This was a population-based prospective study from Canterbury, New Zealand
Key findings:
Overall incidence rates were 1.93 per 100,000 for AIH (95% CI, 1.58–2.34), 0.51 per 100,000 for PBC (95% CI, 0.33–0.73), and 0.92 per 100,000 for PSC (95% CI, 0.68–1.21).
The incidence rateof AIH was significantly higher during the period of 2014–2016 (2.39 per 100,000; 95% CI, 1.76–3.23) than during the period of 2008–2010 (1.37 per 100,000; 95% CI, 0.91– 2.06) (P < .05). Incidences of PBC and PSC did not change significantly.
In 2016, prevalence values were 27.4 per 100,000 for AIH (95% CI, 23.58–32.0), 9.33 per 100,000 for PBC (95% CI, 7.13–12.05), and 13.17 per 100,000 for PSC (95% CI, 10.56–16.42).
My take: This study indicates that autoimmune hepatitis has been increasing in incidence.
This study was an analysis of data from the Scientific Registry of Transplant Recipients (2002 through 2019).
Key findings:
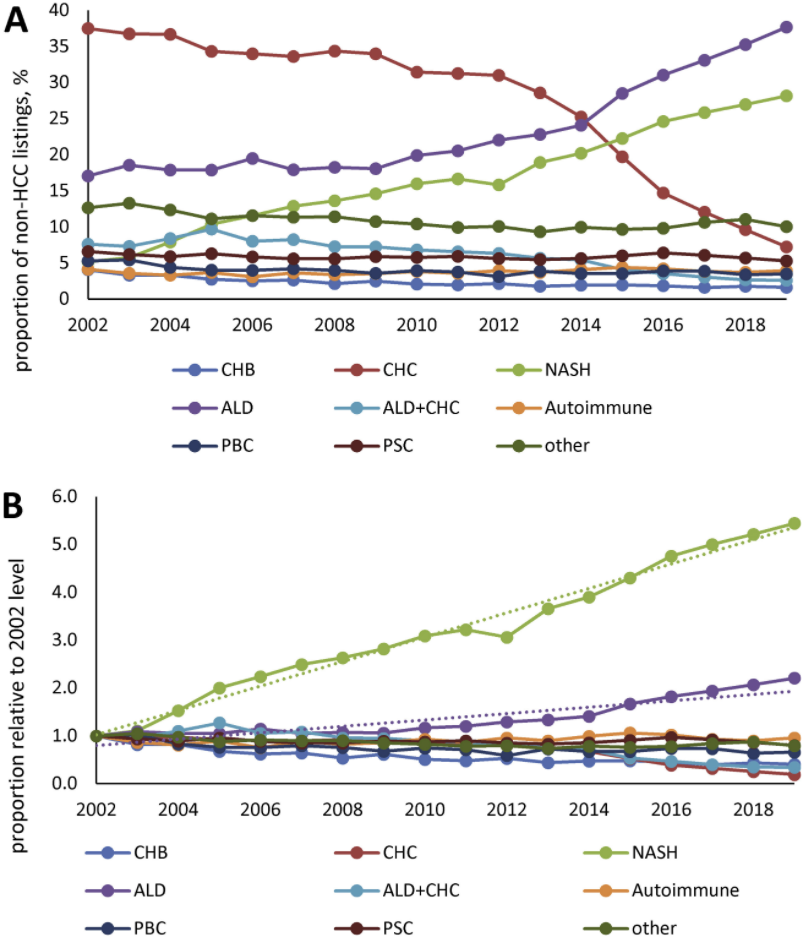
In 2002, the most common etiologies of non-acute liver failure on the liver transplant waitlist (in patients without HCC)
In 2019, among patients without HCC, NASH was the second leading indication for liver transplantation (28% of patients), after ALD (38% of patients). were chronic HCV infection (37%) and ALD (16%), whereas only 5% had NASH
HCC accounted for 27,799 patients (16.5%) and was commonly due to chronic HCV throughout study period
My take: Demand for liver transplantation has NOT improved despite curative therapy for chronic hepatitis C. This is due to increased liver failure related to fatty liver disease and alcoholic liver disease.
Figure 1 Prevalence of the most common CLD etiologies in waitlisted liver transplant candidates without HCC. (A) Proportion of all non-HCC listings with known etiology; (B) the proportion relative to that seen in 2002.
Methods: In a population‐based prospective cohort study of 1,940 infants, we assessed sugar‐containing beverage intake (juice or soda) at 1 year with a validated Food Frequency Questionnaire. Liver fat fraction and NAFLD (liver fat fraction ≥5.0%) were assessed with MR. Key findings:
Compared to infants with <1.0 serving/day, those with >2.0 servings/day had the highest odds of NAFLD at 10 years of age (OR, 3.02; 95% CI, 1.34, 6.83). This was independent of sugar‐containing beverage intake and body mass index at school age
Liver fat fraction greater than or equal to 5% in school-aged children was almost 3-fold higher in those who consumed more than two servings of juice per day at age 1 (4.0%) than in those who drank less than one per day (1.4%)
The associations between juice intake in infancy and NAFLD were strongest in children with overweight or obesity at age 10 and those in families with more limited education
Major strengths of this study are the population‐based prospective longitudinal design with a large sample size, with information on sugar‐containing beverage intake in infancy and liver fat fraction measured with MR at 10 years of age.
My take: Juice and other high sugar beverages (eg soda) should be avoided, particularly at younger ages.
This study analyzed data from 66 patients who completed the 16-week, double-blind, induction portion of a phase 2 study of RPC4046 (180 mg or 360 mg/wk) vs placebo and then completed a 52-week LTE, receiving open-label RPC4046 360 mg/wk. 20 of the 86 initial subjects (from the 16 week induction study) did not complete the full 52-week duration of the open label extension
Key findings:
Overall, 42 of 66 (64%) subjects had a peak eosinophil count <15 at 52 weeks
In the initially-treated group, 29/57 (51%) had peak eosinophil count <15 at 16 weeks
20/29 maintained a eosinophil count <15 at 52 weeks; 3 had an eosinophil count of 15 or greater at 52 weeks. Thus, 20/23 (87%) with data at 52 weeks maintained response.
In the initially-treated group, 28/57 (49%) had a peak eosinophil count of 15 or greater at 16 weeks
10/28 (36%) had a peak eosinophil count <15 at 52 weeks and 12 continued with an eosinophil count of 15 or greater at 52 weeks. Thus, 10/22 (45%) acquired a response after the induction period.
In the placebo induction group (n=29), none had a peak eosinophil count <15 at week 16
12/29 (43%) had a peak eosinophil count <15 at 52 weeks during open-label treatment; 9 continued with an eosinophil count of 15 or greater at 52 weeks. Thus, 12/21 (57%) developed a response without an induction treatment.
In addition to the improvements in eosinophil count, the authors identified clinical, endoscopic, and histologic improvement. “RPC4046 was well tolerated with little immunogenicity elicited in the LTE period.” Overall, the majority of treatment related adverse events were mild or moderate in severity and “no significant safety concerns.”
My take: This study shows that RPC4046 may emerge as a useful treatment for EoE.
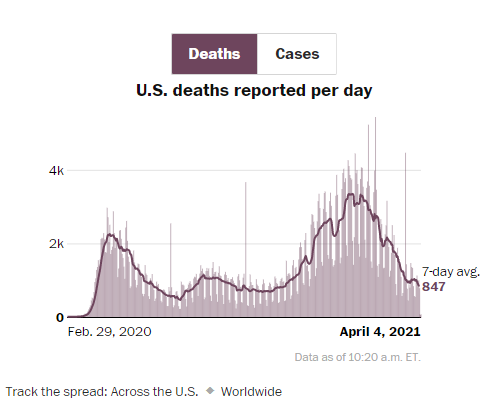
From Washington Post. U.S. Death rate from COVID-19 continues to decline, even though the number of reported daily cases has increased in last 3 weeks. With previous surges, deaths have been a lagging indicator. With the large number of vulnerable individuals vaccinated, it is unclear if the death rate will rise again or will continue to decline.
An excerpt: “The 2021 “Dirty Dozen,” released Wednesday by the Environmental Working Group, ranked pesticide residue levels of fruits and vegetables based on samples taken by the U.S. Department of Agriculture and the U.S. Food and Drug Administration…’The most important thing is that everyone should be eating lots of fruits and vegetables…We do recommend you try to reduce your pesticide exposure.'”
