Adalimumab trough levels (TLs) at both weeks 4 and 8 were significantly higher in remitters vs nonremitters at week 24 (P < 0.001 and P = 0.002, respectively)
The best ADA TL cutoffs at weeks 4 and 8 for predicting clinical/biomarker remission at week 24 were 22.5 µg/mL (80% sensitivity, 90% specificity) and 12.5 µg/mL (94% sensitivity, 60% specificity) respectively
My take (borrowed from authors): Greater early ADA exposure is associated with superior clinical/biomarker outcomes at week 24. ADA pediatric dosing is looking a lot like infliximab dosing in which nearly 75% would be underdosed if using on-label dosing.
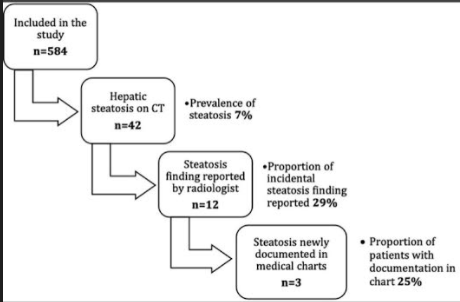
Using absolute liver attenuation <48 Hounsfield units (HU), the prevalence was 7% (n = 42/584). Steatosis was reported for only 12 of 42 (28%) of these patients and was documented in clinical notes in only 3 of those cases
232 (40%) had liver enzymes available within 24 hrs of CT scan. 79 had elevated ALT values; steatosis accounted for only 22% of those with elevated ALT values
In those with liver attenuation < 48 HU, nearly all had abnormal ALT values and the median was 52 U/L
Patients with steatosis had an 8-fold likelihood of overweight/obesity
Discussion:
These findings are similar to an adult study of 1290 patients in which 26% had steatosis but only 5% had those findings identified and documented beyond the radiology report. (N Kutaiba et al. J Med Imaging Radiat Oncol 2019; 3: 431-8)
CT findings are considered much more accurate than ultrasonography.
The authors argue that identification of NAFLD is “crucial” to allow for further specialty evaluation and to exclude secondary causes of steatosis.
My take: This study shows that there is an opportunity to improve identification of incidental steatosis. If identified, this can/should be addressed by their primary care team to emphasize improved diet choices and physical activity.
The abstract, in my view, makes a mistake by emphasizing that NG fed infants (n=35) had less hospital readmissions and ED encounters than G-tube fed infants (n=65). This is problematic because infants who received G-tubes were much sicker than NG fed infants (see Table 1). Compared to NG patients, G-tube patients were more premature (32% 22-28 weeks vs 20% for NG), lower birthweight (2510 g vs 1664 g), more chromosomal anomalies (suspected & confirmed 38% vs. 23%), more likely to have abnormal brain imaging (32% vs 20%), and more likely to have a tracheostomy (34% vs. 0%). In addition, as noted below, the institution reports a very high rate of G-tube dislodgement.
Key points (in my view):
“Our institution uses a a bridle to secure NG tubes just before NICU discharge”
The authors delineate specific criteria for NG discharge: “at least 36 weeks of postmenstrual age (PMA) and weight of 2 kg; 5 days free of apnea or bradycardia requiring nursing intervention after discontinuation of caffeine; 2 days of temperature stability in an open crib; receiving home respiratory support (either room air, or at or below 0.5 liters per minute nasal cannula); at least 25% of feedings by mouth; age-appropriate weight gain; and without anatomic anomalies precluding NG tube placement”
“By 3 months after NICU discharge, 27 of 35 (77%) infants discharged with NG tubes had progressed to full oral feeds; of the remaining 8 infants, 3 received G tubes during the study period, and an additional 3 were scheduled to receive a G tube”
Median duration of NG use was 29 days. The discussion notes that discharge to home may facilitate quicker weaning from NG tubes (SL Williams et al. Tube feeding outcomes of infants in a Level IV NICU.J Perinatol. 2019; 39: 1406-1410)
The authors report a very high rate of G-tube dislodgement, 19 of 65, in a 3-month period. This point is not analyzed by the authors but suggests that the institution utilizes a G-tube prone to dislodgement (eg. secured by a balloon).
