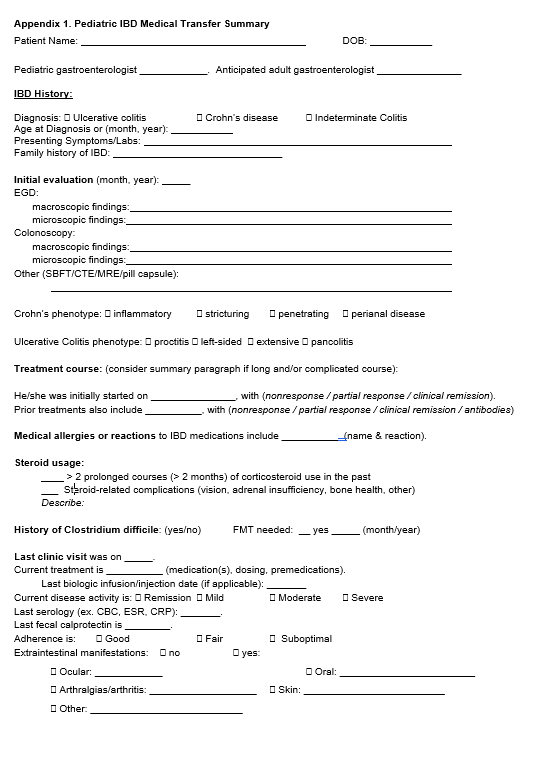
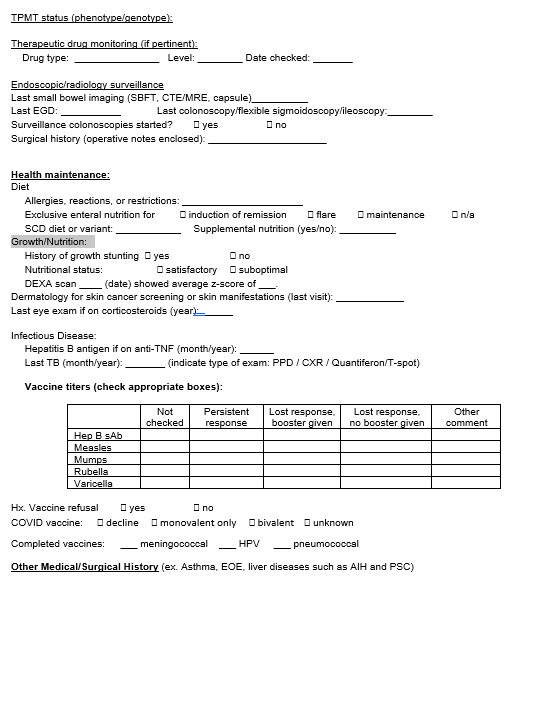
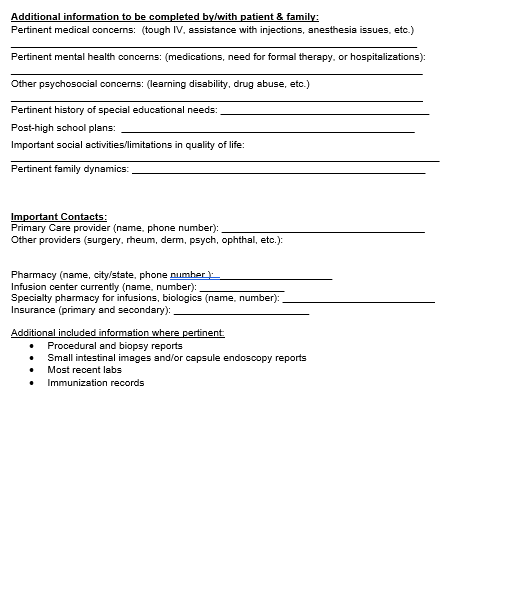
This article describes a “multidisciplinary development and testing of a standardized pediatric IBD medical transfer summary template (PIBD-MTS) as a tool to improve the handoff of patient care.”
The “succinct nature allows AGIs [adult GIs] to review information within 10 min, in contrast to typically sifting through copious disorganized notes that may be redundant, at times irrelevant or missing key information. Its comprehensive nature includes prompts for disease monitoring, health maintenance, nutrition as well as mental health and socioeconomic factors that may affect IBD care.”
My take: This is a good template for transitioning patients. Though the focus is on transfers to adult gastroenterologists as patients get older, this form would be applicable for many patients who see other pediatric gastroenterologists for location or second opinions. It would be a good idea for this form to be available on the ImproveCareNow website. (It may be there but I did not see it). In addition, many centers may want to incorporate this template into their EMRs (eg. EPIC letter).
This genome-wide association study (GWAS) confirms the idiopathic achalasia (IA) “association of variants in HLA-DQB1 and HLA-DQA1, but also points to a more complex genetic risk architecture at this locus that involves an IA risk variant in HLA-DRB1. Moreover, the GWAS resulted in the identification of three novel disease variants outside HLA. One leads to an amino acid substitution with functional effect in PTPN22. One further novel IA risk variant leads to a downregulated expression of TNFSF8, TNFSF15 and TNC in immune-relevant cells. The remaining disease variant is located near ZNF365, but the cellular pathogenic mechanism remains unknown.”
“On the polygenic level, this study provides the first IA heritability estimate and shows that immune-mediated mechanisms that are shared with Crohn’s disease (CD) contribute to IA aetiopathology.”
My take: This study “highlights that immune-mediated mechanisms influenced by genetic risk are of major relevance for disease development.”
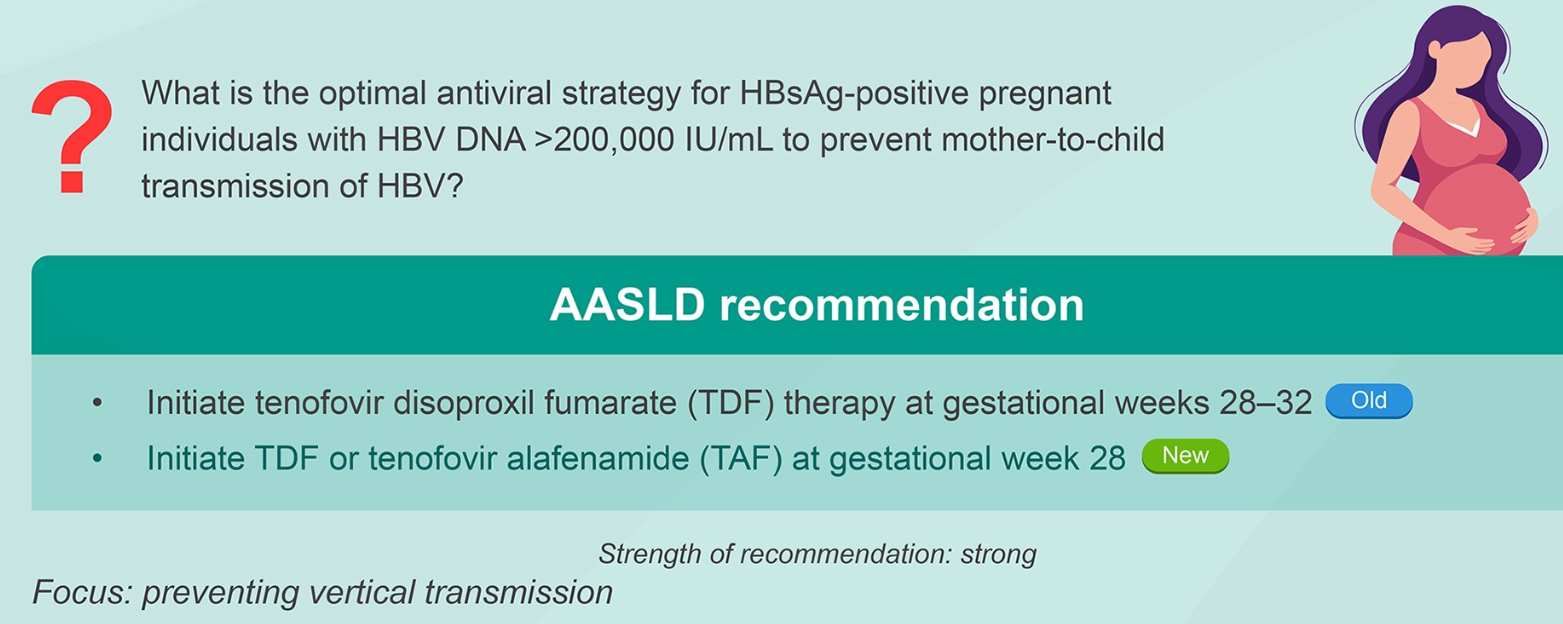
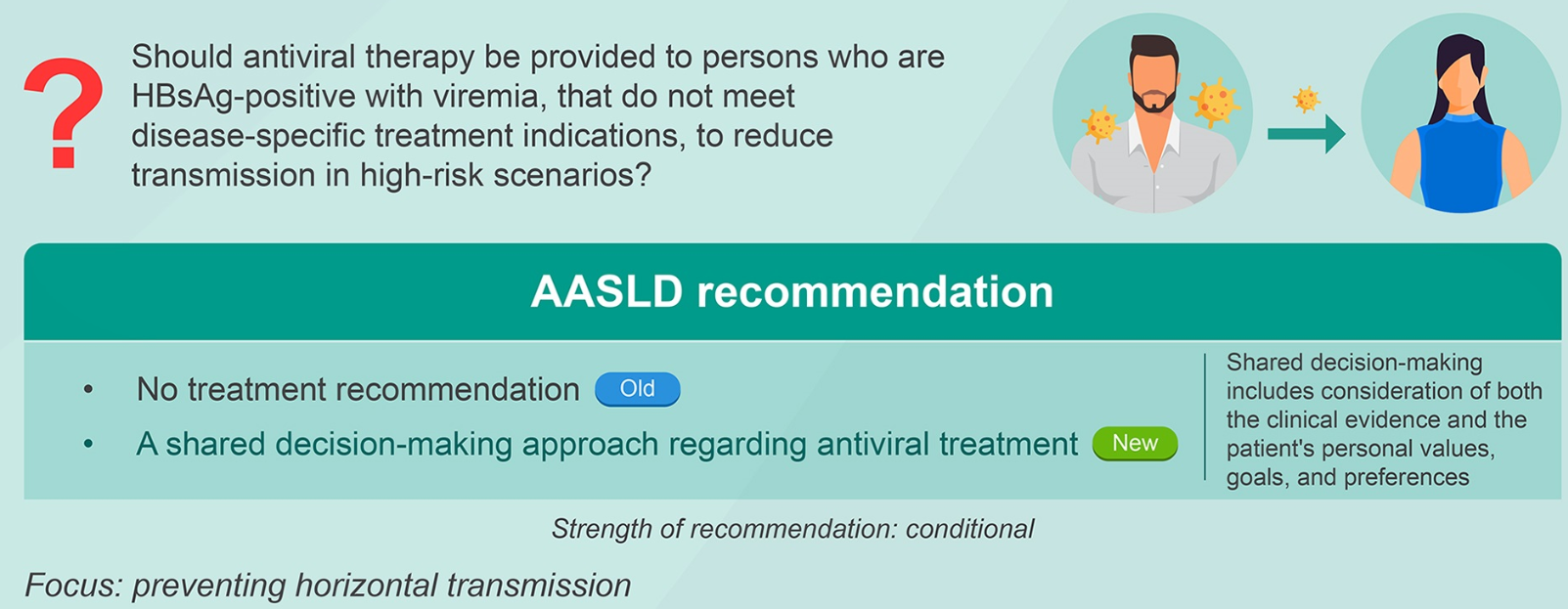
Yesterdays’ blog post summarized the 6 key questions that are reviewed in the updated guidelines. Today’s post provides more details on treatment and a direct link to the practice guideline.
