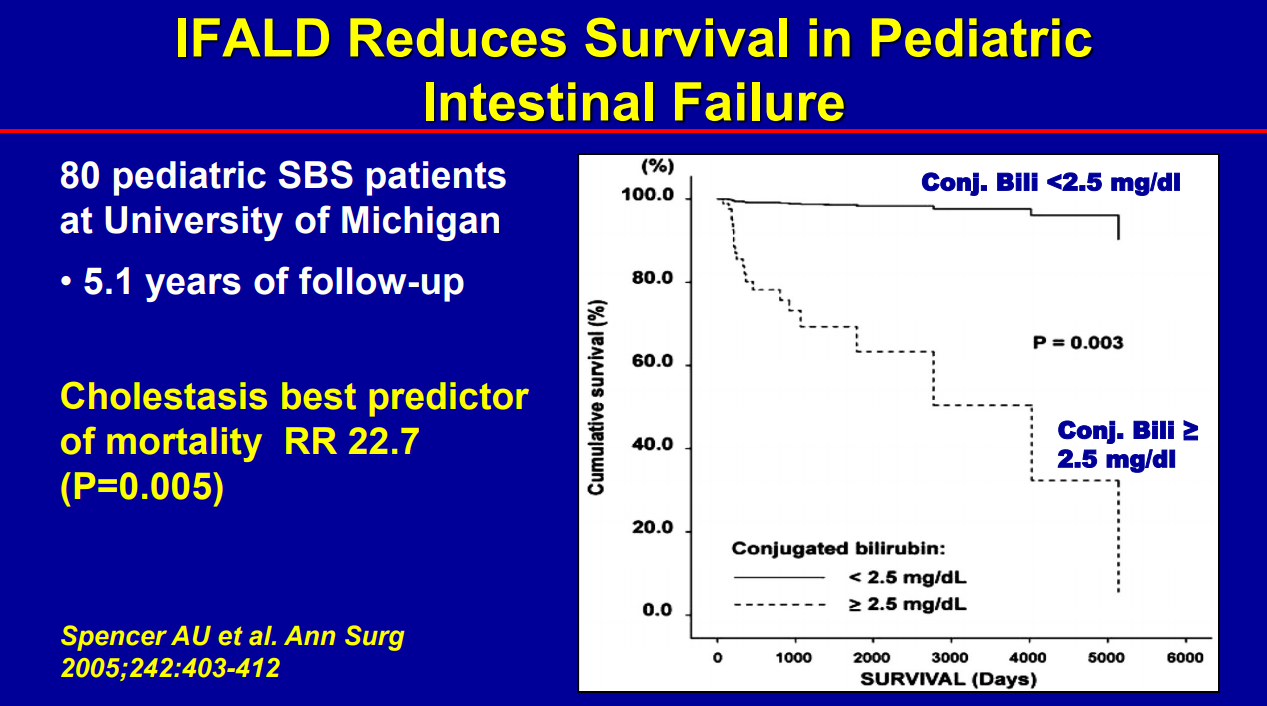
Conjugated bilirubin >2.5 had RR 22.5 for mortality (prior to availability of intestinal transplantation)
Even after weaning off PN, studies have shown long-lasting fibrosis and steatosis in more than 40% of patients (>8 yrs off PN)
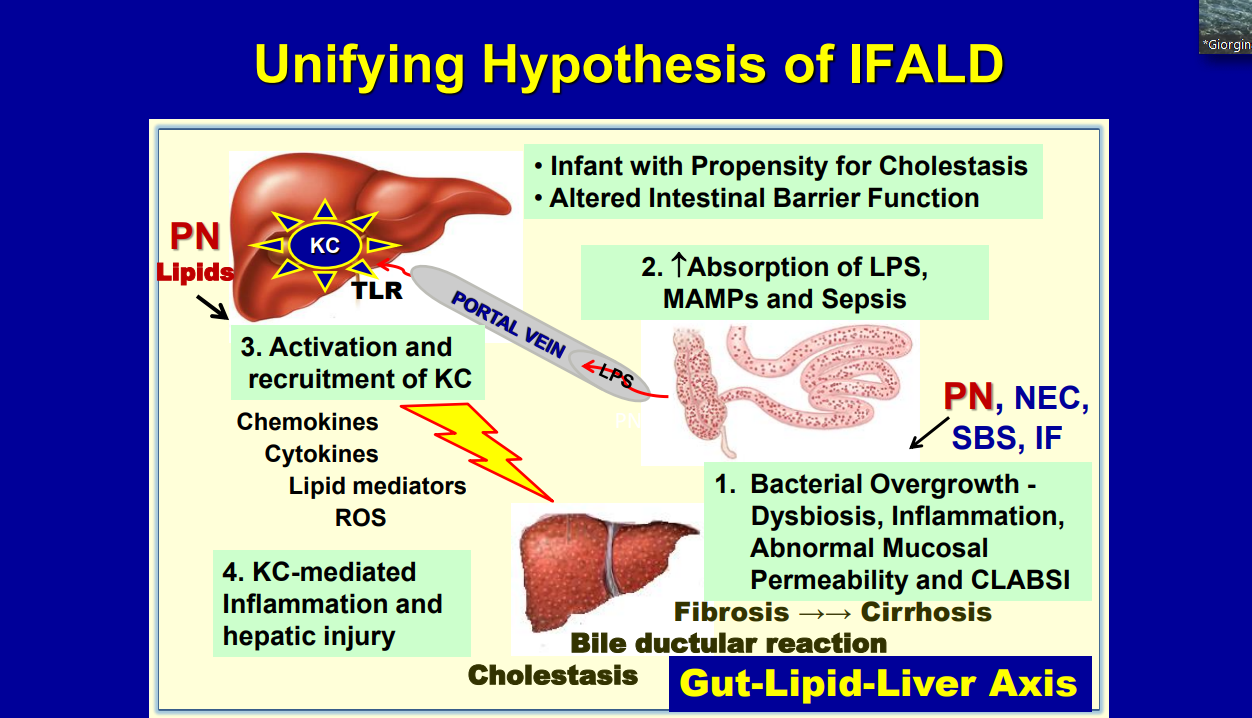
Intestinal microbiome is altered in patients with IFALD
Puder M et al. (Ann Surg 2009; 250: 395) showed that fish oil (at lower doses) was associated with improvement/resolution of parenteral nutrition associated cholestasis (PNAC)
Lipid reduction also is associated with cholestasis resolution
Caution with Fish oil (omegaven): 1. Does not prevent hepatic fibrosis progression 2. Reduction of lipid doses can have negative effects on brain growth
Lipid management has been crucial in reducing the number of children needing intestinal transplantation
Some of the slides:
IBAT Inhibitors Frederick Suchy
Key points:
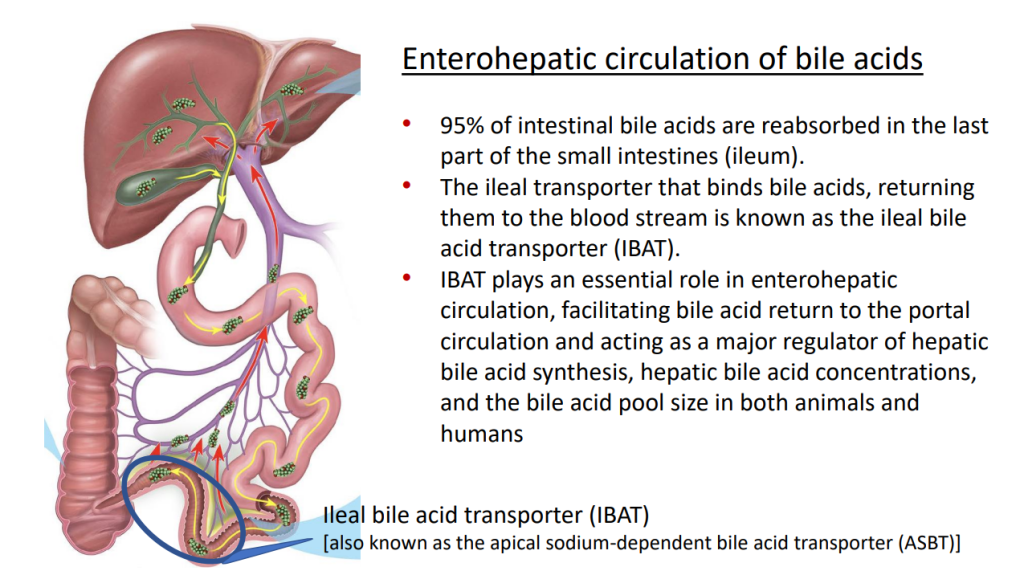
