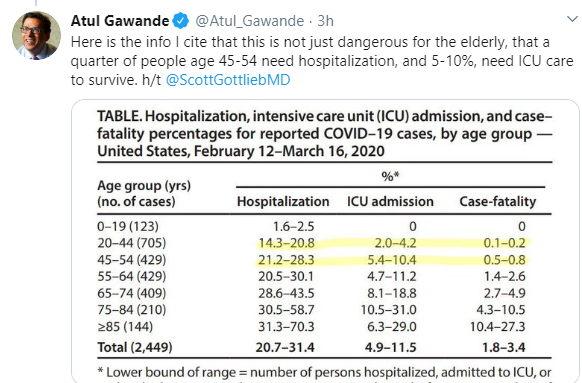
NPR’s website has a good tracker of what is going in each state. Here’s the link:
NPR: Map: Tracking The Spread Of The Coronavirus In The U.S One example: on this tracher, in Georgia, March 27, 8:30 am: 1642 reported cases, 56 deaths. (However, Georgia has conducted less than 10,000 tests in a population of more than 10 million).
——————–
A recent review (M Kay, R Wyllie. JPGN 2020; 70: 280-4) provides some practical tips for improving polypectomy technique.
Key points:
The optimal position for the polyp is in the 5-7 o’clock position.
- Snaring juvenile polyps close to the head rather than close to the colonic wall “allows for easier therapeutic intervention if polypectomy bleeding occurs” (eg. hemoclip) and may lower the risk of complications like perforation
- Epinephrine volume reduction (for larger polyps) (use 1:10,000 dilution) and saline-assisted polypectomy may facilitate procedure. Large polyps (>2 cm) could require piecemeal resection; epinephrine reduction may result in a decreased size as well.
- “Cold snare technique has replaced use of hot biopsy forceps in adults for removal of small sessile polyps”
- Electrosurgical units (ESUs) -settings are specific to each unit. Newer ‘smart’ ESUs have suggested default settings, typically lower settings for right colon. “Most endoscopists use pure coagulation current or a combination of coagulation and cutting settings (blended current) for snare polypectomy. Use of pure cutting current without coagulation will result in bleeding.”
Related blog posts:
- How Benign Are Juvenile Polyps?
- Adverse Events Following Pediatric Endoscopy -Previously Underestimated
- ESPGHAN Juvenile Polyposis Position Paper
- While the polyps described are not tubular adenomatous polyps, it is noted that guidelines in adults recommend followup in 5-10 years for a single (non-serrated) adenomatous polyp (Polyps: Clinical Decision Tool).
- Updated Guidelines on Genetic Testing/management for Hereditary GI Cancer Syndromes
- Surprising Genetic Mutations in Polyposis Study
- Polyposis in Pediatric Patients -Review
- Consensus guidelines after polypectomy | gutsandgrowth)
- Adenoma Detection Rate: Life or Death Quality Measure
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition