This year I had the opportunity to give a lecture to our group that reviewed much of the important advances that happened in 2024. Here are some of the slides (if you have any trouble reading the slides, you can search for the original blog post using author name).
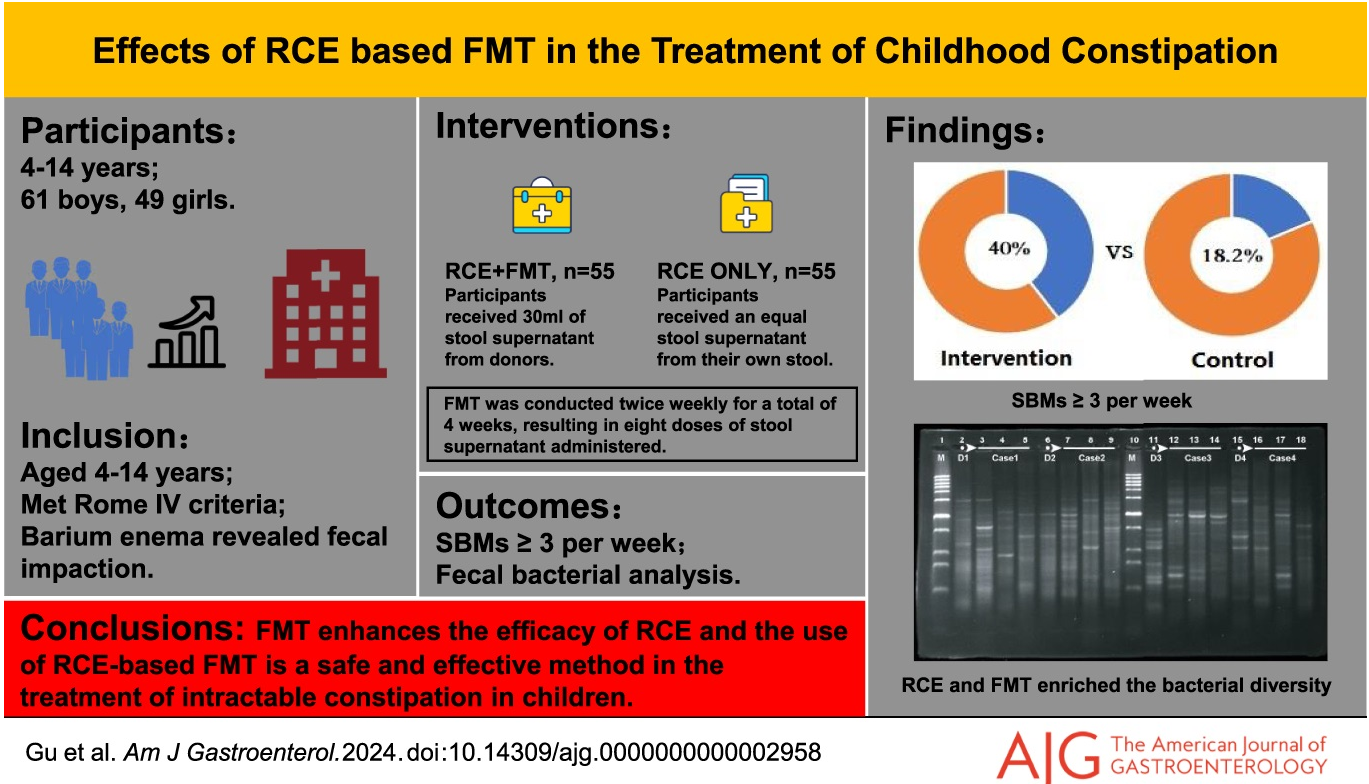
Methods: The efficacy of retrograde colonic enema (RCE) with fecal microbiota transplantation (FMT) was studied in a randomized, double-blind, controlled trial with 110 children. The initial cohort recruited was 576 patients; however, 466 were excluded for not meeting inclusion criteria. All participants received a daily RCE, followed by a 4-week FMT treatment (twice a week) and a 12-week follow-up period.
Key findings:
At the end of the follow-up period, 22 patients (40.0%) in the FMT with RCE group and 10 patients (18.2%) in the placebo with RCE group had ≥ 3 spontaneous bowel movements per week
There was a low response to RCE alone which the authors attributed in part to the severity of constipation in the cohort. It is unclear the degree of compliance with the treatment protocol which was done in the home setting. There was a prior open-label study with NJ FMT which improved constipation in half of participants.