IBAT inhibitors block intestinal absorption of bile acids/disrupt enterohepatic circulation; this leads to augmented bile acid excretion in stools
IBAT inhibitors may reduce liver damage in the setting of cholestasis/accumulation of toxic bile acids
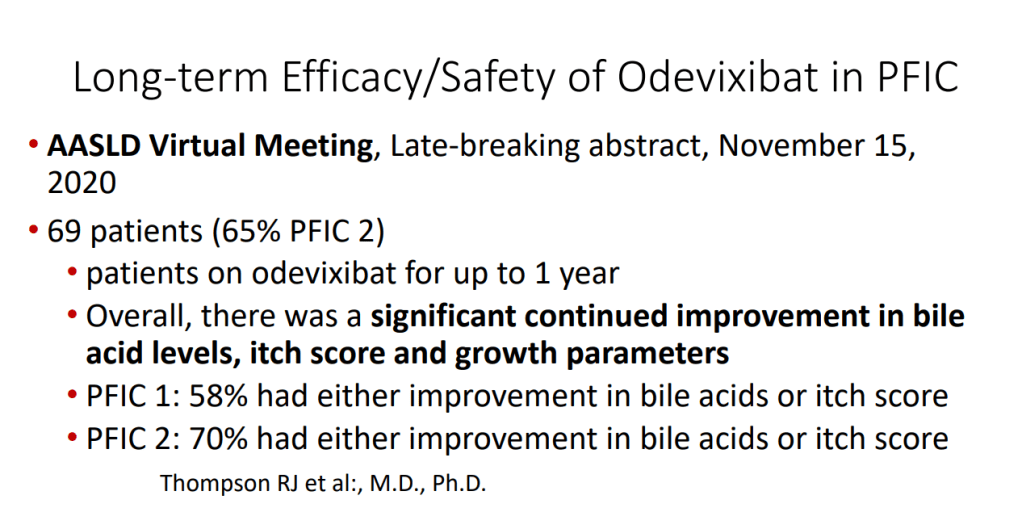
Potential diseases for IBAT inhibitors include Alagille syndrome and PFIC
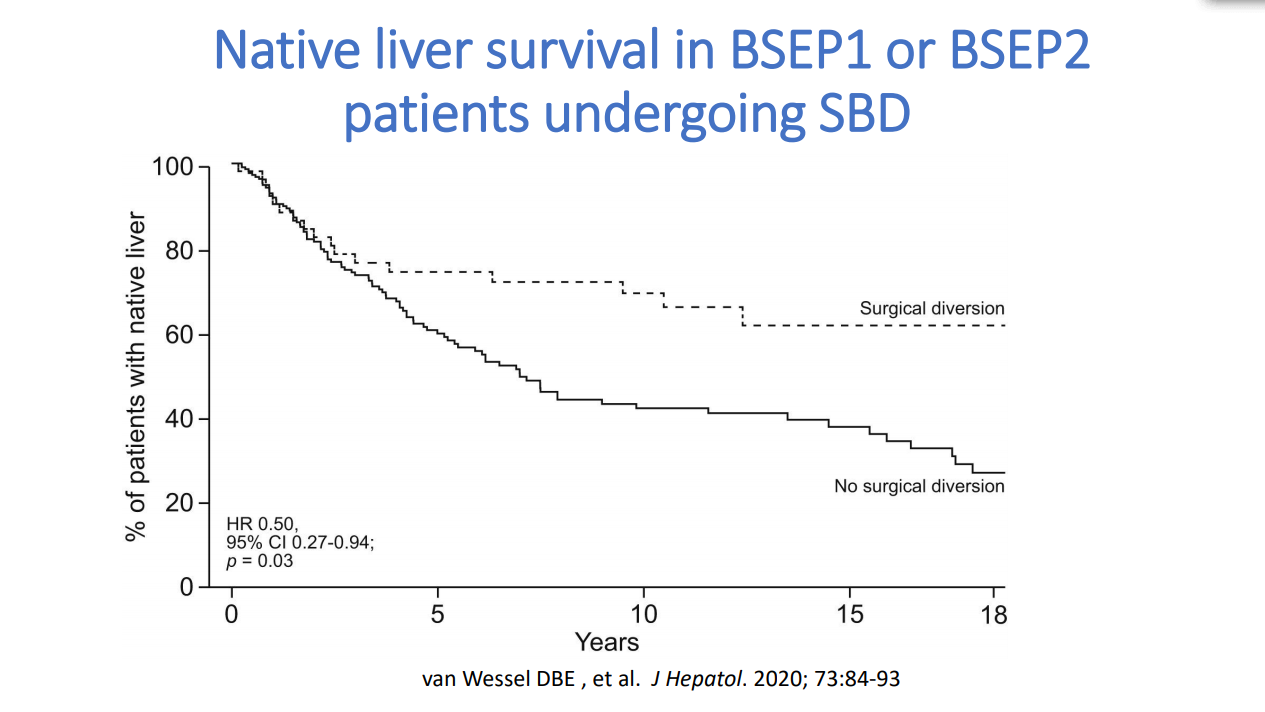
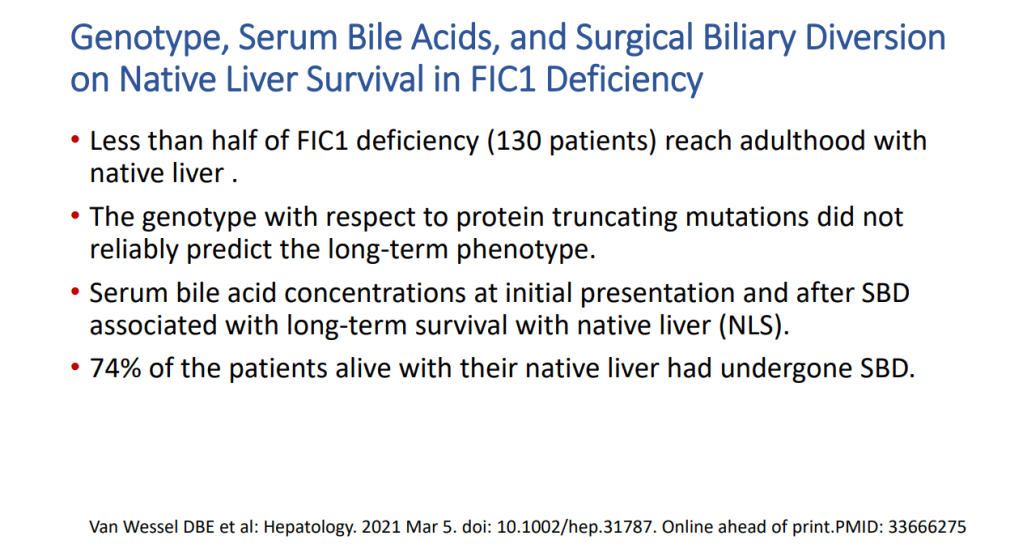
Van Wessel et al (J Hepatol 2020; 73: 84-93) correlated survival with PFIC1/PFIC2 with bile acid levels and showed improvement in survival in those with surgical biliary diversion
Goals for IBAT inhibitor trials: improvement in pruritus, bile acids, reduced ALT, hepatic fibrosis, HCC and need for liver transplantation
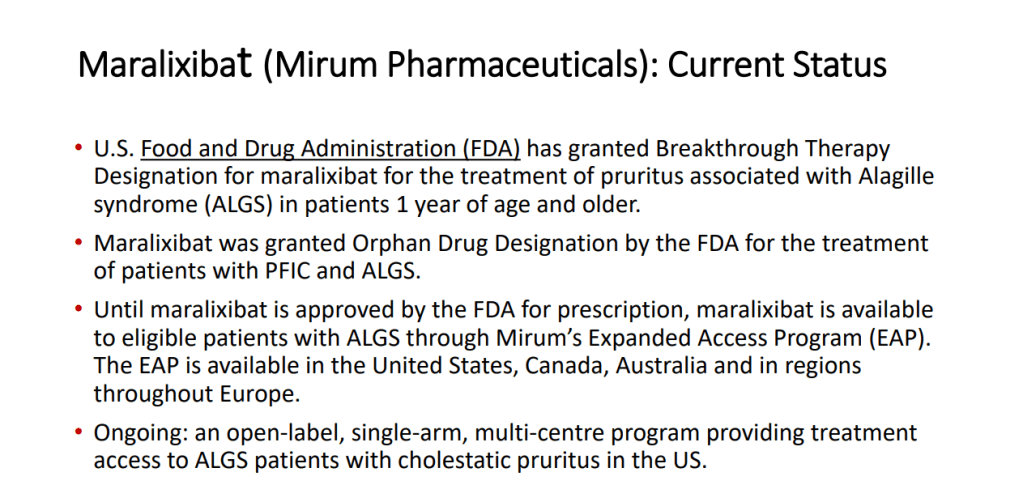
Marixibat is available for use as an FDA approved breakthrough medication for Alagille and PFIC2 in pediatric patients older than 1 year
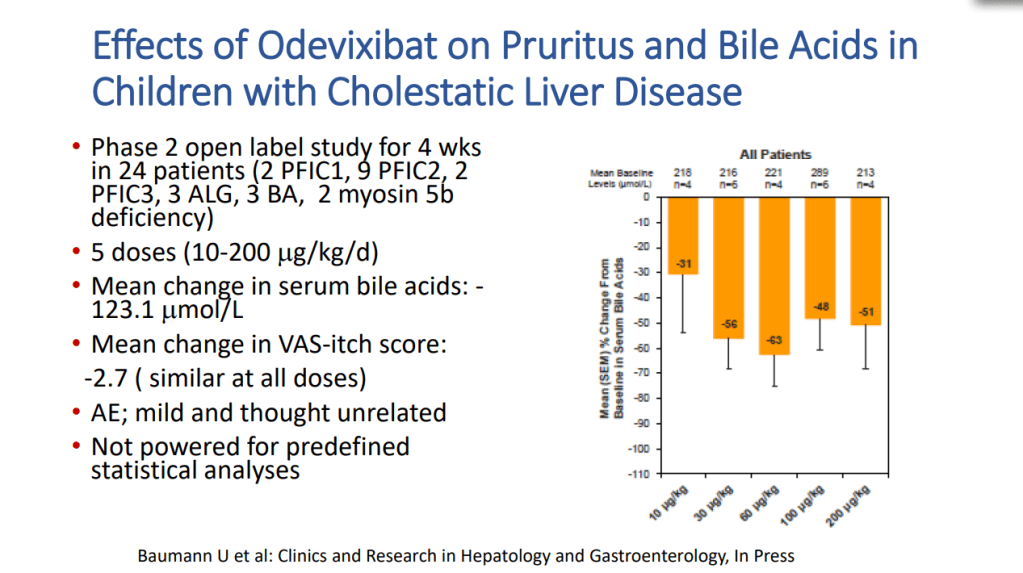
Odexibat is designated as an orphan drug for Alagille, PFIC, PBC, and biliary atresia