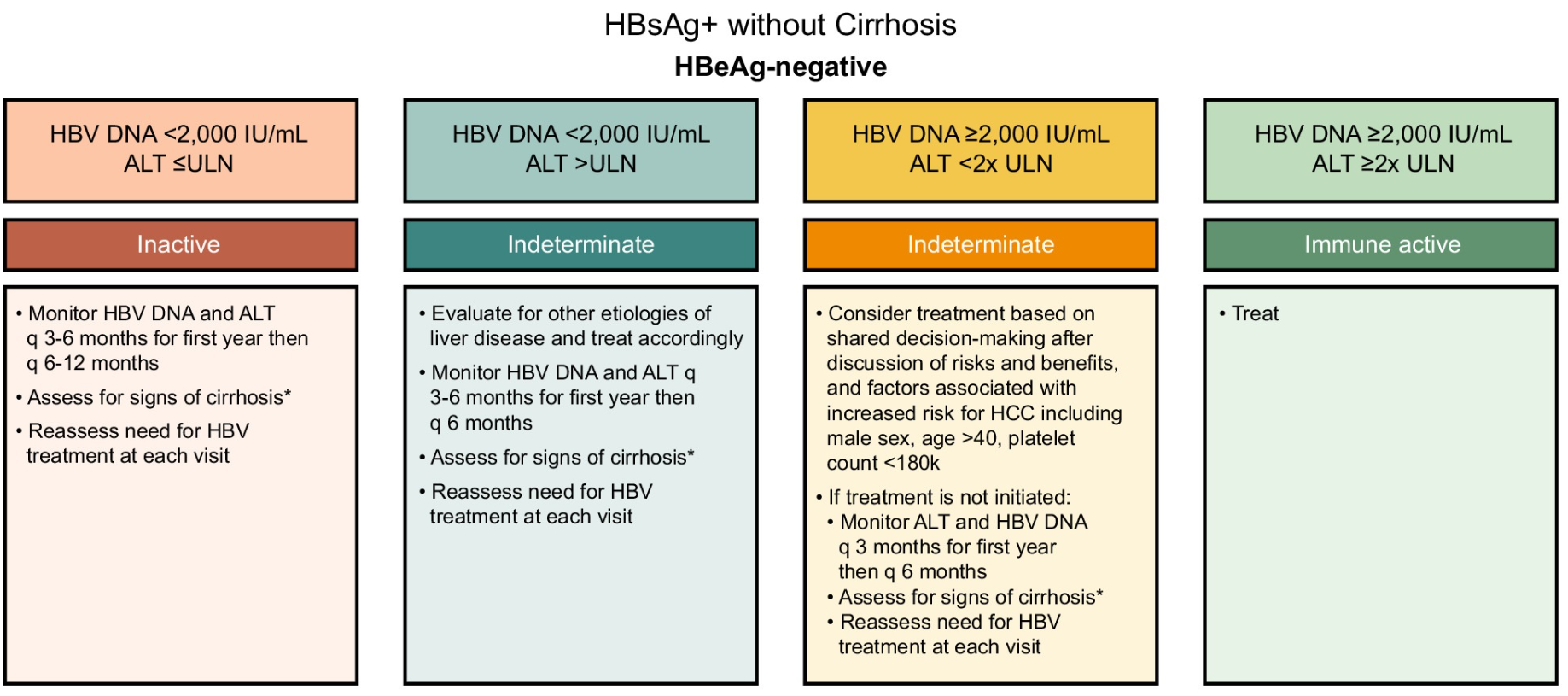
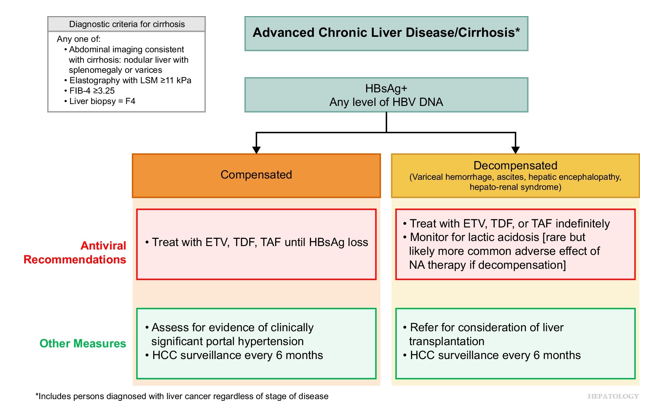
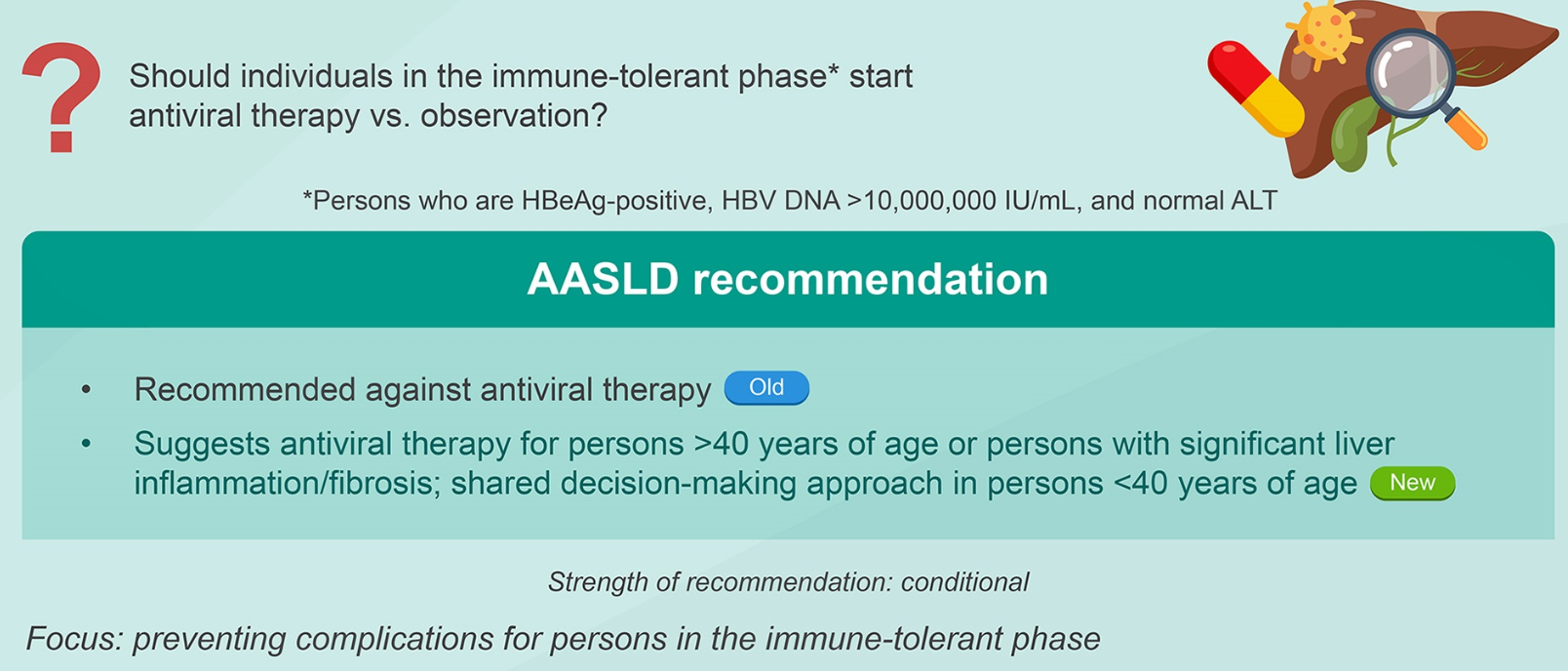
Background: “CHB affects ~258 million individuals (2022) globally8 and leads to an estimated 1.1 million deaths annually due to complications of cirrhosis and HCC…This guideline focuses on six specific issues related to management of CHB. Other recommendations for management of CHB addressed in the 2018 guidelines will continue to be applicable and the reader is referred to this document.1“
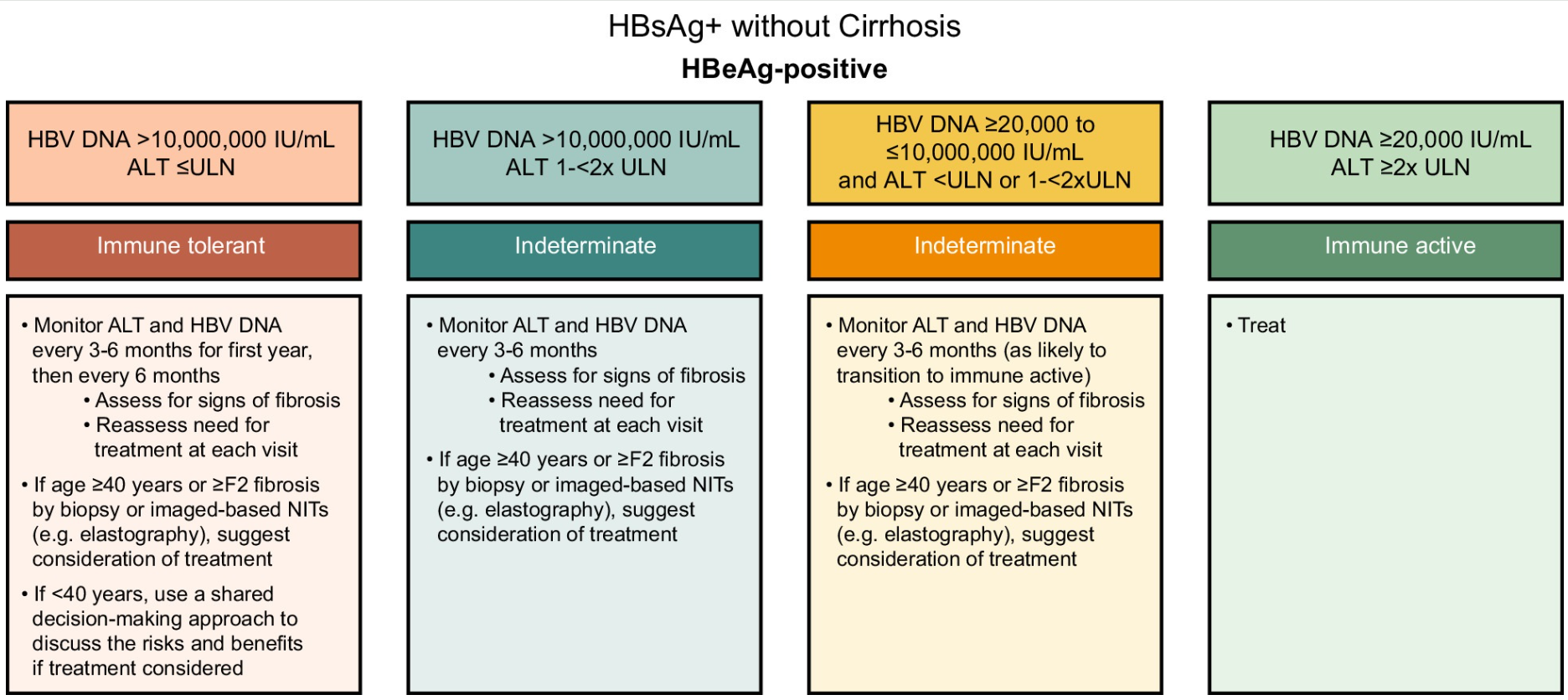
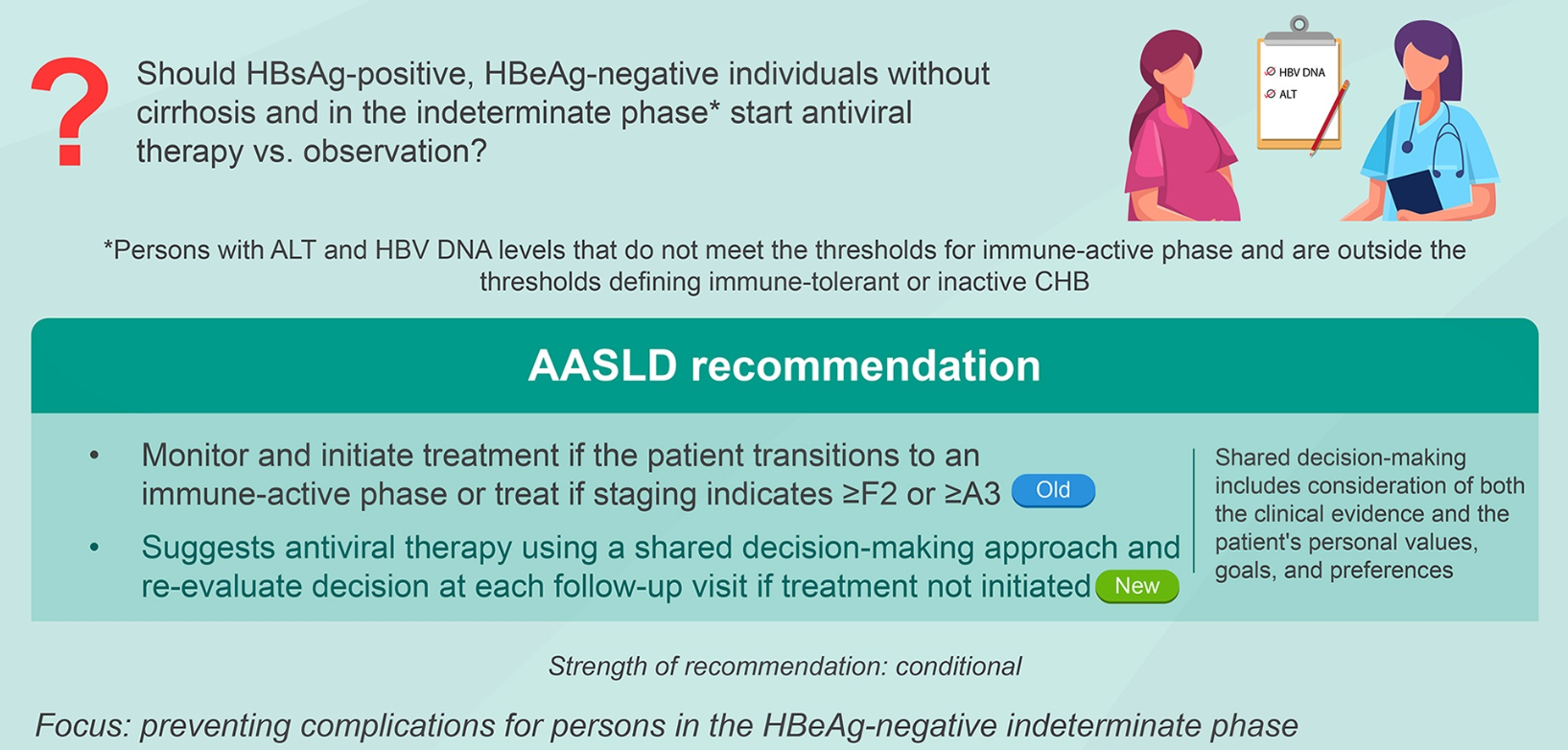
Treatment Recommendations for Patients without Cirrhosis Based on HBeAg Results, HBV DNA and ALT Values
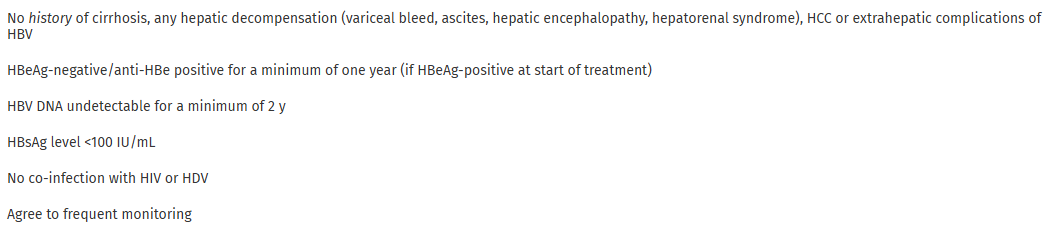
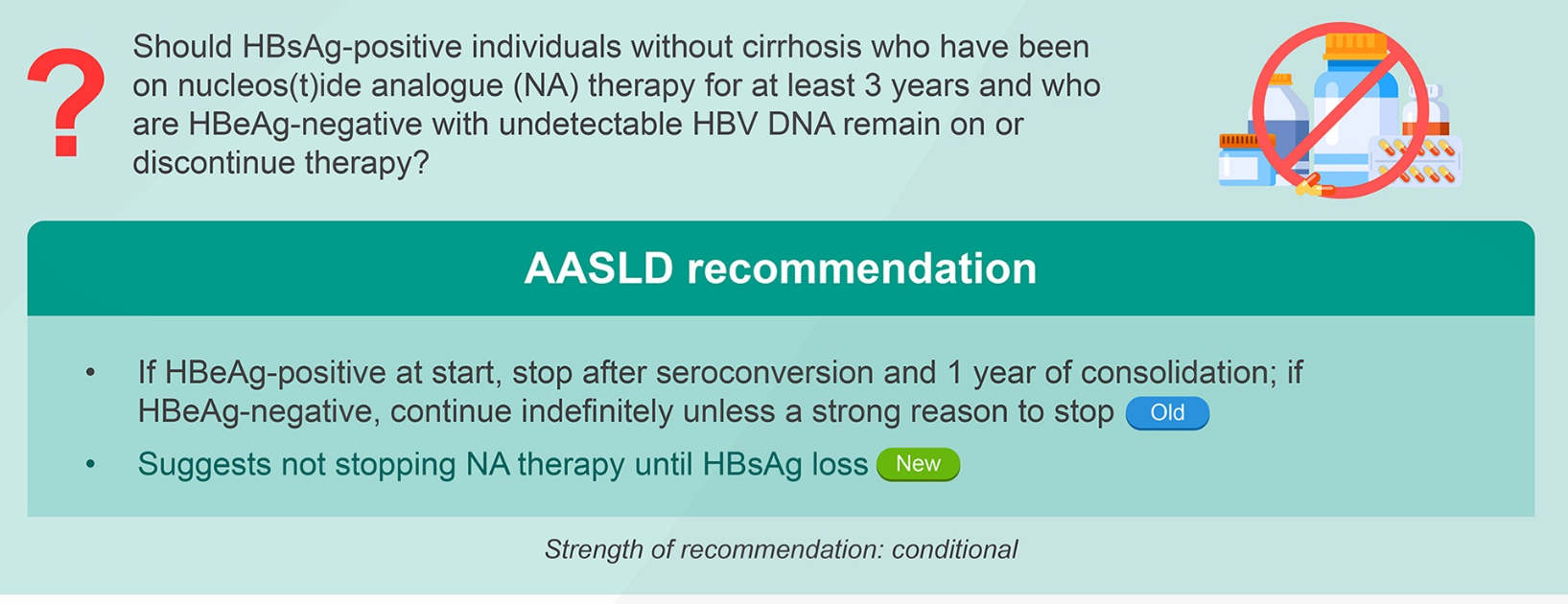
AASLD guidelines favor continuing nucleos(t)ide analogs (NAs) therapy until loss of HBsAg. However, there are additional criteria in new the guidelines for shared decision-making on stopping therapy in those with very low HBsAg levels (<100 IU/mL).
