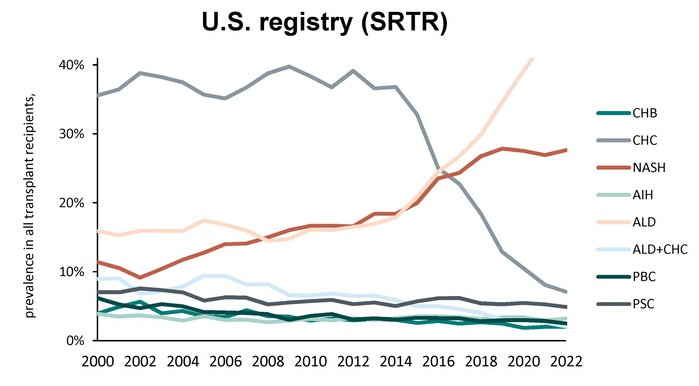
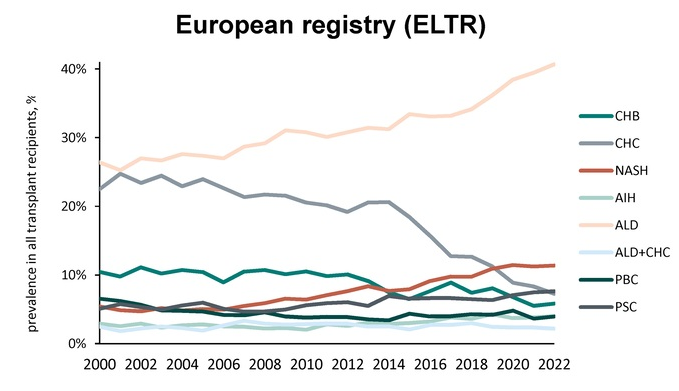
Methods: Adult data from 2 large LT registries: the US Scientific Registry of Transplant Recipients (SRTR) and the European Liver Transplant Registry (ELTR), years 2000–2022, were compared. There were 109,048 recipients of transplant from ELTR (30 countries), and 128,765 from SRTR.
Key findings:
#1 cause in 2022: Alcohol-associated liver disease (ALD) increased: SRTR 15%to 45%, and ELTR 25% to 41%
#2 cause in 2022: NASH/MASH also increased: SRTR 9% to 28%, and ELTR 5% to 12%
Chronic hepatitis C decreased: SRTR 40% to 7%, and ELTR 25% to 7%
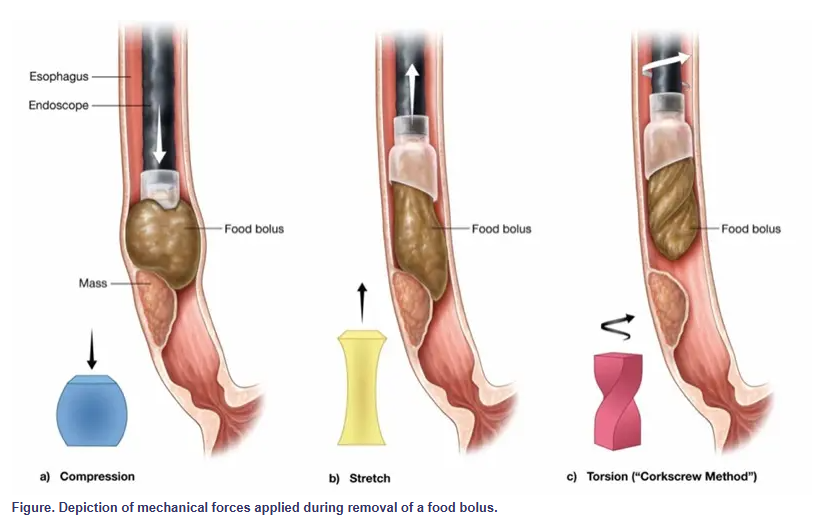
Yet, just as one wouldn’t simply yank a cork from a bottle, it may be time to rethink how we approach food bolus removal. Torsional stress—twisting rather than pulling—may provide a more efficient and atraumatic method for managing these impactions, a technique we refer to as the “corkscrew method.”
Less force is required because rotation gradually disengages the bolus, decreasing the need for strong pulling or pushing. This method also poses a lower risk for mucosal injury. Shear forces are distributed rather than focused, reducing trauma.
My take: This is probably worth a try for the next food impaction requiring endoscopic removal.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Methods: The authors calculated IBD polygenic scores (PGS) for 3732 Danish patients with Crohn’s disease (CD) and 4535 patients with ulcerative colitis (UC), and investigated their association with disease outcomes.