My take: Modulating the microbiome can have beneficial effects on stool frequency. This can be through diet and possibly FMT in severe cases of constipation. The availability of capsules could make this type of therapy easier but perhaps less palatable. Even if FMT proves to be a useful treatment, the optimal treatment regimen is not clear.
According to the Centers for Disease Control and Prevention, alcohol consumption is the third-leading preventable cause of cancer in the United States, after tobacco and obesity. And according to the report released by Murthy’s office, it increases the risk for at least seven types of cancer…
In a post on X, Murthy said alcohol contributes to about 100,000 cancer cases and 20,000 cancer deaths annually in the U.S., a number greater than the 13,500 alcohol-related traffic accidents each year.
Murthy is calling on Congress to act to update the labels to include an increased risk of the following cancers linked to alcohol consumption:
Breast
Colon
Throat
Liver
Voice box
Esophagus
Mouth
From NY Times:
While most cancer deaths occur at drinking levels that exceed the current recommended dietary guidelines, the risk for cancers of the breast, the mouth and the throat may rise with consumption of as little as one drink a day, or even less, Dr. Murthy said on Friday.
Overall, one of every six breast cancer cases is attributable to alcohol consumption, Dr. Murthy said. …
The World Health Organization says there is no safe limit for alcohol consumption…The most widely accepted theory is that inside the body, alcohol breaks down into acetaldehyde, a metabolite that binds to DNA and damages it, allowing a cell to start growing uncontrollably and creating a malignant tumor.
My take: It is surprising that alcohol is attributed to causing more deaths due to cancer than due to motor vehicle accidents.
First of all: Bilberries are similar to blueberries, but have red inner flesh rather than white flesh.
Background: The authors note that some small studies have shown that anthocyanin-rich extract (ACRE), the bioactive ingredient of bilberries, has been effective for ulcerative colitis (UC)
“ACs have been associated with many protective biological effects, including anti-oxidative, anti-carcinogenic, antimicrobial, and anti-inflammatory properties [17,20,21]. Due to their phenolic structure, ACs exhibit an anti-oxidative capacity in vivo as they scavenge reactive oxygen species (ROS) [20,22], also a classical effect of 5-ASA [23]. After ingestion, ACs largely bypass absorption in the upper gastrointestinal tract, reaching the colon intact, where they are metabolized by microbiota through deglycosylation and further degraded into vanillic, protocatechuic, p-coumaric, gallic, and syringic acids (i.e., phenolic acids) [24]. ACs interrupt the pro-inflammatory signaling and are inhibitors of 5-lipoxygenase, a key enzyme implicated in the arachidonic acid pathway for the biosynthesis of active leukotrienes.”
Methods: A multi-center, randomized, placebo-controlled, double-blind study with a parallel group was conducted. Due to COVID-19’s effect on study enrollment, only 34 patients were randomized and only Eighteen ACRE and eight placebo patients could be analyzed (per protocol set)
Key finding:
Half (9/18) of ACRE patients and 3/8 of placebo patients responded clinically (p = 0.278). An improvement in the Mayo score was observed in the ACRE arm (77.8% vs. 62.5% placebo).
Fecal calprotectin (FC) dropped from 1049 ± 1139 to 557 ± 756 μg/g for ACRE but not for the placebo group (947 ± 1039 to 1040 ± 1179; p = 0.035).
The authors state that the placebo group had an unusually high response and that improved FC with ACRE patients indicates efficacy in UC.
Figure 2Figure 3
My take: This is a negative study (despite the secondary finding of improved FC at some timepoints). Importantly, the study did not demonstrate any harms in the ACRE group. It did help me understand more about bilberries!
“There is no consensus regarding optimal management in instances of Orbeez™ ingestion. However, a review of reported cases from 2021 indicated that of 43 cases of bowel obstruction secondary to water bead ingestions, two patients required endoscopic removal and the remaining 41 required surgical enterotomy or intestinal resection. We report a case of successful medical management following ingestion of over 1000 water beads…The patient was placed on a clear liquid diet and received a mineral oil enema with minimal passage of beads. She was then started on sennosides and erythromycin ethylsuccinate to help stimulate expulsion. Stools were closely monitored and revealed passage of greater than 1000 beads over the next 24 h.”