Criteria for stopping NA therapy if ALL are met:
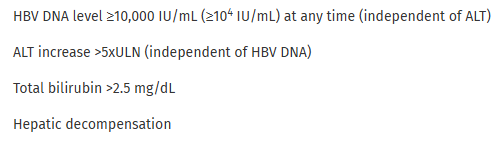
Criteria for resuming therapy immediately (need only 1)
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
This commentary/review makes a number of useful points:
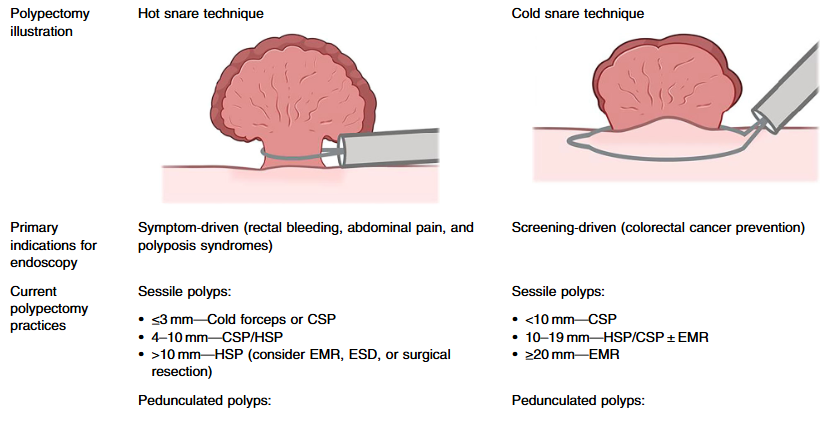
In adults, there have been important changes in recommendations. Guidelines recommend “cold snare polypectomy (CSP) for small and diminutive polyps (<10 mm) due to its favorable safety profile compared to electrocautery techniques.2”
“The European Society for Paediatric Gastroenterology, Hepatology, and Nutrition provides position papers for polyposis syndromes from 2019, including familial adenomatous polyposis (FAP), Peutz–Jeghers syndrome (PJS), and juvenile polyposis syndrome (JPS), which also provide guidance on polypectomy practices.8–10“
“No studies have directly compared the safety and efficacy of various polypectomy techniques—such as cold forceps, hot forceps, cold snare, and hot snare methods—in children. As a result, pediatric practices often rely on extrapolated adult data, despite key differences in patient populations.”
My take (borrowed from authors): “Polypectomy is central to pediatric endoscopy, yet evidence-based, pediatric-specific guidelines are lacking.”
Related article: Hoskins BJ, Grabau JM, Rex DK. J Pediatr Gastroenterol Nutr. 2025;81:1311-131. Pediatric endoscopic mucosal resection: a 10-year single-center experience. . https://doi.org/10.1002/jpn3.70194
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition
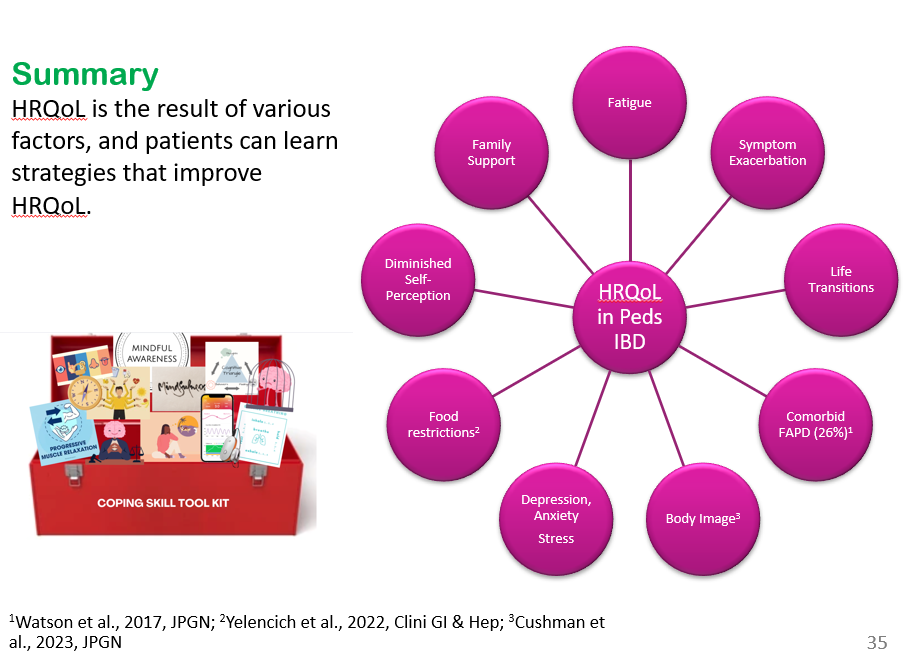
We had a terrific lecture given to our group by Dr. Bonney Reed. She is a pediatric psychologist with a clinical and research focus on children with inflammatory bowel disease. Our group has worked closely with Dr. Reed for many years. Many of her slides are included below along with my notes; my notes may contain errors in transcription and in omission.
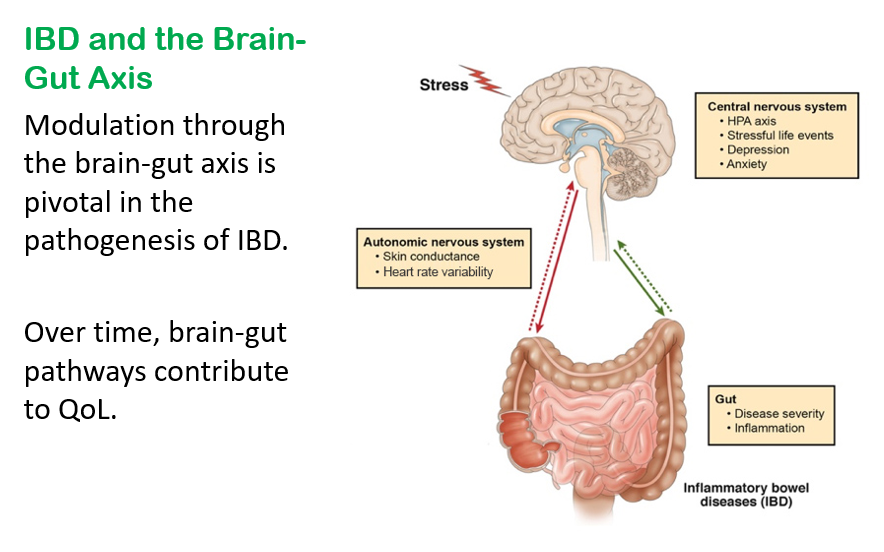
GI symptoms may begin as the result of organic disease (e.g., IBD). Anxiety and chronic activation of the stress response system may lead to alterations in the brain, spinal cord, and gut increasing the load of GI symptoms. In turn, distress associated with GI symptoms may contribute to anxiety or depressed mood, creating a cycle of worsening GI symptoms and overall psychological distress.