“The Danish National Biobank stores neonatal blood spots from almost all Danes born since 1982…The North Denmark IBD (NorDIBD) cohort is a population-based cohort of all patients from the North Denmark Region with a confirmed IBD diagnosis from 1978–2020.17 From this cohort, 940 patients with IBD and a further 973 blood donors with no IBD diagnosis were genotyped from whole blood…applied variant loadings for calculating PGS for CD and UC susceptibility generated by Middha et al19 to our dataset. These variant loadings were derived from summary statistics from the IIBDGC.” This cohort had a young age. Only 2% and 3% of CD and UC patients, respectively, were 40+.
Severe Disease Definitions:
For patients with CD, a severe disease course was defined as experiencing (1) 2 or more IBD-related hospitalizations exceeding 2 days, (2) 2 or more IBD-related major surgeries, (3) 1 IBD-related hospitalization and 1 IBD-related major surgery not overlapping in time, or (4) a total use of at least 5000 mg prednisolone-equivalent systemic corticosteroids within the first 3 years after diagnosis
For patients with UC the severity definition was modified to experiencing (1) 2 or more IBD-related hospitalizations exceeding 2 days, (2) 1 or more IBD-related major surgeries, or (3) a total use of at least 5000 mg prednisolone-equivalent systemic corticosteroids.
Key findings:
Increased PGS was associated with higher fecal calprotectin and C-reactive protein levels, and decreased hemoglobin levels
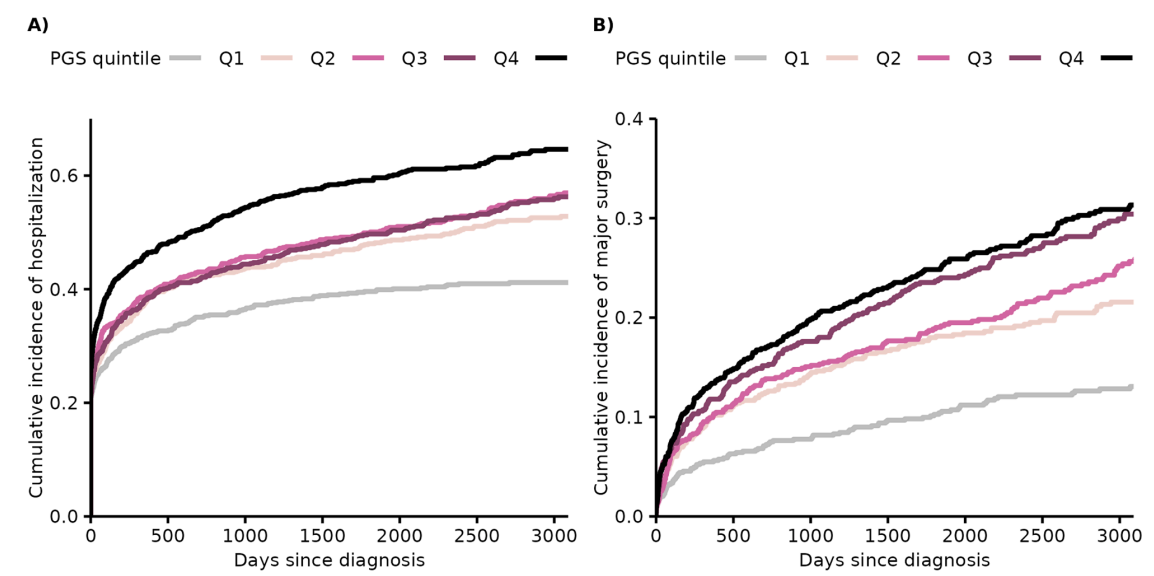
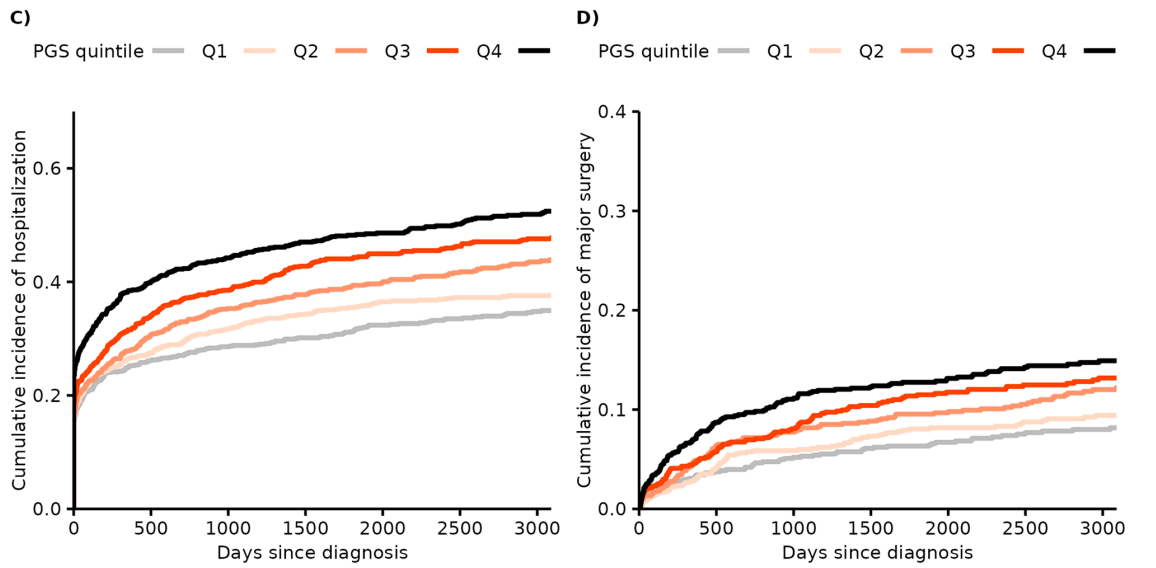
When comparing the highest vs lowest PGS quintile, we observed a hazard ratio for major surgery of 2.74 in patients with CD and of 2.04 in UC
Patients with severe disease had higher PGS than patients with less severe disease (CD, odds ratio = 1.25; UC, odds ratio = 1.33)
The graphs below show the differences in hospitalization and surgery based on PGS for CD (A & B) and then for UC (C & D)
Discussion:
“Our results suggest that IBD susceptibility genetics only explain part of the severity of IBD, hence leaving room for other factors at play… This observation is promising, as it points toward the possibility of modulating the effects of genetic susceptibility through lifestyle interventions directed toward potential environmental factors that are yet to be uncovered.”
My take: It is intuitive that those with more genetic risk factors would be more likely to have severe disease. This study shows this assumption is correct in this cohort; in fact, there is a dose-response relationship. Those with higher PGS had more hospitalizations, major surgeries and medical treatments.
Methods: In this review/meta-analysis with 35 eligible studies, there were 1,002 adult participants with celiac disease (CeD) in remission on a gluten-free diet undergoing a gluten challenge (GC).
Key findings:
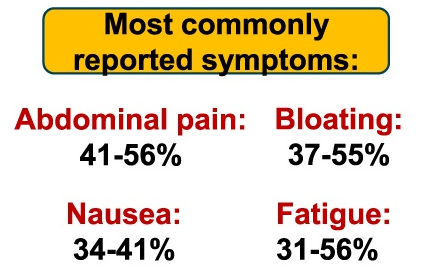