My take: This article makes two key points: 1. An NG feeding program can help get infants home sooner and safely (especially with bridle placement) 2. In their institution, G-tubes are dislodged a lot and this leads to frequent returns for medical care; this high rate of dislodgement may indicate a potential benefit to using a different type of G-tube.
Previously the CRISPR gene-editing has been used to counter genetic defects in conditions like sickle cell and thalasemia. This has involved taking cells out of the body, editing them in the lab, and infusing them back in or injecting CRISPR directly into cells that need fixing.
Now, scientists are directly injecting nanoparticles with the CRISPR gene-editing tools. Here’s an excerpt:
Doctors infused billions of microscopic structures known as nanoparticles carrying genetic instructions for the CRISPR gene-editor into four patients in London and two in New Zealand. The nanoparticles were absorbed by their livers, where they unleashed armies of CRISPR gene-editors. The CRISPR editor honed in on the target gene in the liverand sliced it, disabling production of the destructive protein.
“This is really opening a new era as we think about gene-editing where we can begin to think about accessing all kinds of different tissue in the body via systemic administration“
My take: This type of discovery could dramatically improve the treatment of many diseases including heart disease, muscular dystrophy and brain diseases such as Alzheimer’s.
Case report of a 10 month old who developed a small bowel obstruction due to an “Orbeez” ball. “Orbeez balls are small polymer beads that absorbs water and expands, it can get up to 150 times their original size. When left out of water, the beads shrink back down to its original size. They were originally invented as a way to keep moisture in soil for plants. They are hugely popular with children and often used as toys, flower holders, air fresheners, light jars, and objets d’art in the house.”
Methods: A retrospective cohort study was performed on patients (n=518) ages 0 to 21 hospitalized at Johns Hopkins Hospital between 1983 and 2010 with an ICD-9 discharge diagnosis of ascites
Key findings:
Among the 3 age groups (0–5, 6–12, and 13–21), the 0 to 5 age group experienced significantly increased length of stay (LOS) (P < 0.001) and mortality (P = 0.027).
Ascites etiology of veno-occlusive disease (VOD) and the presence of hydrothorax or thrombocytopenia was also significantly associated with increased LOS.
Ascites with the etiology of congestive hepatopathy and the presence of grade 3 ascites, hepatic encephalopathy, hepatorenal syndrome, hydrothorax, hyponatremia, and thrombocytopenia were associated with increased mortality.
Black pediatric patients with ascites have an increased risk of mortality
Zack Cooper, an economist at Yale School of Public Health, and his colleague, Martin Gaynor, have crunched the numbers on hospitals using the government’s preferred way of measuring market concentration, and they’ve found that about 80% of America’s hospital markets are now “highly concentrated.”…
The research clearly shows, Cooper says, that growing monopolization has raised prices for patients. Less competition means hospitals can charge higher prices and get away with it. They can pay lower wages and get away with it. And they can provide worse care and get away with it. “We want firms to compete and be incentivized to raise their quality to attract more consumers, and the more that hospitals merge, the less sharp those incentives become,” Cooper says. “We have evidence that death rates are literally higher in markets where hospitals face less competition.”…
The bizarre part of all this is that many of these monopolizing hospitals are technically considered “nonprofits.” … instead of making profits that are distributed to shareholders, nonprofit hospitals take the extra money they make and use it for executive compensation and buying shiny stuff.
Using a selected sample from a database with >62 million patients, this retrospective cohort study determined the rates of colorectal cancer among patients with IBD. Key finding:
Among the IBD cohort, patients treated with anti-TNF agents were less likely to develop CRC; patients with Crohn’s disease: odds ratio, 0.69; 95% confidence interval, 0.66-0.73; P < 0.0001 vs patients with ulcerative colitis: odds ratio, 0.78; 95% confidence interval, 0.73-0.83; P < 0.0001.
My take: This study found an association between anti-TNF therapy and a reduced risk of CRC in patients with IBD.
