RW Himes et al. J Pediatr 2021; 230: 55-61. Gastrointestinal Hemorrhage: A Manifestation of the Telomere Biology Disorders
Background: Telomere biology disorders are a complex set of illnesses defined by the presence of very short telomeres; these individuals are at very high risk of bone marrow failure, cancer, and pulmonary fibrosis. There are 15 known genes which can experience damaging mutations, or other abnormalities, that can cause very short telomeres (for example the telomerase genes TERC and TERT). The most widely recognized telomere biology disorder is known as dyskeratosis congenita (DC); others include Hoyeraal-Hreidarsson syndrome, Revesz syndrome, and Coats plus.
Key findings:
- Sixteen patients who experienced GI hemorrhage were identified at 11 centers. Ten patients had a history of hematopoietic cell transplantation.
- Initial GI bleeding occurred at a median of 12.5 years.
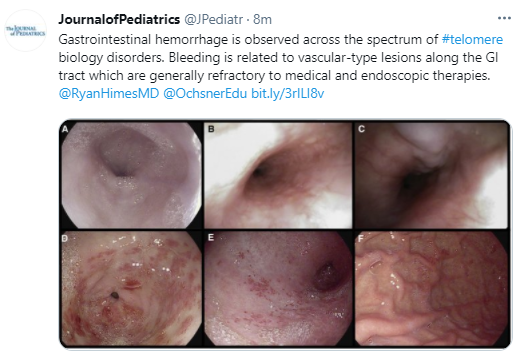
- Angiodysplasia of the stomach and/or small bowel was described in 8 of the 12 patients who underwent endoscopy; 4 had esophageal varices. The lesions were often diffuse and widespread (see Figures 1 & 2).
- GI bleeding appeared to be more prevalent in those with TINF2, CTC1 or STN1 mutations (12 of 14 with genetic testing).
- Recurrence was common, and the overall long-term outcome for affected patients was poor. 12 of 16 were deceased at time of data collection (median age of 16.5 years at time of death), though the proximate cause of death was not reported.
- No single intervention was uniformly associated with cessation of bleeding, although 1 patient had a sustained response to treatment with bevacizumab. Other treatments that were tried included endoscopic treatments, thalidomide, octreotide, proton pump inhibitors, sirolimus and hormonal treatments.
My take: GI bleeding in these rare disorders is a difficult clinical problem.
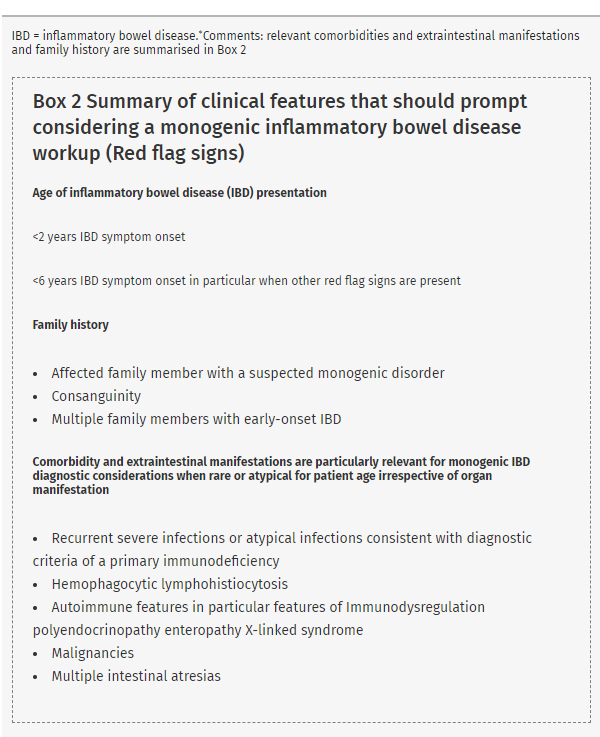
Related blog post: Patterns and Puzzles with Very Early Onset IBD