The most common symptoms were abdominal pain (41-56%), bloating (37-55%), and nausea (34-41%). The lower numbers were the composite result from non-randomized controlled trials; the higher numbers were reported in randomized controlled trials
Diarrhea was reported in 29-38%
Bloating, fatigue, flatulence, and nausea were significantly more reported in studies administering ≥6 g gluten/d
My take: The symptoms that occur with a gluten challenge are likely similar to those with inadvertent intake. However, with inadvertent gluten exposure, the amount of gluten could be substantially more and increase the severity of symptoms.
Since I completed my pediatric residency and pediatric gastroenterology fellowship in Cincinnati, I receive their bulletins. A recent title (Link: EoE: The Fifth Member of the Atopic March) prompted me to review the source article. The Cincinnati summary noted that “children with AD [atopic dermatitis] within the first two years of life are 10 times more likely to develop EoE [eosinophilic esophagitis] by age 8.”
Background: The atopic march refers to the natural history of allergic disease manifestations as they develop in childhood.1 Classically, the march begins with atopic dermatitis (AD), followed sequentially by food allergy (FA), asthma, and allergic rhinitis (AR),1 but there is significant heterogeneity in the timing, order and organ(s) affected.2
Methods: Using the Mechanisms of Progression of Atopic Dermatitis to Asthma in CHildren (MPAACH) cohort,4 a US longitudinal early-life cohort of children (n=700) with AD, the authors examined the associated epidemiology of EoE with other members of the atopic march.
Key findings:
“Of 700 MPAACH participants, 10 have EoE, and in all cases, EoE developed after AD onset. Of these 10 subjects, 2 had EoE at enrollment, whereas 8 developed EoE subsequent to enrollment in MPAACH”
“To date, 48.9% of the children in MPAACH had developed at least 1 allergic comorbidity (FA, AR, and/or asthma) by age 8 years versus 90% of the children with EoE (P = .009), highlighting the strong association between EoE and other atopic diseases”
“Despite no difference in skin barrier quality or AD severity, the children with EoE were significantly more likely to have food sensitization (as defined by at least 1 positive result of a skin prick test to a food allergen [60% vs 28% (P = .039)]) and FA (70% vs 13% [P < .001])…suggesting that the esophageal epithelium may be the site of allergen penetration and immune activation, independent of the skin barrier”
My take: There was a 10-fold higher risk of EoE (1.4% or 10 of 700) in this cohort of children with AD compared to the general population. However, I was expecting a much higher prevalence in this population. This could be due to the fact that patients are seeing me for GI symptoms rather than for AD. It is possible, as well, that the number of EoE patients would be higher if there was a prospective evaluation (e.g. endoscopy).