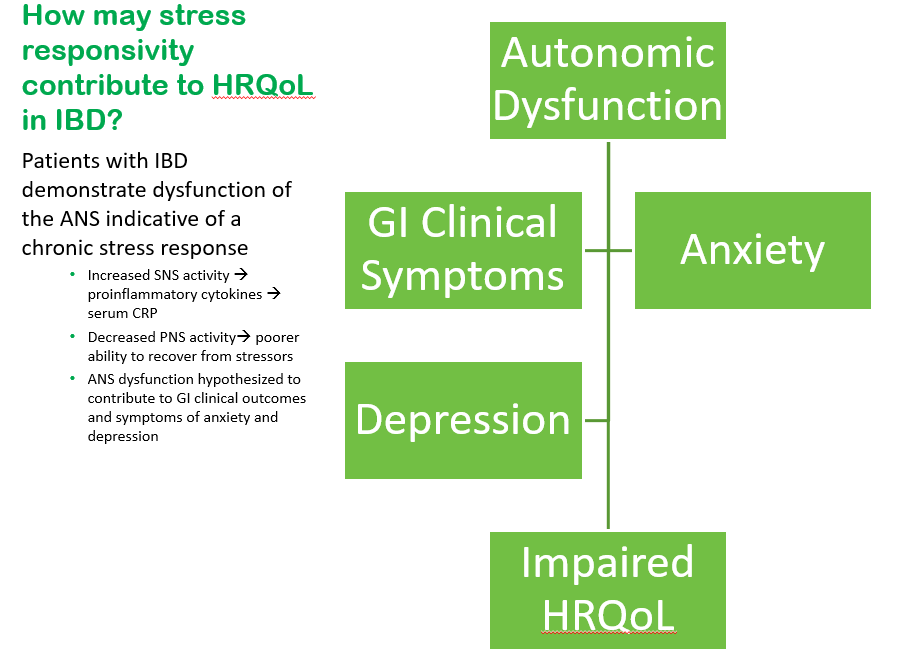
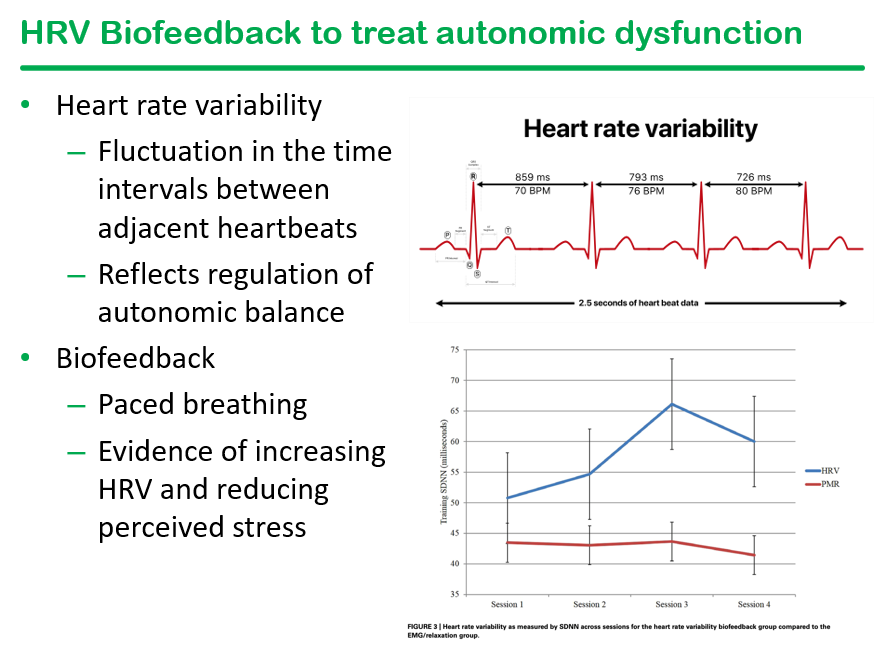
Consistent with a brain-gut axis model, individuals with IBD, compared to healthy controls, demonstrate dysfunction of the ANS indicative of a chronic stress response which is characterized by increased sympathetic nervous system (SNS) activity and reduced parasympathetic nervous system (PNS) activity
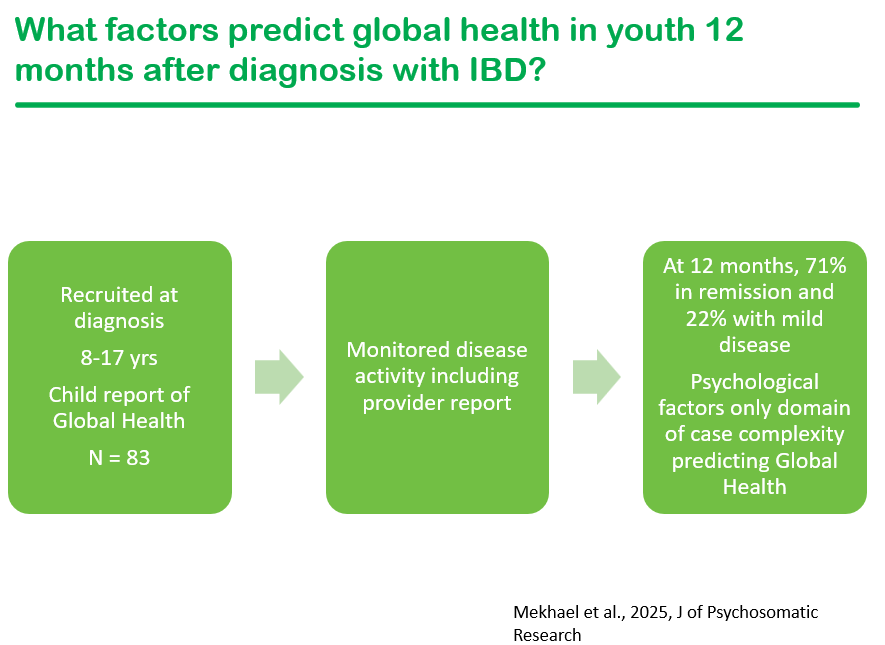
Psychological factors are the key factor for pediatric patients with IBD when self-rating their global health
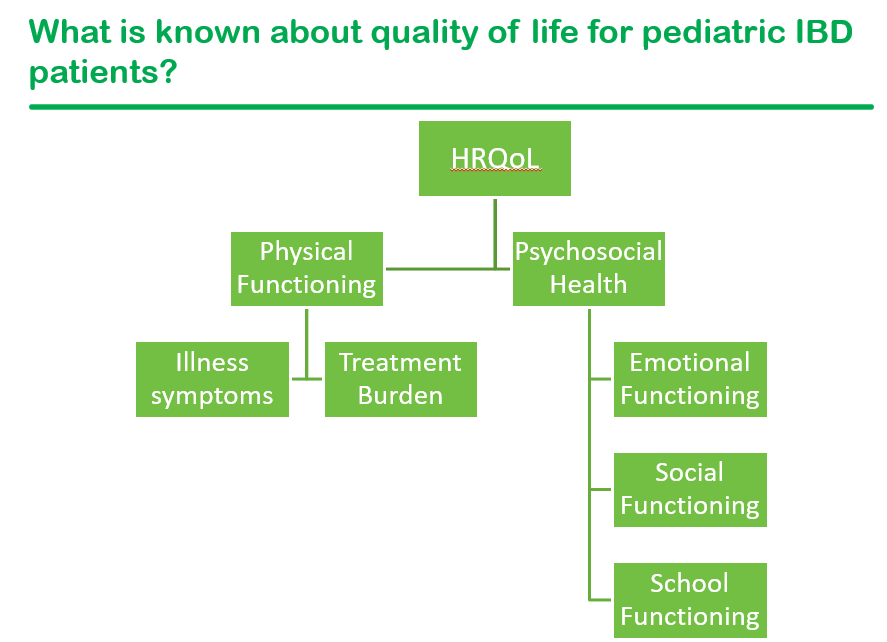
Factors that contribute to an individual’s current QoL: symptom exacerbation, psychological functioning including stress, and family support.
Health-related quality of life factors: major life transitions (eg. graduating high school and needing to manage IBD at college), fatigue ( persists despite controlled inflammation), poor body image (especially with weight changing rapidly), a diminished self-perception or seeing oneself as less capable, comorbid functional abdominal pain (about a quarter of youth with IBD), and food restrictions that can interfere with daily quality of life.
Stress plays important role influencing (bidirectional) disorders of brain gut interaction (DBGI)
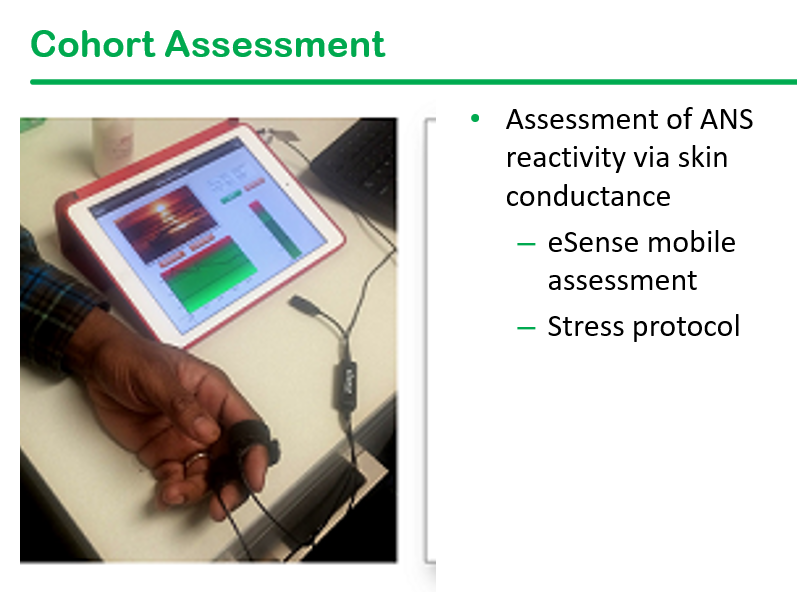
Dr. Reed’s research includes a longitudinal cohort of newly-diagnosed (w/in 45 days) pediatric patients with IBD. This cohort undergoes psychosocial assessment along with ANS assessment
Emotional reactivity indicates individuals with a ‘short fuse’ who take longer to return to normal. Those with emotional reactivity are at increased risk for anxiety/depression.