GI and Hepatology News, Open Access: Watershed Moment’: Semaglutide Shown to Be Effective in MASH (November 2024): “At 72 weeks, a 2.4-mg once-weekly subcutaneous dose of semaglutide demonstrated superiority, compared with placebo, for the two primary endpoints: Resolution of steatohepatitis with no worsening of fibrosis and improvement in liver fibrosis with no worsening of steatohepatitis.”
“ESSENCE (NCT04822181) is an ongoing multicenter, phase 3 randomized, double-blind, placebo-controlled outcome trial studying semaglutide for the potential treatment of MASH.” Cohort: N=1200, biopsy-defined MASH and fibrosis, stages F2 and F3…”After initiation, the semaglutide dosage was increased every 4 weeks up to 16 weeks when the full dose (2.4 mg) was reached.”
Key findings:
62.9% of those in the semaglutide group and 34.1% of those in the placebo group reached resolution of steatohepatitis with no worsening of fibrosis.
37% of those in the semaglutide group and 22.5% of those in the placebo group had improvement in liver fibrosis with no worsening of steatohepatitis
Weight loss was also significant, with a 10.5% reduction in the semaglutide group compared with a 2% reduction in the placebo group
No new safety signals were identified
Cardiometabolic risk factors improved as well, with changes in blood pressure measurements, hemoglobin A1c scores, and cholesterol values.
20%-40% improvements in liver enzymes and noninvasive fibrosis markers, such as ELF and vibration-controlled transient elastography liver stiffness.
My take: This expected finding indicates that more GLP-1 agents are likely to be approved for MASH treatment. Survodutide received “U.S. FDA Breakthrough Therapy” in October 2024.
JHW Zhang et al. NEJM 391: 2098-2109. Xalnesiran with or without an Immunomodulator in Chronic Hepatitis B
Background: Xalnesiran, a small interfering RNA molecule that targets a conserved region of the hepatitis B virus (HBV) genome and silences multiple HBV transcripts.
Methods: This was a phase 2, multicenter, randomized, controlled, adaptive, open-label platform trial that included the evaluation of 48 weeks of treatment with xalnesiran at a dose of 100 mg (group 1), xalnesiran at a dose of 200 mg (group 2), xalnesiran at a dose of 200 mg plus 150 mg of ruzotolimod (group 3), xalnesiran at a dose of 200 mg plus 180 μg of pegylated interferon alfa-2a (group 4), or a nucleoside or nucleotide analogue (NA) alone (group 5) in participants with chronic HBV infection who had virologic suppression with NA therapy. The primary efficacy end point was hepatitis B surface antigen (HBsAg) loss (HBsAg level, <0.05 IU per milliliter) at 24 weeks after the end of treatment.
Key findings:
In the associated editorial by Janssen et al. (NEJM 2024;391:2163-2168), the authors note that “nucleoside or nucleotide analogues currently form the backbone of therapy for most patients with chronic HBV infection who have access to treatment…However, treatment must be continued on a long-term basis…Although treatment with nucleoside or nucleotide analogues is associated with a decrease in the severity of liver fibrosis and reduction of liver-related complications, the risk of hepatocellular carcinoma persists at the population level because functional cure is not achieved in most patients.”
“Further data are needed on the durability of the effect achieved with new agents that directly interfere with HBsAg production. The results reported by Hou et al. indicate a risk of relapse, undermining the choice of functional cure as an end point for these agents, at least when assessed relatively early after the withdrawal of therapy…Hou et al. observed that functional cure was achieved only in patients with a baseline HBsAg level of less than 1000 IU per milliliter. Although a substantial proportion of patients have similarly low HBsAg levels, patients with higher HBsAg levels have the greatest risk of adverse liver-related outcomes and thus have the most to gain from new therapies.”
My take: While this study represents important progress, it is not likely to change current treatment strategies in the near-term. Even better than treating HBV is preventing HBV. The best strategy for reducing HBV mortality and morbidity still relies of wide-scale use of the highly effective HBV vaccine.
The authors utilized prospectively collected data from 3 population-based birth cohorts (Danish National Birth Cohort, Norwegian Mother, Father, and Child Cohort, and All Babies in Southeast Sweden). This collectively included nearly 170,000 offspring.