Eczema Rarely Linked to Food Allergy Dave Stukus: Many parents are told that if they can find the ‘cause’ of their child’s eczema and eliminate exposure, then their skin will improve. Unfortunately, this is not the case because the cause of eczema is a disrupted skin barrier, which leads to excessive water loss, dryness and itching.Children with eczema, especially those with persistent, severe cases affecting most of their body, are at higher risk to develop allergies and asthma as they get older….In rare instances, specific foods may be a major contributor to a child’s eczema, but this is the exception and typically affects infants less than one year of age with truly unmanageable, severe eczema, despite good daily skin care.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition
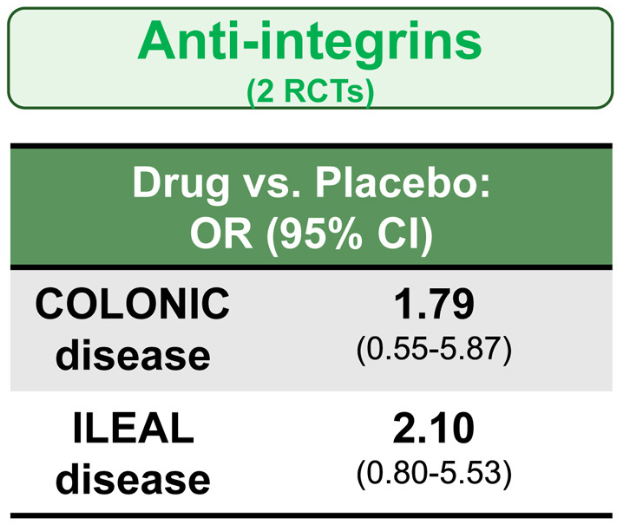
Methods: In the study by Lee et al, the authors identified 14 randomized controlled trials in 3139 patients with moderate-to-severe CD who were treated with different advanced therapies vs placebo, and reported efficacy in inducing clinical remission, stratified by disease location (isolated colonic vs ileal disease, excluding ileocolonic disease). The authors did not identify any RCT of TNF antagonists that reported induction of remission by disease location.
Key findings:
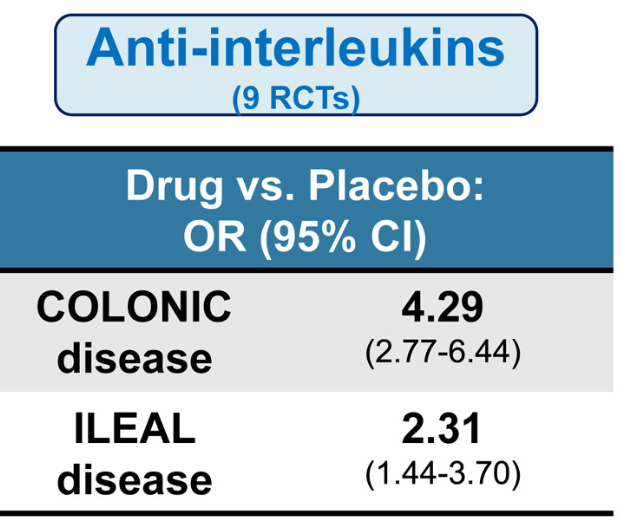
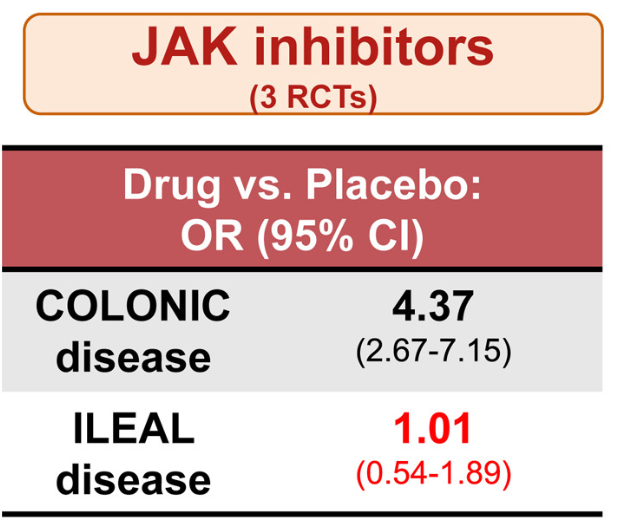
All advanced therapies had better success with colonic disease rather than ileal disease
Anti-interleukins (eg. IL23 o rIL12/IL23 agents) worked best for ileal disease among these advanced therapies
JAK inhibitors did not work well for ileal disease, but performed well for colonic disease
Anti-integrins, like vedolizumab, had some efficacy for ileal disease but generally a lower clinical remission rate than other agents
Lmitations included the use of clinical remission as the primary outcome
While this study did not provide data on anti-TNF therapy, in the discussion the authors note that “TNF antagonists may have advantages in small bowel CD…infliximab demonstrated the highest rate of improvement in large ileal ulcers (>0.5 cm).” [ref#45] “Additionally, infliximab has been reported to reduce fibrostenosis-associated inflammation, [Ref#46] making it currently the most suitable therapeuctic option for small bowel CD.”