Safety appears good with IBAT inhibitors. Fat soluble vitamin monitoring is needed
Case report: Alejandro Velez Lopez
3 yo presented with fatigue and jaundice, 3 weeks after COVID-19 infection. She was not taking any medications. Labs: ALT 939, AST 1321, T bili 5.5, D bili 0.9, INR 2, Plts 174, Hgb 12.8, LDH 1297. remained positive for SARS-CoV2 by PCR. Acetaminophen -no exposure. Evaluation: LKM 1:1280. Neg ANA, NL Ferritin, NL sIL2r, Other viral studies negative, NL IgG. Developed encephalopathy with NH4 317, INR peaked at 2.8. Treated with steroids, rifaximin and lactulose. Liver biopsy showed sub-massive necrosis and fibrosis (indicative of autoimmune hepatitis, likely triggered or exacerbated by COVID-19). Patient responded to medical therapy and did not require liver transplantation.
This blog entry has abbreviated/summarized this presentation. Though not intentional, some important material is likely to have been omitted; in addition, transcription errors are possible as well. Another great lecture from Dr. Suchy.
IBAT Inhibitors Frederick Suchy
Key points:
IBAT inhibitors block intestinal absorption of bile acids/disrupt enterohepatic circulation; this leads to augmented bile acid excretion in stools
IBAT inhibitors may reduce liver damage in the setting of cholestasis/accumulation of toxic bile acids
Potential diseases for IBAT inhibitors include Alagille syndrome and PFIC
Van Wessel et al (J Hepatol 2020; 73: 84-93) correlated survival with PFIC1/PFIC2 with bile acid levels and showed improvement in survival in those with surgical biliary diversion
Goals for IBAT inhibitor trials: improvement in pruritus, bile acids, reduced ALT, hepatic fibrosis, HCC and need for liver transplantation
Marixibat is available for use as an FDA approved breakthrough medication for Alagille and PFIC2 in pediatric patients older than 1 year
Odexibat is designated as an orphan drug for Alagille, PFIC, PBC, and biliary atresia
Safety appears good with IBAT inhibitors. Fat soluble vitamin monitoring is needed
3 yo presented with fatigue and jaundice, 3 weeks after COVID-19 infection. She was not taking any medications. Labs: ALT 939, AST 1321, T bili 5.5, D bili 0.9, INR 2, Plts 174, Hgb 12.8, LDH 1297. remained positive for SARS-CoV2 by PCR. Acetaminophen -no exposure. Evaluation: LKM 1:1280. Neg ANA, NL Ferritin, NL sIL2r, Other viral studies negative, NL IgG. Developed encephalopathy with NH4 317, INR peaked at 2.8. Treated with steroids, rifaximin and lactulose. Liver biopsy showed sub-massive necrosis and fibrosis (indicative of autoimmune hepatitis, likely triggered or exacerbated by COVID-19). Patient responded to medical therapy and did not require liver transplantation.
From the 2nd lecture of the Aspen Webinar. This blog entry has abbreviated/summarized this presentation. Though not intentional, some important material is likely to have been omitted; in addition, transcription errors are possible as well. This was a terrific lecture!
