A recent NY Times commentary: “Where the Frauds Are Legal” details another group of problems with health care economics. These problems are on top of a long list of other problems which at their core relate to lack of price transparency/hidden charges and excessive charges for some services.
Here’s an excerpt:
Much of what we accept as legal in medical billing would be regarded as fraud in any other sector…
Medical Swag…Companies are permitted by insurers to bill for “durable medical equipment,” stuff you receive for home use when you’re in the hospital or doctors’ office. That yields some familiar marked-up charges, like the sling you can buy at Walgreens for $15 but for which you or your insurer get a bill for $120 after it is given to you at urgent care…
The Cover Charge…Trauma activation fees have been allowed since 2002, after 9/11, when the Trauma Center Association of America, an industry group, convinced regulators that they needed to be compensated for maintaining a state of “readiness.”…
Impostor Billing…We received bills from doctors my husband never met… for bedside treatment from people who never came anywhere near the bed to deliver the care…
The Drive-By…There was no significant health service given. Just an appearance and some boxes checked on a form. It’s a phenomenon called drive-by doctoring.
The Enforced Upgrade…[like meeting] in the emergency room [because clinic is closed]
Why do insurers pay? Partly because insurers have no way to know whether you got a particular item or service. But also because it’s not worth their time to investigate the millions of medical interactions they write checks for each day. Despite the advertised concern about your well-being, as one benefits manager enlightened me: They’re “too big to care about you.”…these are all everyday, normal experiences in today’s health care system, and they may be perfectly legal. If we want to tame the costs in our $3 trillion health system, we’ve got to rein in this behavior, which is fraud by any other name.
My take: I find it troubling to be a cog in a system that has such devious billing practices. This particularly relates to my interactions when providing hospital-based care. In our office, we have at least some measure of control and we can offer services like outpatient endoscopy at one-third of the cost compared to hospital-based endoscopy; similarly, our outpatient infusions are much more cost-effective than hospital-based infusions.
In terms of the health care system, my expectation is that there is not a strong enough incentive or empowerment for physicians to tackle rising health care costs (& low value care) and as such the industry will face a reckoning from outside forces.
Related blog posts:
- Why Are So Many “Low Value” Endoscopies Performed?
- Do you know about the “Choosing Wisely… | gutsandgrowth
- Deriving Measures of High Value Pediatric Care | gutsandgrowth
- Value-based care | gutsandgrowth
- Implementing High-Value Care | gutsandgrowth
- What physicians can learn from fast-food restaurants… | gutsandgrowth
- 5000% Increase for Well-Established Drug | gutsandgrowth
- Some Hospitals Marking Up Treatments By As Much As 1000%
- Cornering the Generic Markup | gutsandgrowth
- Considering Cost in Treatment Choices | gutsandgrowth
- Improving the Value of Pediatric Colonoscopy
- Colonoscopy and Isolated Abdominal Pain = Low Value Care
- Anti-TNF Therapy: Might Save Your Health But Not Your Wallet
- Don’t miss the gorilla!
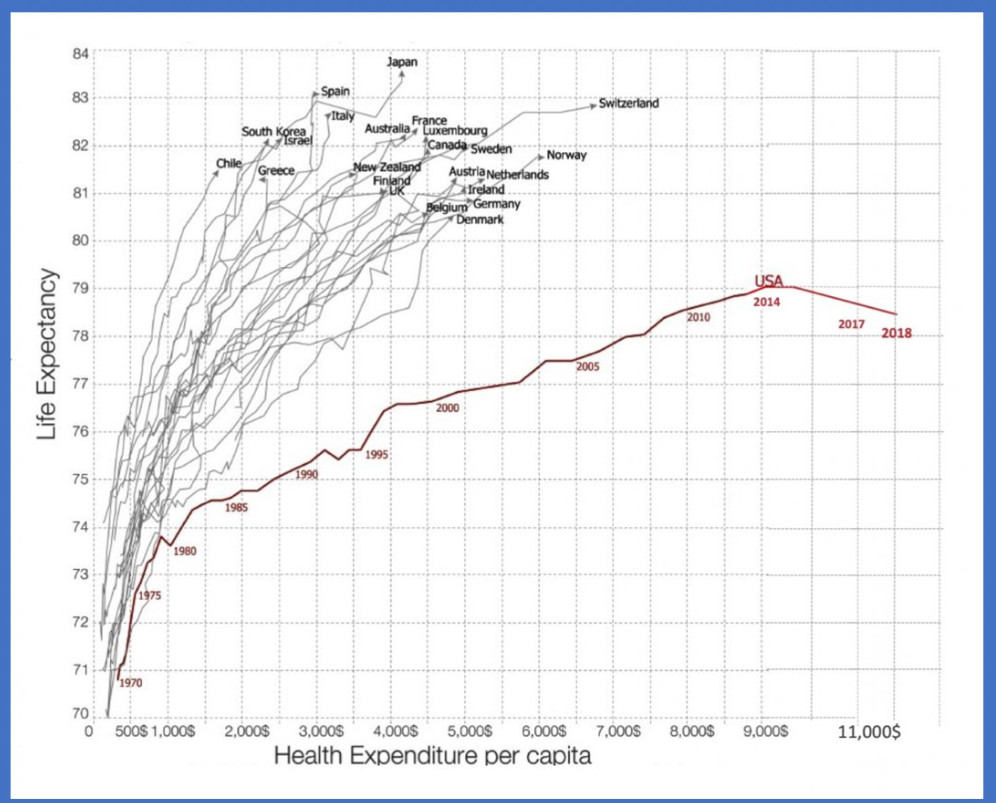
- Healthcare Costs Rising -Graphic Image