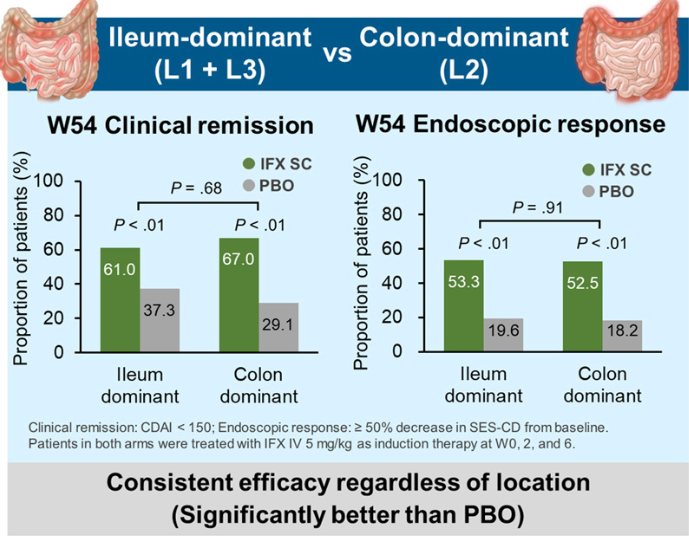
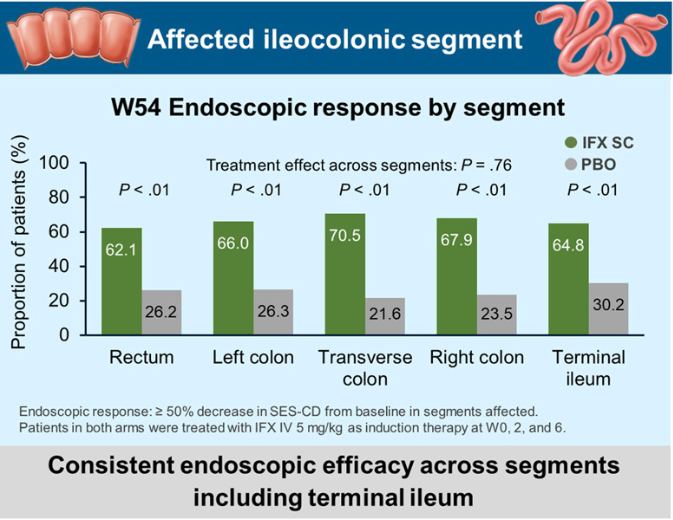
In the study by Sands et al, this post-hoc analysis included week 10 responders (n=329) to intravenous IFX induction therapy who were randomized to receive IFX SC 120 mg every 2 weeks or placebo (PBO) during maintenance therapy.
Key findings:
My take: These two studies indicate that anti-TNF agents (particularly infliximab) and IL-23 type agents are most effective for Crohn’s disease affecting the ileum. JAK inhibitors are best for colonic disease.
“The daily pill, called Foundayo [orforglipron], follows the approval of Novo Nordisk’s Wegovy pill in recent months. The lowest dose is expected to cost $149 a month for people paying out of pocket…Foundayo will be offered in six doses, with patients typically starting on the lowest dose and working their way up to reduce side effects. It can be taken at any time of day without meal restrictions — unlike the Wegovy pill, which must be taken on an empty stomach each morning…Phase 3 clinical trial data found that Foundayo helped people lose 12.4% of their weight, on average, at its highest dose after 72 weeks — similar to the Wegovy pill but less than injectable versions of Wegovy and Zepbound.”