Skin conductance response (SCR) can help determine autonomic nervous system (ANS) dysfunction. It is a measure of sympathetic arousal and stress
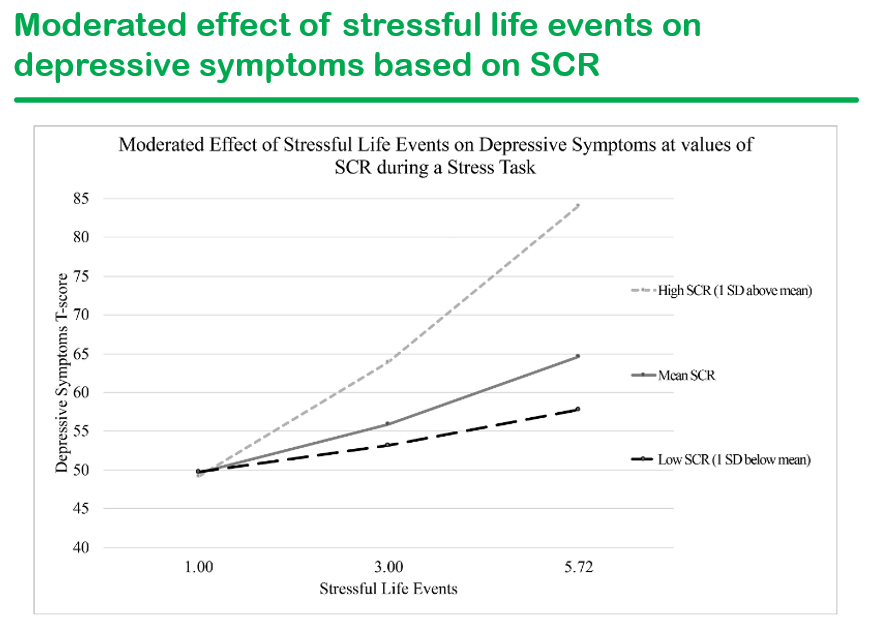
Stressful life events increase the rates of depression and correlate with skin conductance at medium and high levels
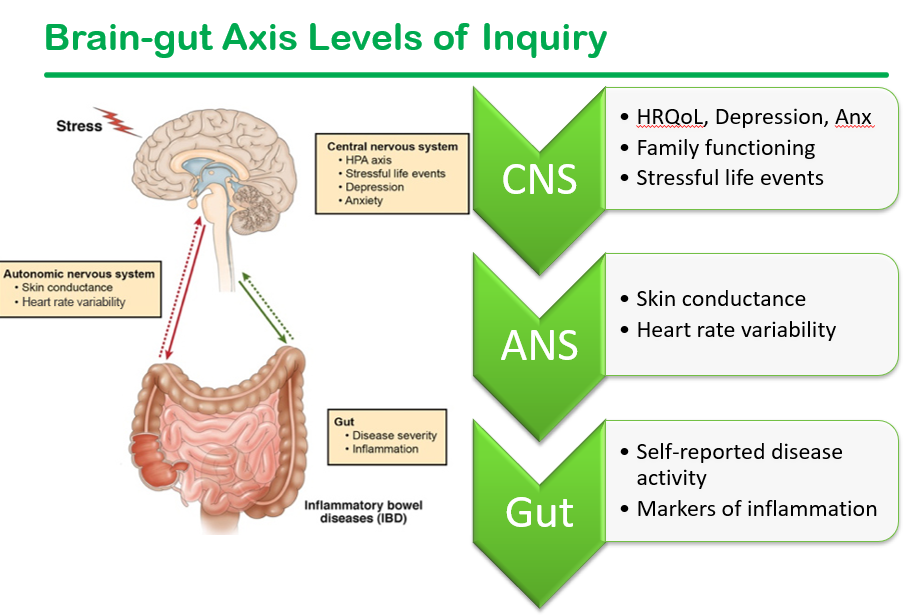
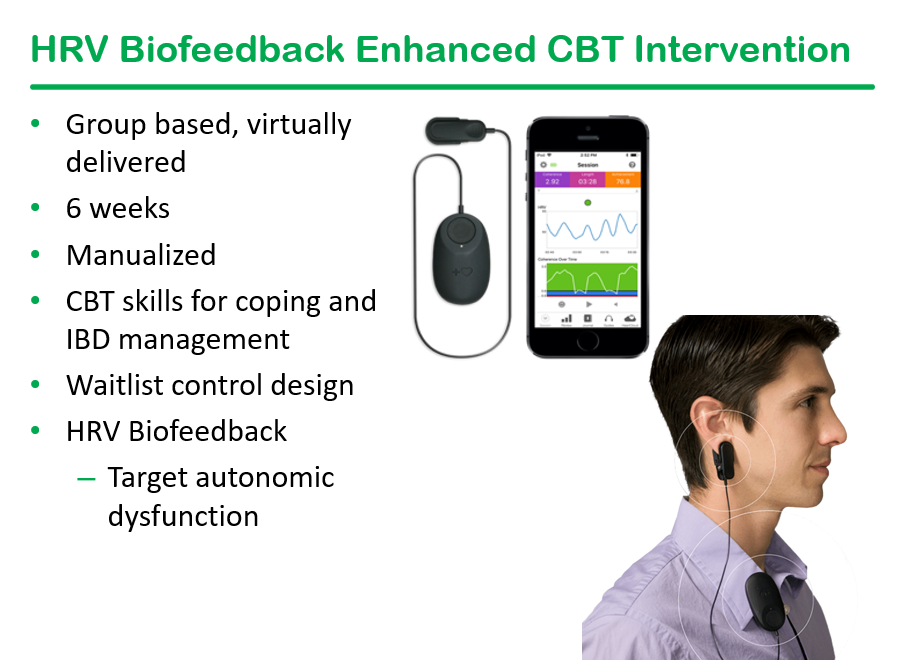
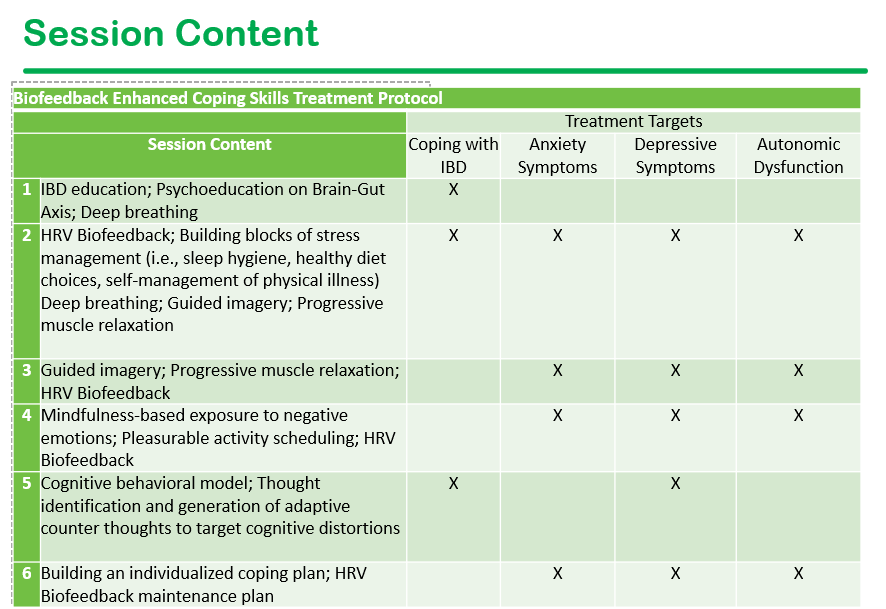
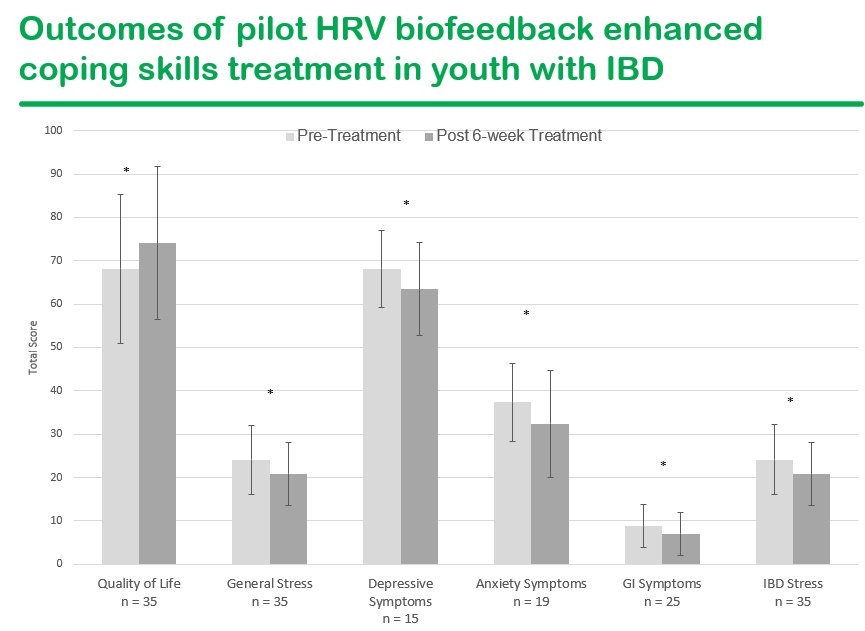
Within this model, Dr. Reed’s research focuses on the hypothesis that autonomic dysfunction is indicative of a chronic stress response. This, in turn, contributes to increased sympathetic nerve activity and decreased parasympathetic activity. This contributes to symptoms of anxiety and depression as well as GI clinical symptoms, all of which lead to impairments in QoL. Addressing autonomic dysfunction may provide a mechanism by which to address all of these QoL drivers
ANS dysfunction (which is also seen in cyclic vomiting syndrome) can improve with biofeedback focused heart rate variability (HRV). HRV, in turn, is associated with increase inflammation
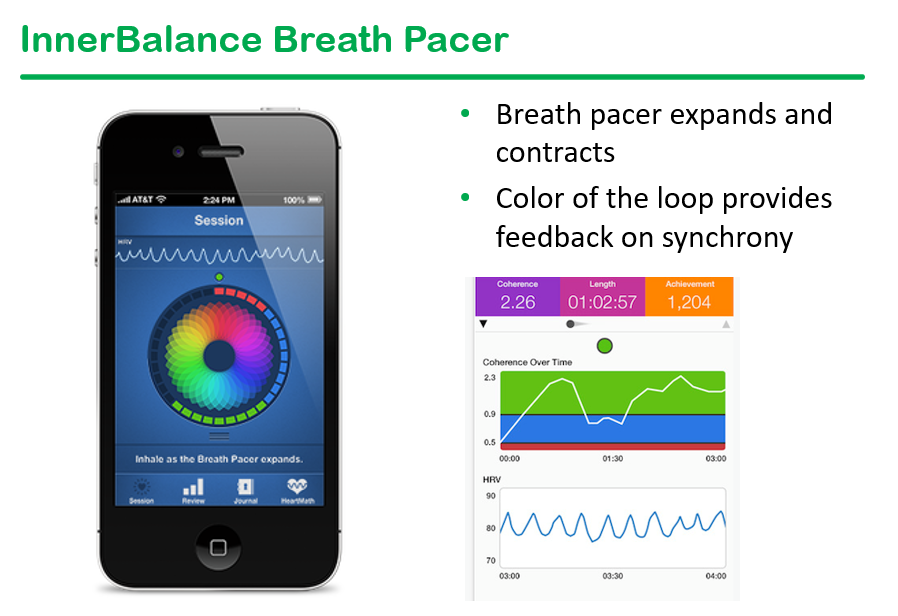
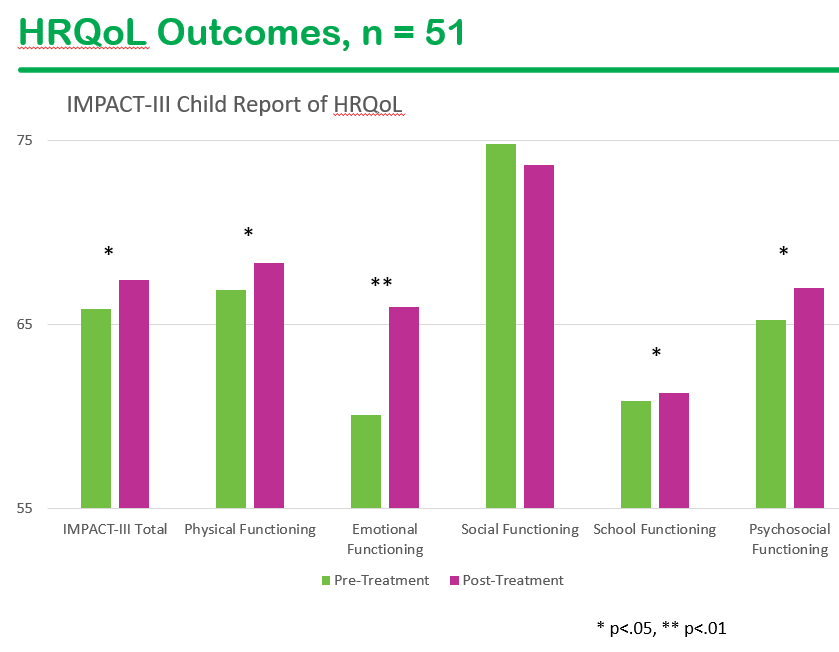
Preliminary data from breath pacer intervention has shown in improvement in multiple variables
Background: “Vaccination status cannot be verified through standard blood supply channels, patients seeking “unvaccinated” blood have increasingly resorted to directed donation from known donors…directed donations demonstrate higher rates of infectious disease marker reactivity compared with repeat community donors, particularly among first-time parental donors.25, 26“
Methods: This was retrospective review of directed donations (n=15 including 9 pediatric patients) received at Vanderbilt University Medical Center between January1, 2024 and December 31, 2025
Key findings:
Two patients clinically deteriorated in the setting of refusal of standard components
Two additional patients had surgical delay/cancellation with rescheduling associated with directed component availability