Key findings:
During median follow-up of 16.3–22.3 years, between 1996 and 2021, 543 offspring were diagnosed with IBD
In each country, there was no association between exclusive breastfeeding duration and offspring IBD risk
Discussion:
“In contrast to majority of case-control studies, both cohort studies reported null association between breastfeeding, treated as a binary exposure (any versus no breastfeeding) or by duration, and offspring IBD risk. Similarly, 2 nested case-control studies, leveraging prospectively collected data on early life exposures as part of the population-based Jerusalem Perinatal Study and 2 United Kingdom birth cohorts (the 1946 National Survey of Health & Development and the 1958 National Child Development Study) reported null associations between breastfeeding and IBD risk.22,23 Data from these studies, which are more rigorous in methodology compared with case-control studies, are consistent with findings from our analyses.”
My take: While this study has some limitations inherent in observational data, this study with prospectively-collected data indicates that breastfeeding did not modulate the risk of developing IBD.
Methods: The authors used a cross-sectional study using data from the National Health and Nutrition Examination Survey (2005-2010) and they used two 24-hour dietary recalls and, based on the Nova classification, calculated intakes of ultra-processed foods (UPFs) and minimally-processed foods (MPFs). N=12,716 adults.
Key Findings:
Median UPF and MPF intakes were 26.5% and 66.2% of total grams per day, respectively
Greater UPF consumption (in % gram/d) was associated with higher odds of constipation (adjusted OR [aORQ4 vs Q1], 2.20]
Discussion point: The authors did not find an association with diarrhea. “UPF consumption has been associated with increased risks of GI disorders that can cause chronic diarrhea including IBD and irritable bowel syndrome (IBS). This was thought to be related to alteration of the gut barrier integrity and activation of the immune response in the setting of microbial dysbiosis. The overall effect induces a pro-inflammatory micro-environment in the intestine and alterations in bowel function. However, the amount of UPFs needed to be consumed by individuals such that the risk of diarrhea would be higher is unknown and likely varies between individuals.”