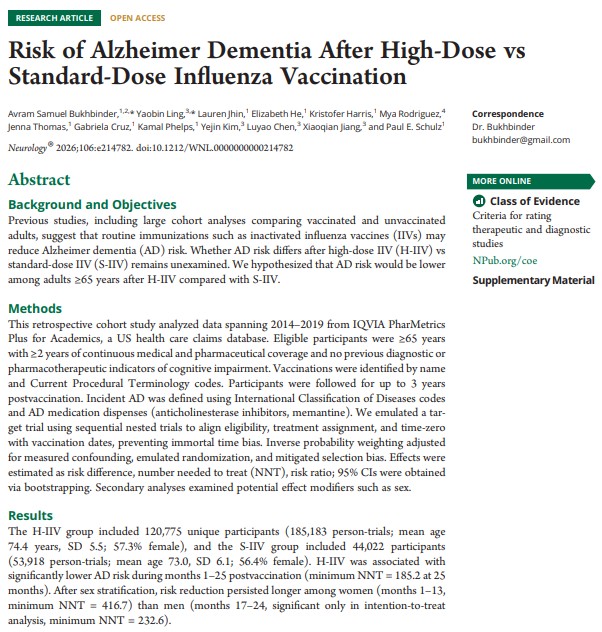
This was a retrospective study comparing the high dose influenza vaccine (H-IIV) compared to the standard dose (S-IIV) in 65+ patients. The H-IIV group included 120,775 unique participants (185,183 person-trials; mean age 74.4 years, SD 5.5; 57.3% female), and the S-IIV group included 44,022 participants (53,918 person-trials; mean age 73.0, SD 6.1; 56.4% female).
Key findings:
H-IIV was associated with significantly lower AD risk during months 1–25 postvaccination (minimum NNT = 185.2 at 25 months), with a stronger effect among women.
“Routine childhood immunizations in the United States from 1994 through 2023 are estimated to have prevented roughly 508 million illnesses, 32 million hospitalizations, and more than 1 million deaths. Those gains translated into approximately $540 billion in direct medical cost savings and nearly $2.7 trillion in total societal savings. Put simply, every $1 spent on childhood immunizations generated about $11 in savings…Adult vaccination also produces meaningful economic gains, particularly through reduced absenteeism, less presenteeism, and better labor-market continuity. Evidence suggests that adult immunization programs can return up to 19 times their initial investment.”
“In South Carolina, a 2025–2026 outbreak with 993 cases generated an estimated $35.5 million in costs, compared with $66,193 to vaccinate the same number of children through VFC. Those costs are only growing – the outbreak in South Carolina has not yet abated.”
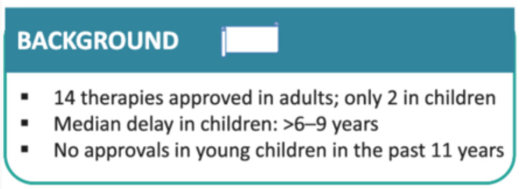
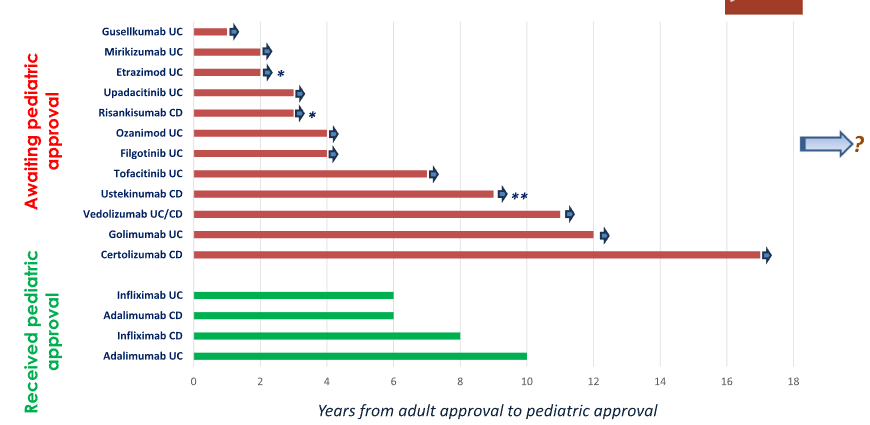
D Turner et al. J Pediatr Gastroenterol Nutr. 2026;82:867–894. Reshaping study design for faster extrapolation‐baseddrug approval in pediatric inflammatory boweldiseases: An ESPGHAN–NASPGHAN position paper
“It has been 11 years since the adult approval of vedolizumab and 9 years since the approval of ustekinumab, yet neither is currently approved for use in children (Table 1). Instead of taking the necessary steps to shorten this unacceptable delay, there are now extra hurdles for clinical trials such as three ileocolonoscopies over 1 year in both pediatric CD and UC, as suggested by the FDA…”
Addendum: See comment by Matthew Kowalik, MD who is the Director (Acting) of Division of Gastroenterology for FDA/CDER/OND/OII. There has been recent approval recent of Stelara (ustekinumab) for the treatment of pediatric patients 2 years and older with moderately to severely active Crohn’s disease. Here’s a link: Johnson & Johnson (JNJ) Gains FDA Approval for Pediatric Crohn’s Disease Treatment
“Pediatric extrapolation is based on assessing relevant similarities in disease characteristics, drug pharmacology, and treatment response between the target pediatric population and adults or other reference pediatric populations. While, historically, extrapolating safety data was considered unacceptable, the recent International Council for Harmonization (ICH) E11A Guideline on pediatric extrapolation that has been endorsed in 2024 by the EMA”[European Medicines Agency (EMA) ]
Selected Summary Statements (total of 24 are in the report):
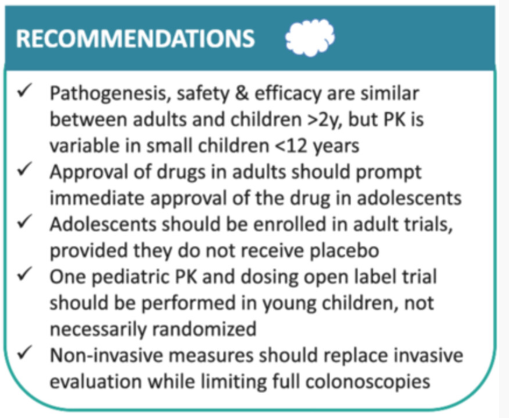
1.There is no evidence that differences in pathogenesis and pathobiology between pediatric and adult patients with IBD are associated with differences in response to pharmaceutical therapies, except for monogenic disease (agreement 21/22).