Conclusion by authors: “Directed donation pursued for “unvaccinated” blood concerns occurred across pediatric and adult settings in both elective and urgent clinical scenarios. These requests were associated with clinical deterioration, care delays, and resource inefficiencies when standard inventory products were refused.”
My take: Many families do not understand that directed donation is less safe than using the blood bank.
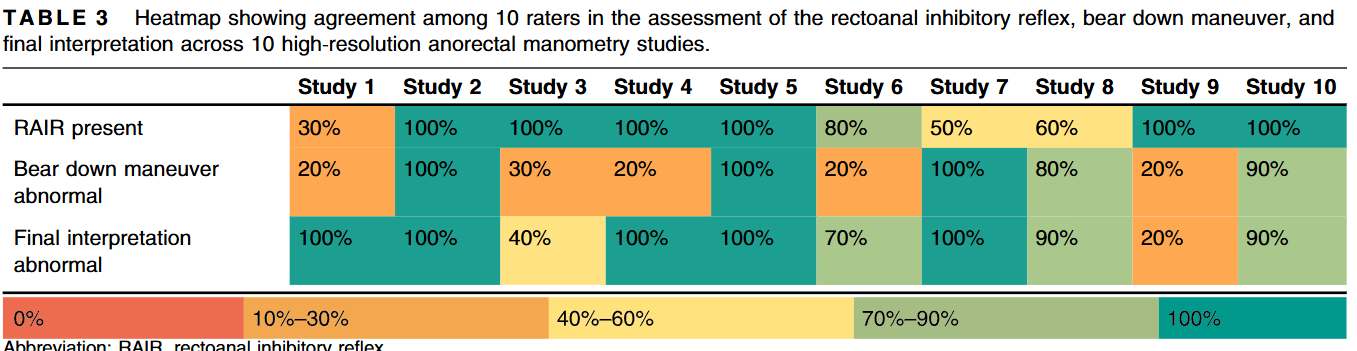
JMJ van der Zande et al. J Pediatr Gastroenterol Nutr. 2026;82:980–987. Interrater reliability in pediatric high-resolution anorectal manometry recordings
This study analyzed the interpretation of 10 pediatric high-resolution anorectal manometry (HR-ARM) by 10 pediatric experts in neurogastroenterology, including one of my partners, Dr. Jose Garza.
Key findings:
There was only fair agreement among readings with regard to rectoanal inhibitory reflex (κ = 0.35), the bear down maneuver, and the final interpretation of the study either being normal or abnormal (κ = 0.50 and κ = 0.43, respectively).
There was excellent agreement with regard to assessment of the anal canal resting pressure, the squeeze pressure, as well as the squeeze duration
My take: This is a cautionary study indicating a high-rate of variability in the interpretation of key components of HR-ARM; the results are similar to a 2012 study of colonic manometry (see below). Thus, clinical context and supporting data (eg. histology) are quite important as well for clinical decision-making.
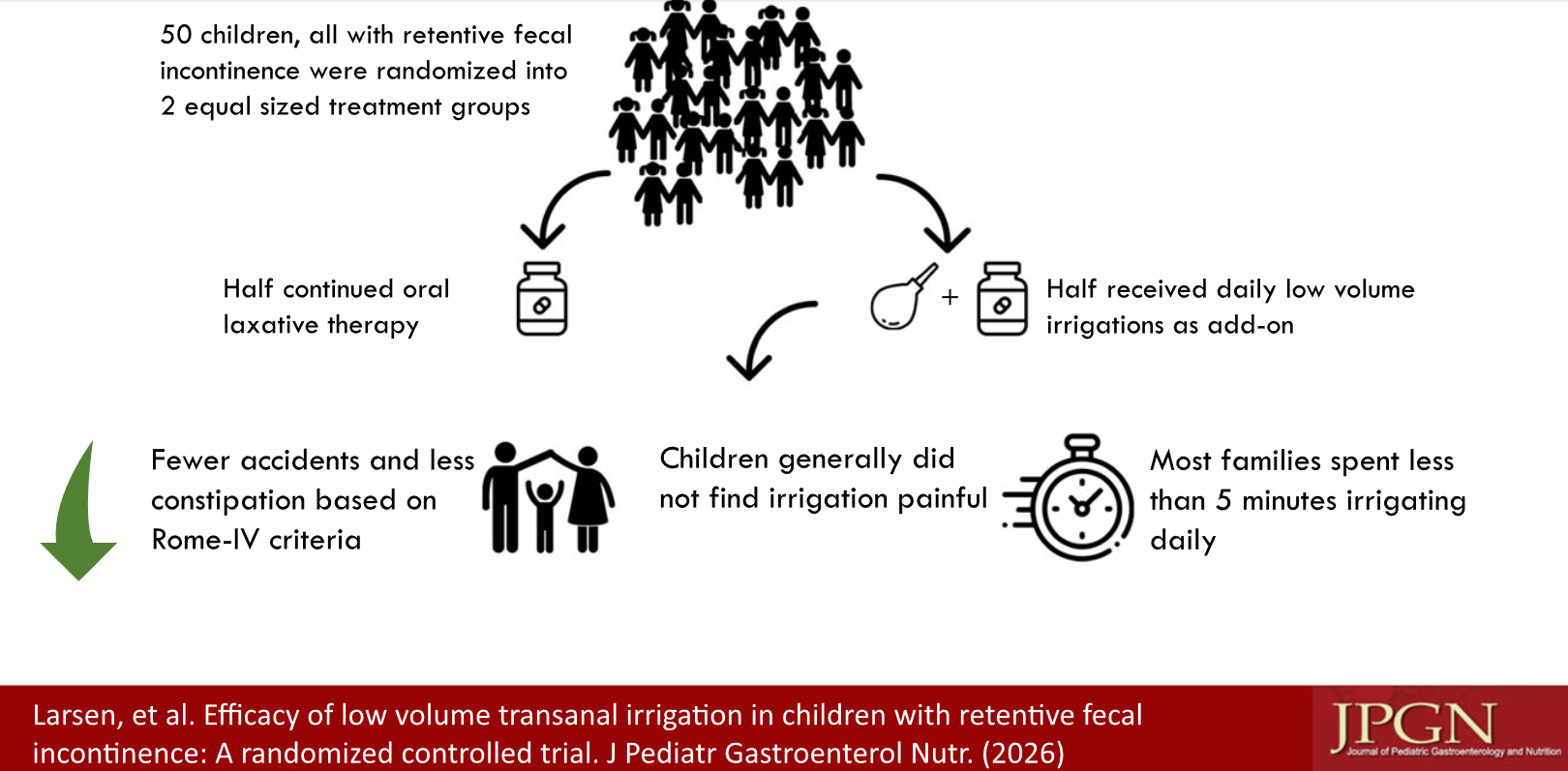
SO Larsen et al. J Pediatr Gastroenterol Nutr. 2026;82:425–433. Efficacy of low volume transanal irrigation in children with retentive fecal incontinence: A randomized controlled trial
Methods: Two-arm randomized controlled trial, including children (N=41) aged 4–14 suffering from retentive fecal incontinence. All included children were refractory to at least 2 months treatment with stool softening oral laxatives. Treatment duration was 6 weeks. The control group continued oral laxative therapy. The intervention group received low-volume transanal irrigation (L-TAI) as add-on.