Using the National Health Interview survey (2015), the authors identified individuals with self-reported IBD and assessed national estimates of financial toxicity. Key findings:
23% reported financial hardships due to medical bills, 16% of patients reported cost-related medication nonadherence, and 31% reported cost-reducing behaviors
Approximately 62% of patients reported personal and/or health-related financial distress, and 10% of patients deemed health care unaffordable
Inflammatory bowel disease was associated with 1.6 to 2.6 times higher odds of financial toxicity across domains compared with patients without IBD
My take: In addition to the physical and emotional toll of having IBD, there is also significant financial hardships for many.
Methods: Data from 6 ustekinumab phase 2/3 CD and UC studies were pooled, and safety was evaluated through 1 year; this included 2574 patients (1733 patient-years of follow-up)
Key Safety findings –Events per 100 patient years -placebo vs ustekinumab respectively:
Major cardiovascular events were rare with 2 in placebo group 0.34 and 2 in the ustekinumab group 0.12
Morekey findings:
No cases of progressive multifocal leukoencephalopathy or reversible posterior leukoencephalopathy
Antibodies to ustekinumab were identified in 3.6% of patients
My take: This study showed similar safety between ustekinumab and placebo, but is limited by short followup. The authors note that 5-year data from ustekinumab’s use with psoriasis has found no safety signals for malignancy.
This cross-sectional study with 229 patients examined the relationship between inflammatory bowel disease (IBD) activity and resilience based on the Connor-Davidson Resilience Scale questionnaire (high resilience score ≥ 35).
Key findings:
High resilience was noted in 27% of patients with UC and 21.5% of patients with CD.
Among patients with UC, those with high resilience had a mean Mayo score of 1.54, and those with low resilience had a mean Mayo score of 4.31, P < 0.001.
Among patients with CD, those with high resilience had a mean HBI of 2.31, and those with low resilience had a mean HBI of 3.95, P = 0.035.
In multivariable analysis, high resilience was independently associated with lower disease activity in both UC (P < 0.001) and CD (P = 0.037) and with higher QoL (P = 0.016).
High resilience was also associated with fewer surgeries (P = 0.001) among patients with CD.
Reading this study, made me think of Galen’s assertion about a different treatment, circa 100 AD: “All who drink of this remedy recover in a short time except those whom it does not help, who all die. It is obvious, therefore, that it fails only in incurable cases.” In the case of this study, the remedy is resiliency.
This study is intriguing and adds to the literature that mental health and IBD may be a two-way street: mental health may affect IBD and IBD activity may affect mental health. However, it is difficult to prove causation in a cross-sectional study. Reverse causation is possible; that is higher disease burden may result in lower resilience.
Also, it is not clear to me that resilience is a particularly modifiable factor. Some may interpret this study in a ‘blame the victim’ mode. I think a lot of individuals would think they are resilient but most do not know until they face a difficult situation. Perhaps, Mike Tyson’s assertion is more apt: “Everyone has a plan until they get punched in the mouth.”
My take: This study does not prove that resilience helps prevent IBD activity, though being resilient is nice if you have it.
Plus one: JR Rosh et al. J Crohns Colitis. 2021 May 26; jjab089. doi: 10.1093/ecco-jcc/jjab089. (EPUB). Ustekinumab in Pediatric Patients with Moderately to Severely Active Crohn’s Disease Pharmacokinetics, Safety, and Efficacy Results from UniStar, a Phase 1 Study This was a “multicentre, 16-week, double-blind induction dose-ranging study (NCT02968108), patients aged 2-<18 years; patients were randomized (1:1) to one of 2 weight range-based intravenous induction doses: 130mg vs 390mg in patients ≥40kg and 3mg/kg vs 9mg/kg in patients <40kg. At week 8, all patients received a single subcutaneous ustekinumab maintenance dose of 90mg in patients ≥40kg or 2mg/kg in patients <40kg..” (Kudos to my partner, Stanley Cohen, one of the authors)
Key finding: Pharmacokinetics were similar to those in adults with Crohn’s disease. However, serum ustekinumab concentrations were lower among those with body weight <40kg…These results suggest a different dosing regimen may be required for patients <40kg