2.In general, efficacy and drug-related safety outcomes in children older than 2 years are comparable to adults (agreement 22/22).
9. Optimal dosing should be used in all study arms in pediatric trials. Placebo, sham, or doses demonstrated to be subtherapeutic in prior studies should not be permitted. They are unethical in children, reduce feasibility of enrollment, and are not expected to be informative given the underpowered sample size of pediatric studies (agreement 22/22).
13.Ileocolonoscopic assessment is the gold standard for assessing mucosal healing (MH) and should be required at most twice in each study: that is, at baseline and study end (agreement 22/22).
14. Noninvasive objective measures, including serum and fecal biomarkers, magnetic resonance enterography (MRE), and/or intestinal ultrasound (IUS), should be used for assessing postinduction interim therapeutic response between the two ileocolonoscopies rather than requiring a third ileocolonoscopy (agreement 22/22).
My take (borrowed from the authors):
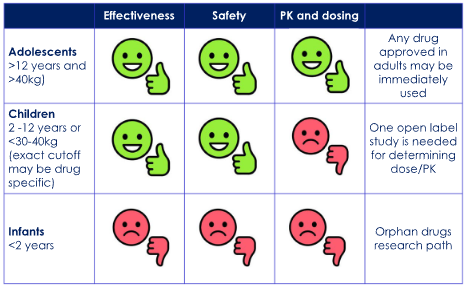
“While it is paramount to achieve a precise and comprehensive approval process for new drugs in pediatric IBD, it is equally important to expedite the process, so children and adolescents are not denied effective treatment available for adults with IBD…”
“Under these assumptions, future trial designs should be single-arm and open-label to focus on dosing and pharmacokinetics in children weighing <30–40 kg while mandating long-term safety registries, disease- and not necessarily drug-specific. Data should be supported by meticulously collected real-world evidence. Pediatric data must be collected as soon as a confident signal of efficacy and safety is achieved in adult studies…”
“This will resolve the current paradox in which children have the most severe and extensive disease and the highest efficacy of drugs, yet very limited access to these drugs.”