“USDA’s Pesticide Data Program report finds that 99% of samples tested fell below the safety standards set by the Environmental Protection Agency…Only one in 10 Americans eat enough fruits and vegetables daily, according to the Centers for Disease Control and Prevention…Dirty Dozen list creates fear and disparages consumers from buying — organic or not.”
Related article: NY Times, Nicholas Kristof: What are Sperm Telling Us? “Scientists are concerned by falling sperm counts and declining egg quality. Endocrine-disrupting chemicals may be the problem.”
My take: It is concerning that many foods have pesticides. However, adequate fruit and vegetables in the diet offers many health advantages and this is probably a greater priority.
K Gottlieb, J Requa et al. Gastroenterol 2021; 160: 710-719. Central Reading of Ulcerative Colitis Clinical Trial Videos Using Neural NetworksKey finding: A deep learning algorithm can be trained to predict levels of UC severity from full-length endoscopy videos with excellent agreement with human central readers; endoscopic healing accuracy was 97% for UC endoscopic index of severity (UCEIS) and 95.5% for endoscopic Mayo score.
The investigators enrolled 53 adults with celiac disease (CD) for at least two years and followed symptoms as well as stool/urine testing for gluten immunogenic peptide (GIP). “GIP in stool can detect gluten consumption of more than 40 mg/d and the urine tests are positive from 40 and 500 mg/d of gluten.”
Key findings:
Over the 4-week study period, weekend samples (urine) identified 70% of patients excreted GIP at least once, compared with 62% during weekdays (stool).
Patients had a median of 3 exposures during the 4 weeks.
Also, the authors noted increases in GIP excretion towards the end of the study. “This suggests a potential Hawthorne effect that could be explained by a decrease in hypervigilance that often is seen in a context of research studies.”
The authors note that GIP “excretions of greater than 2 mcg/g in stool or greater than 12 ng/mL in urine can induce mucosal damage in almost 100% of patients.”
My take: This study adds to the body of literature emphasizing the high rate of inadvertent gluten exposure.
This is a very useful article with recommendations for central venous access in children. The main recommendations are summarized in Table 3 & listed below; however, there is a lot of detailed information in the article on frequent issues like schools, travel (including dealing with TSA), sports, and even swimming. In addition, the article delineates recommendations for management and prevention of line complications.
1. Recommendations for venous access:
Tunneled, single lumen, cuffed silicone catheters should be used for children with IF.
Upper extremity access is the preferred location when available.
2. Recommendations pertaining to routine CVC care:
Proper technique and hygiene surrounding CVC care are of paramount importance in preventing CVC-associated complications. Caregivers should receive directed education regarding CVC care before initial discharge, with subsequent reinforcement education as needed.
CHG impregnated supplies (disk, sponge, or dressing) should be considered for central line dressing in pediatric IF patients.
Routine surveillance of central venous access should be performed by US. MR, CT, or traditional venography should be reserved for when further delineation of access is required.
3. Recommendations regarding general considerations—sports, travel, and emergencies:
All children with IF should be provided with an emergency letter that details the specific needs of the individual child in case of an emergency. (See at bottom for example -Figure 1)
Discuss with families the risks of swimming and sports participation with strategies to protect the dressing and central line.
All travel plans should be discussed with the intestinal rehabilitation team well in advance of travel to facilitate discussion of a plan of care in case of emergency.
4. Recommendations regarding central line-associated bloodstream infections:
All children with IF and CVC who develop a fever (≥38.0°C) should be admitted to the hospital and assessed for bacteremia with central and peripheral blood cultures while receiving broad-spectrum empiric antibiotics through the CVC for at least 48 h, awaiting culture results regardless of other infectious sources.
If clinically stable, discuss with the patient’s IRP before line removal for CLABSI.
Prophylactic lock therapy with ethanol or other nonantibiotic locks should be strongly considered in all children with IF who have had at least one central line-associated bloodstream infection or are at high risk for infection.
5. Recommendations pertaining to central line mechanical complications:
In children with IF, CVC should be repaired whenever possible to preserve central venous access.
Children with IF and a newly identified CRT should be treated with low molecular weight heparin for at least 6 weeks with guidance from a hematologist.
Children with IF who have persistence of at least one chronic thrombus should be maintained on prophylactic anticoagulation with low molecular weight heparin.