NASH Update Stavra Xanthakos
Key points:
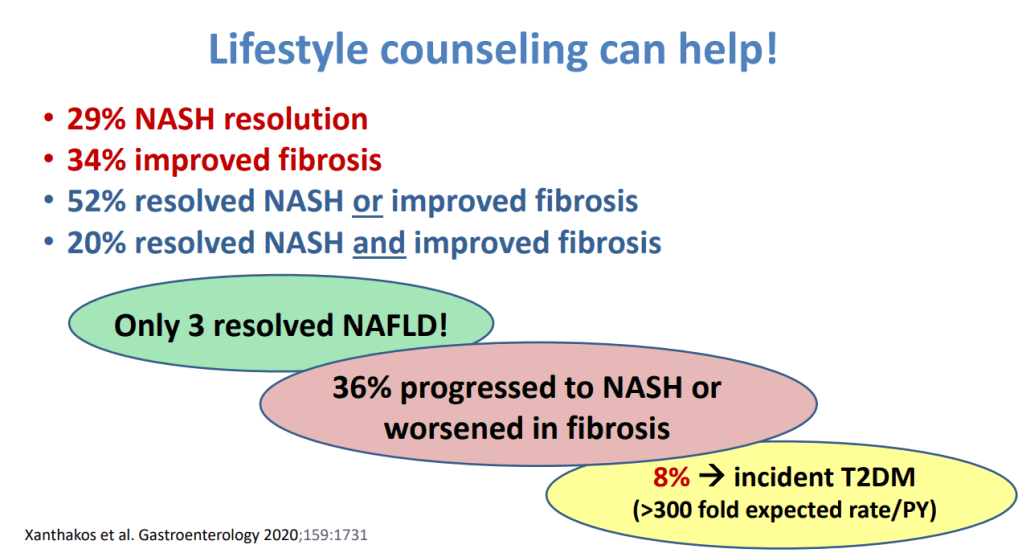
Lifestyle intervention is 1st line Rx (especially avoiding sugary beverages, and processed foods). This may lead to resolution of NASH in ~29%, fibrosis resolution in 34%; though, only 3% resolved fatty liver
Many have progressive disease despite lifestyle treatment recommendations
Consider adjunctive treatments if not improving with lifestyle intervention
Vitamin E for biopsy-confirmed disease (often for 1-2 years of therapy)
Pioglitazone -off-label for adults (18+). Can increase weight; a lot of trials in adults
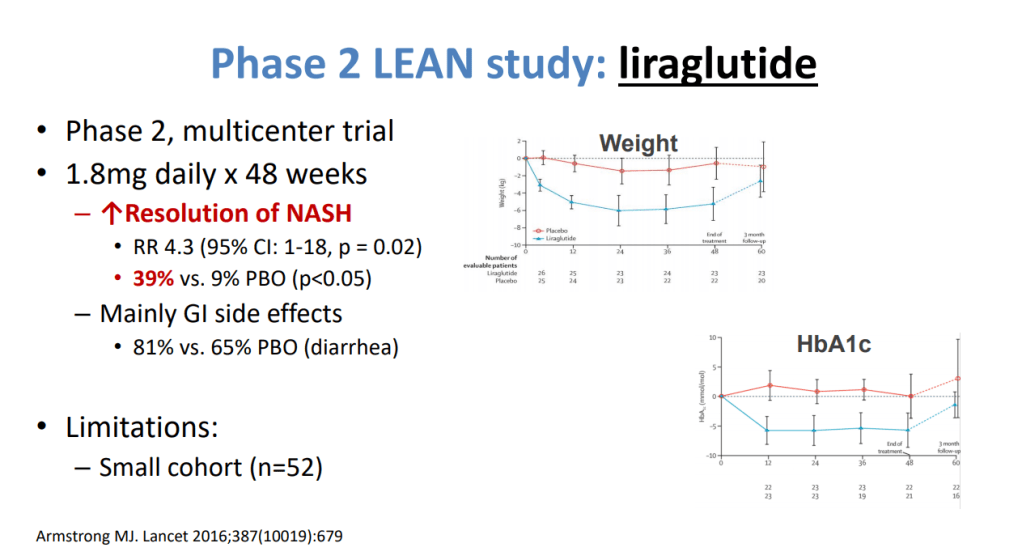
Several phase 3 trials in NASH -GLP1 agonists promising in phase 2 trials
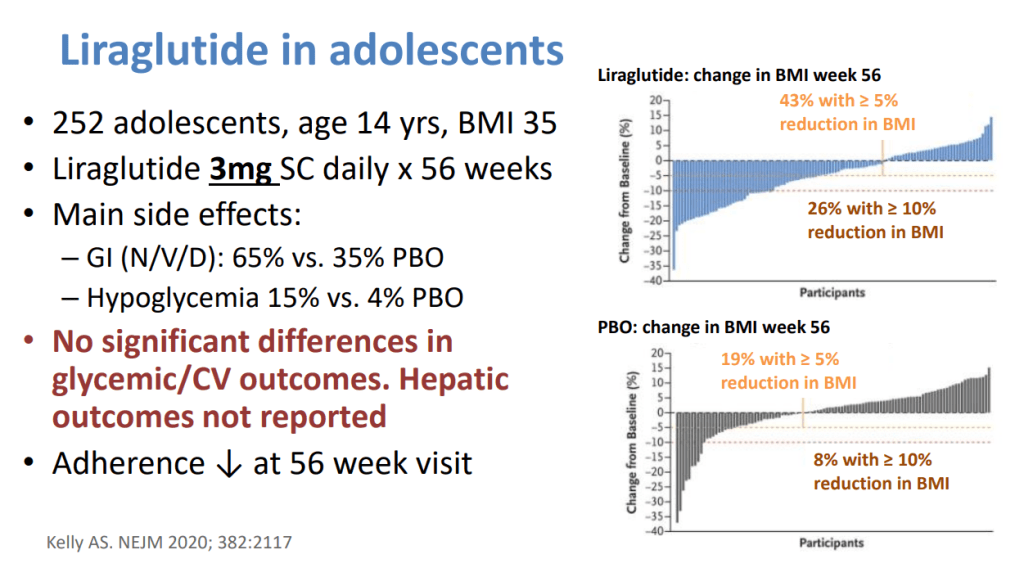
GLP1 agents being used in adolescents with T2DM who may also have NASH – monitor liver outcomes
Anti-obesity medications may help with weight and perhaps the liver. Approved agents for adolescents include 1) Orlistat -safe, but frequent side effects (eg. Diarrhea, greasy accidents) and 2) Liraglutide -daily SC. Insurance coverage is limited.