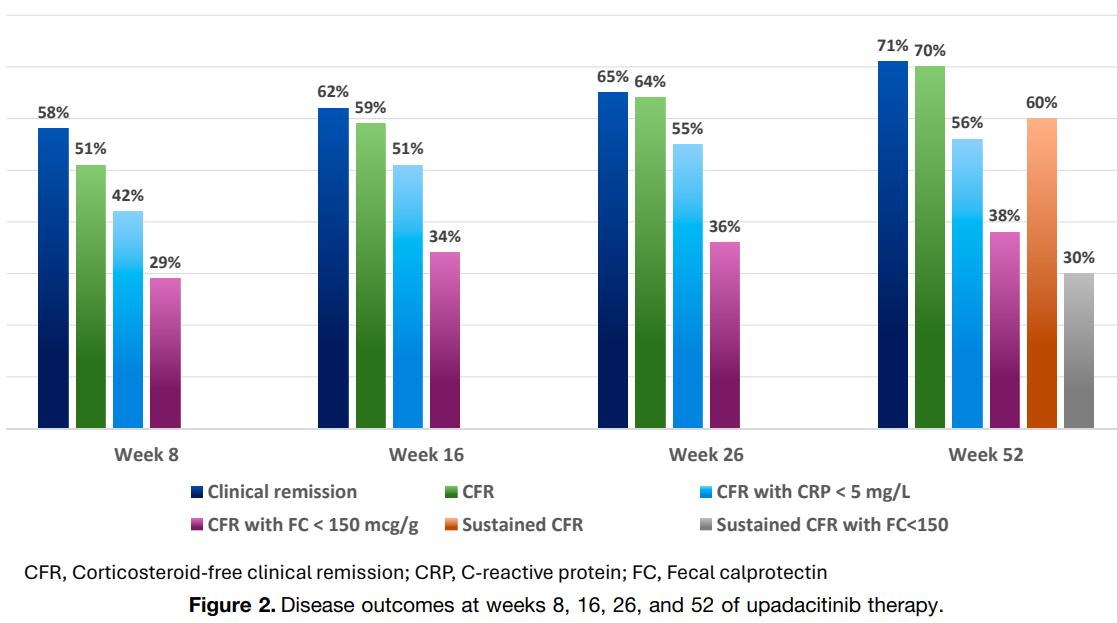
Background/Methods: There is limited data on the use of upadacitinib for pediatric inflammatory bowel disease. This retrospective data from 35 European centers analyzed its effectiveness in 105 children (95 with UC and 10 with IBD-U). Prior to upadacitinib, 103 of 105 children (98%) were treated with biologic therapies and 79 (75%) with ≥2 biologics. The induction dose was 45 mg in 86% of cohort; the maintenance dose was 30 mg in 87% (only 2 patients received 45 mg maintenance). Mean age at IBD diagnosis was 11.3 yrs and mean age at start of upadacitinib was 14.6 yrs. 65% of study participants had a pancolitis.
Key findings:
Clinical remission and corticosteroid-free clinical remission (CFR) were observed after 8 weeks in 61 (58%) and 53 (51%) children, respectively
By week 52, 75 children (71%) achieved clinical remission, 73 (70%) achieved CFR, and sustained CFR in 63 (60%); CFR with FC <150 mcg/g was reached 30 of 80 (38%) (29% of the ITT group)
Adverse effects: There were two serious AEs: an appendiceal neuroendocrine tumor and cytomegalovirus colitis. The most frequent AEs were hyperlipidemia (n = 20), infections (n = 18), and acne (n = 14)
Predictors of response: “The baseline variables that were associated with achieving sustained CFR were prior failure of fewer biologic agents (≤2 vs >2), a lower PUCAI score, absence of corticosteroid therapy, and higher serum hemoglobin and albumin levels.”
Age: “Our findings suggest that upadacitinib provides comparable effectiveness in younger children weighing <40 kg, supporting its therapeutic potential across a broader pediatric age and weight range.”
My take: Upadacitinib is an important therapy for ulcerative colitis in the pediatric age range and in adults. It is effective in all age groups. Also, young children can now be prescribed a liquid version (Rinvoq LQ) which requires twice daily dosing (rather than once a day). Some patients who do not respond adequately or lose response may benefit from higher dosing.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
In the first article by Jaafari et al, the authors identified four predominant food cluster patterns from 54,127 participants from 26 countries who completed online questionnaires. The highest prevalence of IBS was associated with cluster A (including Egypt, Brazil, and Colombia) and the lowest with cluster D from several Asian countries. Cluster A dietary pattern was “rich in FODMAPs.” Cluster D participants reported the highest frequencies of fish, rice and tofu consumption and lowest milk consumption (which could be due to higher rates of lactose intolerance). The limitations from this study include the reliance on a questionnaire, the small number of foods surveyed (10), and cultural differences in reporting symptoms.
The study by Mikhael-Moussa et al examined carbohydrate malabsorption, based on breath testing, in patients diagnosed with disorders of gut-brain interaction (DGBI). Patients completed questionnaires as well.
Key findings:
Among the 301 patients with DGBI included in our analysis, 178 (59.1%) had carbohydrate intolerance
Carbohydrate-intolerant patients were significantly more likely to be female (P value < 0.001), to have 2 or more DGBI (P value = 0.001) to have lactose maldigestion (P value< 0.001) and fructose malabsorption (P value = 0.023), higher irritable bowel syndrome and somatic symptom severity, and lower quality of life (P value < 0.001) compared with patients without carbohydrate intolerance
Discussion:
There are multiple potential reasons why certain foods can contribute to GI symptoms including malabsorption, gastrointestinal mobility, alterations in intestinal microbiota, intestinal distention, fluid accumulation, and localized IgE-dependent reactions (noted with confocal laser endomicroscopy).
“Carbohydrate-reduced diets have been found effective in reducing symptoms in patients, regardless of the presence of maldigestion/malabsorption”
My take: Dietary triggers are important for the majority of patients with IBS. In this study, patients with documented carbohydrate malabsorption had increased severity of their symptoms.