Children who have lost multiple sites of central venous access should be considered for referral to an intestinal transplant center for evaluation and management
6. Recommendations for central venous access program management:
All centers following children with IF should, at a minimum, track the number of outpatient CLABSI per 1000 catheter days.
With regard to swimming: “Swimming introduces an incompletely defined but potentially severe risk to those requiring chronic central venous access. Contamination of various chlorine-treated (swimming pools), stagnant (lakes and ponds), and flowing (oceans and rivers) bodies of water with human pathogens has been well documented, though proper maintenance may minimize outbreaks. The potentially fatal risk of such contaminants gaining access to central circulation via the CVC is unclear…Parents seeking guidance are confronted by mixed messaging from support programs, online resources and blogs, and even IRP. These conflicting recommendations and practices reflect the paucity of data to guide a safe and clear approach for swimming with a central line…[in one study of 16 home PN programs] swimming in low-risk situations [was permitted but] recommended immediate site cleaning and dressing change following water exposure and avoidance of submersion for 4–6 weeks after CVC placement. Ultimately, the decision to permit children with IF to swim lies with the parent or guardian.”
For pets (like Charlie), this article notes that “steps should be taken to promote line integrity in the presence of pets. Particularly in the setting of pets that may attempt to chew or play with tubing, adequate physical protection of the insertion site and catheter itself is recommended. Any line or tubing puncture by an animal should prompt immediate evaluation. Family awareness of zoonotic disease risk and advocacy of handwashing before and after animal care should be made clear.”Figure 1 -Emergency Letter Template
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
This small (n=28) retrospective study provides useful information on the persistence of feeding problems in children with short bowel syndrome (SBS). The authors defined a pediatric feeding disorder (PFD) as “reliance on enteral feeds to sustain nutrition, reliance on high-calorie oral supplements to sustain nutrition, or feeding skill dysfunction resulting in not consuming an age-appropriate diet.” Patients who remained on PN were considered to have a PFD as well.
Key findings:
Of the 21 patients (75% of total cohort) who were weaned off parenteral nutrition, 57.1%, 81.0%, 90.5%, and 100.0% achieved this by 12, 24, 36, and 48 months of age, respectively. Median age at time of weaning PN was 10.8 months.
Of the 13 patients who were weaned off enteral nutrition (EN), 30.8%, 69.2%, 76.9%, and 100.0% achieved this by 12, 24, 36, and 48 months, respectively. Median age of weaning EN was 15.7 months. Overall, about a third of patients required EN beyond 2 years of life.
The prevalence of PFD (of entire cohort) was 100.0%, 76.5%, 68.8%, and 70.0% at 1, 2, 3, and 4 years of age, respectively
My take: When parents ask how long it will be before my child is off PN and eating by mouth, this study’s results could be useful.
In this study, the authors used a state-transition model to assess cost-effectiveness of hepatitis C virus (HCV) infection in children; the model treated a hypothetical cohort of 10,000 children with chronic HCV at age 6 years with combination therapy of sofosbuvir/ledipasvir for 12 weeks vs deferring treatment until 18 years of age.
Key findings:
The incremental cost effectiveness of early treatment of young children was $12 690 per QALY gained after 20 years, which is considered cost effective compared with deferred treatment.
The authors note that if the cost of DAA medications dropped by 60%, then early treatment would not be more cost effective.
However, early treatment of 10,000 children would prevent 330 cases of cirrhosis, 18 cases of hepatocellular carcinoma, and 48 liver-related deaths.
The investigators presented an additional scenario treating children as young as 3 years of age and using alternative treatment with the pan-genotypic combination of glecaprevir/pibrentasvir for 8 weeks; using glecaprevir/pibrentasvir resulted in an incremental cost effectiveness of $12 563 per QALY compared with deferring treatment to age 18 years.
All cost effective models have built in assumptions. This model, for example, presumes each patient is offered treatment only once and does not get reinfected before age 18 years.
Other aspects about early treatment that are difficult to quantitate:
Improved adherence at younger age which improves cost effectiveness
Reduction in transmission of HCV as a consequence of successful treatment
Detrimental effects of untreated/deferred treatment HCV on quality of life, psychosocial health, and cognitive functioning
My take: This study (& editorial) demonstrate that early treatment of HCV is a good value and delivers non-economic benefits as well. Every child (>3 years) with HCV should be treated and cured of HCV infection.