Biopsy is important before implementing medications and may influence decision to pursue bariatric surgery.
Fibroscan, if shows no significant fibrosis, can help limit biopsy.
Notes from this year’s Aspen Webinar 2021. This blog entry has abbreviated/summarized some of these presentations. Though not intentional, some important material is likely to have been omitted; in addition, transcription errors are possible as well. The first talk was excellent.
What’s Hot -COVID-19 and the Liver William Balistreri
This lecture covered a ton of information and publications with regard to COVID-19 and the liver.
Key points:
Numerous studies generally show that liver problems related to COVID-19 are mild, particularly in children
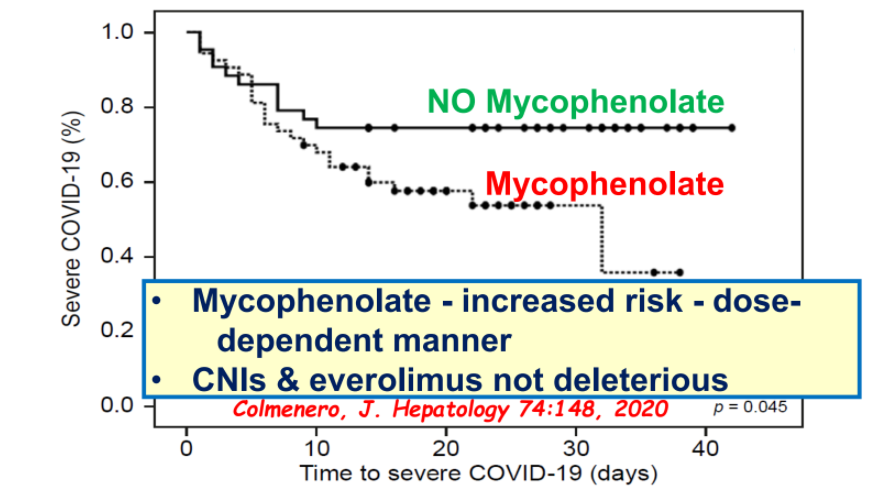
Most immunosuppression agents do not worsen outcomes with COVID-19 and should not be reduced in autoimmune hepatitis or liver transplantation; the exception, mycophenolate has been associated with worsened outcomes
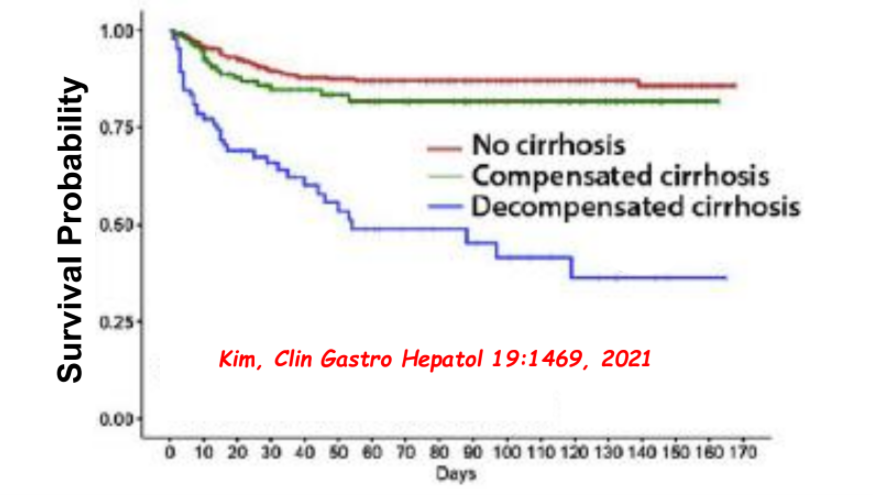
Cirrhosis is associated with worse outcomes in patients with COVID-19
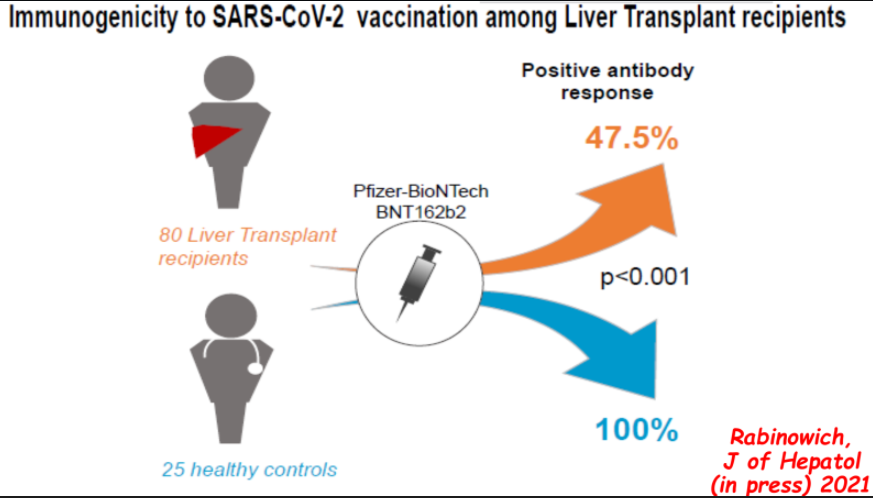
Vaccine response is blunted in immunocompromised patients with 40-50% developing antibody response after two doses of mRNA vaccines and generally lower titers. 3rd dose of vaccine may improve response.