Irrigations: “Irrigations were performed once daily with the Qufora IrriSedo MiniGo® Small system. According to the manufacturer the MiniGo® water pump contains 180 mL of water, with an estimated 20 mL residual water per use. Families were instructed to use 1 pump full of water to irrigate. If this did not result in defecation, they were instructed to refill and irrigate again.”
Key Findings:
In the intervention group, 75% were responders with 35% experiencing full response, while 33% in the control group were responders, with 4.8% experiencing full response
One limitation of this study, besides its sample size, is the type of laxative used prior to enrollment. Patients had been treated with PEG, magnesia or lactulose. These agents are not recommended for refractory constipation; high dose sennosides or bisacodyl have been recommended per recent position paper.
My take: Willie Sutton was a notorious bank robber who was famous for his quote (which he later denied) that he robbed banks “because that’s where the money is.” Similarly, for constipation, targeting treatment at the site of the “deposit” turns out to be an effective strategy. (I have no financial ties to the irrigation company.)
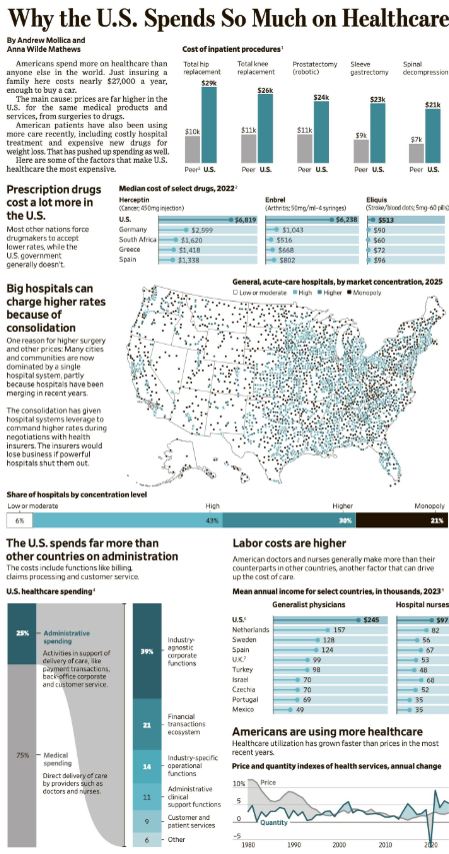
There are several insightful and concise articles that highlight the reasons for increased U.S. healthcare costs as well as challenges: corporitization of health care, private equity, and health-harming corporations.
“Americans spend more on healthcare than anyone else in the world. Just insuring a family here costs nearly $27,000 a year, enough to buy a car. The main cause: Prices are far higher in the U.S. for the same medical products and services, from surgeries to drugs.
American patients have also been using more care recently, including costly hospital treatment and expensive new drugs for weight loss.”
Prescription drugs cost a lot more in the U.S.
Big hospitals can charge higher rates because of consolidation
The U.S. spends far more than other countries on administration
This article notes that historically, in economic experiments, physicians have acted more altruistically than members of the general population and this results in better outcomes for patients. However, “extreme size and corporate ownership are leading to the widgetization of care. It is difficult or impossible for a large organization, even one with well-intentioned leaders, to avoid treating its physicians and staff like interchangeable widgets whose behavior can be monitored and controlled to maximize profit….Physicians who feel like widgets are more likely to behave like widgets…there is evidence that corporatization is leading to higher prices, higher health care spending, and unchanged quality or poorer quality.”
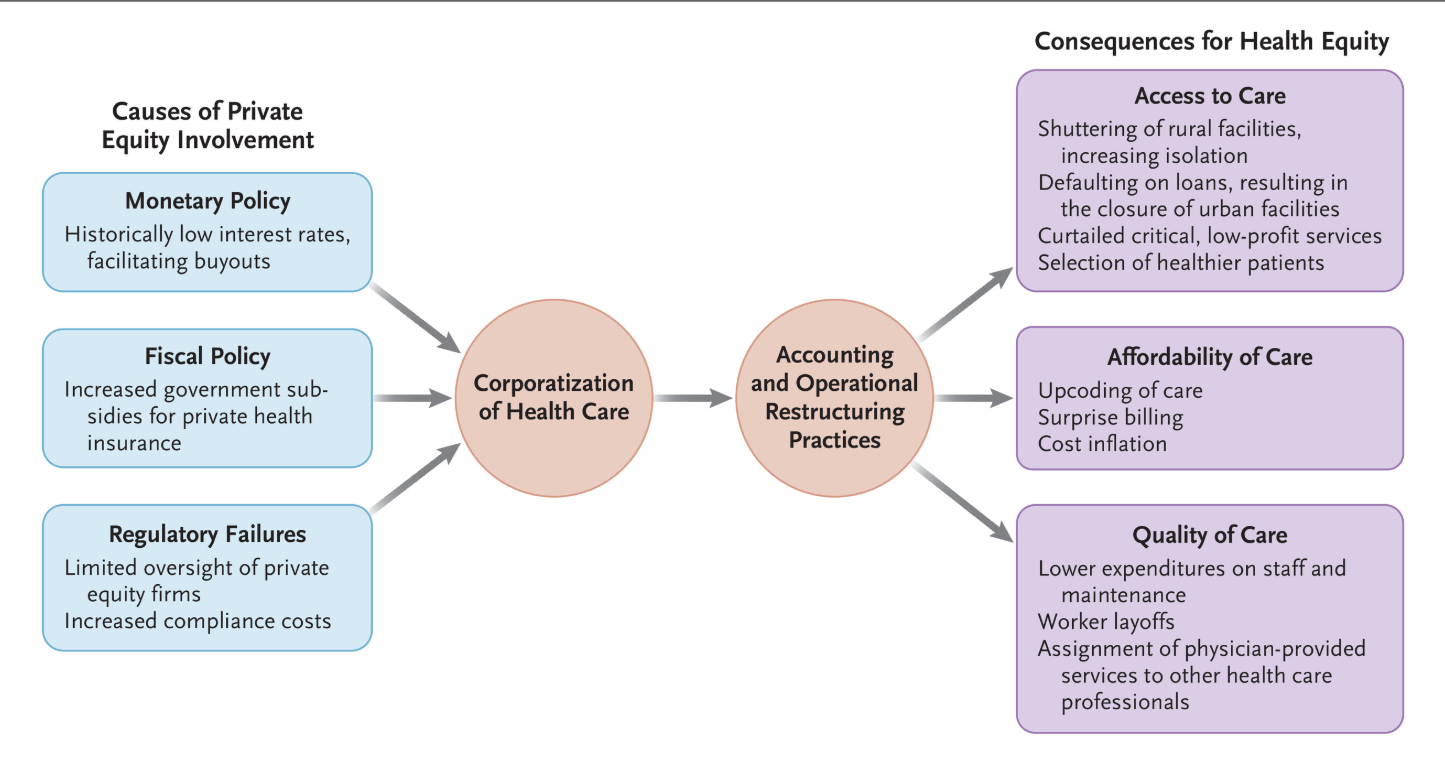
“Accumulating evidence presented in scholarly articles and government reports indicates that the proliferation of PE in health care has reduced access to care, increased costs, and compromised quality of care…PE firms often extract value using tactics that obscure a health care system’s profitability while maximizing financial returns for the firm and its investors. These tactics include sale–leaseback transactions, in which facilities are sold to entities affiliated with a firm and then leased back to the seller at inflated rates. Another strategy is dividend recapitalization, whereby fund managers take on additional debt to pay partners instead of putting money toward staff, critical maintenance, or supplies…
PE investors achieve cost savings by laying off workers, reducing salaries and the number of full-time employees, assigning services previously provided by physicians to other health care professionals, and cutting critical but low-profit services…
Cream skimming — selectively caring for healthier (i.e., lower-cost) patients — is another widely used PE practice. This tactic limits access to care for older and sicker patients, leaving them worse off after PE investment.2 Despite this behavior, hospital acquisitions by PE firms have been associated with increases in emergency department deaths and deaths after emergency surgeries.3,5“
“Health-harming corporations use common tactics to corrupt scientific data, including influencing research questions, attacking and discrediting independent science and scientists who do not support the industry’s position, suppressing scientific data on the health harms of their products, and sponsoring research that downplays those harms.27,28
For example, the primary U.S. manufacturers of perfluoroalkyl and polyfluoroalkyl substances (PFAS) — DuPont and 3M — used multiple tactics to downplay evidence of PFAS toxicity, including successfully suppressing for more than 20 years internal studies showing adverse effects of PFAS…
Corporations have various tactics for influencing the public’s beliefs about their products’ benefits and harms. These include sophisticated and pervasive advertising and marketing campaigns; use of public relations companies, front groups, and think tanks; and capture of consumer groups.
For example, opioid manufacturers deployed particularly insidious advertising strategies for marketing opioids to vulnerable populations, such as recruiting youth coaches and school nurses to encourage opioid use by children, developing unbranded initiatives encouraging adolescents to ask clinicians for pain medications, promoting “safe opioids” for untreated pain in women, and distorting policy discussions of unmet needs for pain medication…
Make America Healthy Again initiative highlights the roles of toxic chemicals and pesticides, ultraprocessed foods, and corporate influence on science in harming children’s health.47 But…the administration has appointed former lobbyists and scientists from the chemical and petroleum industries to lead EPA offices responsible for regulating air pollution, toxic chemicals, and pesticides48,49 — and plans to eliminate regulatory and other measures, which will lead to increased exposure to toxic chemicals and air pollutants, thereby increasing child health risks.50,51
My take: Poorly-regulated capitalism is not good for patients. Insurers, private equity, hospitals, pharmaceutical companies and many providers may prioritize profits over care.