My take: Limiting UPFs and promoting fresh foods/minimally-processed foods is better for our health.
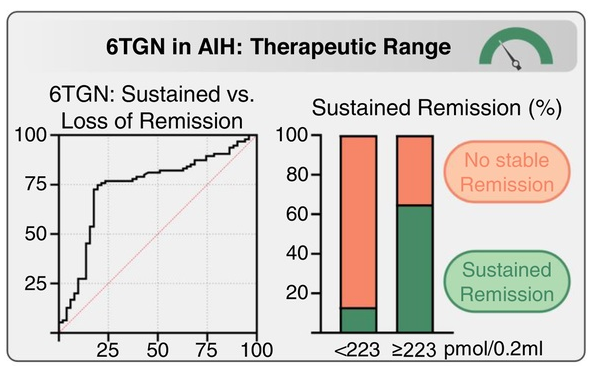
Over 4 years (N = 146), patients with higher average 6TGN levels were associated with those with stable complete biochemical remission (CBR) (260 pmol/0.2 mL) compared to those failing to maintain CBR (181 pmol/0.2 mL; p = 0.0014) or never achieving CBR (153 pmol/0.2 mL; p < 0.0001), with an optimal 6TGN cutoff of ≥223 pmol/0.2 mL
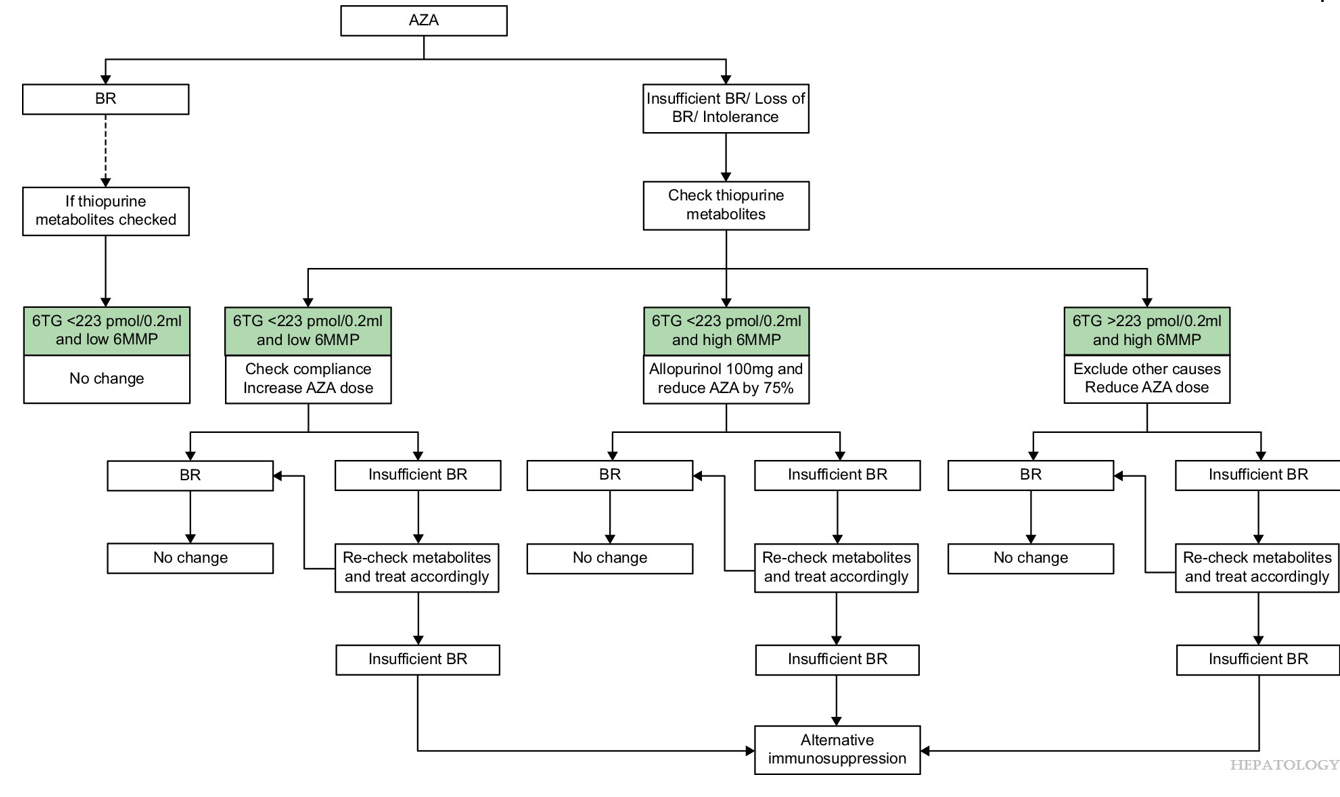
Adding allopurinol to thiopurines in difficult-to-treat patients (N = 36) raised 6TGN (168→321 pmol/0.2 mL; p < 0.0001) and lowered 6MMP (2125→184 pmol/0.2 mL; p < 0.0001), resulting in improved transaminases in all patients and long-term CBR in 75%.
Limitation: most of the 337 patients did NOT have sequential azathioprine metabolite monitoring. This could indicate that the 146 patients with sequential monitoring could have a selection bias favoring patients with a more aggressive disease course. Thus, the proposed 6-TGN level of 223 may not be applicable for all patients.
From editorial:
“In this issue of Hepatology, “Weltzsch et al1 conducted a multicenter study on the metabolic monitoring of thiopurines in AIH. The authors defined an optimal cutoff of ≥223 pmol/0.2 mL average 6TG level to maintain long-term biochemical remission (BR). Notably, 66% of patients with 6TG levels above this cutoff sustained BR rates.
Allopurinol shifts the thiopurine metabolism toward 6TG production, allowing thiopurine dose reduction to 25%–30%, which improves efficacy and tolerability. (The 100 mg dose of allopurinol had more favorable 6MMP/6TG ratio).
However, they note that in a prior study (J Hepatol 2021; 75: 324-32), “patients with subtherapeutic 6TG levels (75–225) achieved similar BR rates (75% vs. 81%, p = 0.589) to those with therapeutic levels (225–450), while experiencing significantly fewer adverse drug reactions (44% vs. 86%, p = 0.0002).”
Proposed Algorithm
My take: This study shows in patients who have not achieved a biochemical remission, optimization of azathioprine dosing with metabolite monitoring improves biochemical remission. In those with low 6TG and low 6MMP, increasing the azathioprine should be considered. In those with low 6TG and high 6MMP, reducing azathioprine and adding allopurinol should be considered.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.