PPI response: 56% for erosive reflux disease, 37% for NERD, and 25% for functional heartburn (FH) per Figure 3 (*”FH might be a placebo effect owing to short follow-up evaluation”
Determination of abnormal acid exposure time (AET >6% in adults) is key in distinguishing NERD from FH which in turn helps with selection of treatment. NERD is notable for AET >6% in adults. Many patients with NERD may also have esophageal hypersensitivity
Table 2 reviews efficacy of neuromodulators for functional esophageal disorders; these include TCAs, SNRIs, SSRIs, and other agents (eg. gabapentin)
Heartburn etiologies in adults, per Yamasak T et al. J Neurogastroenterol Motil 2017; 23: 495-503.
Background: “A high-fat diet has been associated with an increased risk of ulcerative colitis (UC). We studied the effects of a low-fat, high-fiber diet (LFD) vs an improved standard American diet (iSAD, included higher quantities of fruits, vegetables, and fiber than a typical SAD)”
Key findings:
Compared with baseline, the iSAD and LFD each increased quality of life, based on the short IBD questionnaire and Short-Form 36 health survey scores (baseline short IBD questionnaire score, 4.98; iSAD, 5.55; LFD, 5.77; baseline vs iSAD, P = .02; baseline vs LFD, P = .001)
Fecal levels of acetate (an anti-inflammatory metabolite) increased from a relative abundance of 40.37 at baseline to 42.52 on the iSAD and 53.98 on the LFD (baseline vs LFD, P = .05; iSAD vs LFD, P = .09)
Overall, in this small cross-over study (cross-over study) of 17 patients with UC in remission, a catered LFD or a iSAD were each well tolerated and increased quality of life. However, the LFD decreased markers of inflammation and reduced intestinal dysbiosis in fecal samples
My take: While dietary intervention is recognized as a more effective intervention in Crohn’s disease, this study shows that a low-fat high fiber diet for patients with ulcerative colitis may be beneficial.
The four trials (n=255) directly compared the use of normal saline and heparin; the studies all used different protocols for the intervention and control arms, however, and all used different concentrations of heparin.
The estimated RR for CVC occlusion per 1000 catheter days between the normal saline and heparin groups was 0.75 (95% CI 0.10 to 5.51; 2 studies, 229 participants; very low certainty evidence).
The estimated RR for CVC‐associated blood stream infection was 1.48 (95% CI 0.24 to 9.37; 2 studies, 231 participants; low‐certainty evidence).
The duration of catheter placement was reported to be similar for the two study arms in one study (203 participants; moderate‐certainty evidence), and not reported in the remaining studies.
This is in agreement with another updated Cochrane review assessing the effectiveness and safety of intermittent locking of CVCs with heparin vs. normal saline to prevent occlusion in adults (11 studies; N=2,392). The pooled analysis did show fewer occlusions with heparin than with normal saline (RR 0.70, 95% CI 0.51 to 0.95; P = 0.02; 1672 participants; 1025 catheters from 10 studies; I² = 14%), but it is based on a very low-quality of evidence given the differences in methodology, unclear allocation concealment, imprecision, and suspicion of publication bias. (López-Briz E, Ruiz Garcia V, Cabello JB, et al. Heparin versus 0.9% sodium chloride locking for prevention of occlusion in central venous catheters in adults. Cochrane Database Syst Rev. 2018;7(7):CD008462. doi: 10.1002/14651858.CD008462.pub3)
My take: This review found there was not enough evidence to determine which solution, saline or heparin, is more effective for reducing complications.