This blog entry has abbreviated/summarized the presentations. Though not intentional, some important material is likely to have been omitted; in addition, transcription errors are possible as well.
Link: PG Course Syllabus – FINAL (entire syllabus)
The speakers reviewed a lot of IBD material (both at the postgraduate course and at the meeting); much of it has been has been covered in previous blog posts:
Early Onset Inflammatory Bowel Disease –Scott Snapper (Boston Children’s Hospital) pg 170 in Syllabus
- If one has a 1st degree relative with Crohn’s disease: 26-fold increased risk for IBD compared with 8-fold increased risk if 1st degree relative has ulcerative colitis
- 30% of children have one or more family members with IBD
- Concordance rate much greater in monozygotic vs dizygotic twins: 10-15% in UC and 25-30% in Crohn’s with monozygotic
Infantile IBD (age <2 years)
- Often isolated colonic disease
- Severe course – refractory to multiple immunosuppressant medications, often requiring surgery, occasionally fatal
- > 40 % with one or more family members with IBD
- 25% with infantile IBD have this as their first manifestation of underlying immunodeficiency (pg 174): IPEX, CGD, NEMO, Wiscott-Aldrich, XIAP, common variable immunodeficiency
- NEOPICS: interNational Early Onset Pediatric IBD Cohort Study. Expanded to 80 Centers (250 scientists) on 5 continents with access to over 1000 VEO-IBD patients
- IL10 Receptor defect results in infantile onset IBD. Hematopoietic stem cell therapy can be curative. Increased risk of B-cell lymphomas.
- NCF2 variant (NADPH Oxidase Gene) found in 4% of (n=11/268)
- TTC7A mutations (identified by whole exome sequencing) cause apoptotic enterocolitis, intestinal atresias, and SCID (severe combined immunodeficiency) –may not benefit by stem cell transplantation
- Immune workup for VEO-IBD: immunoglobulins, DHR for CGD, lymphocyte subsets. If negative, further genetic testing (candidate gene testing &/or exome sequencing)
Surgery in Crohn’s Disease –Jason Frischer (Cincinnati Children’s)
- 28% of CD patients need surgery within 10 years of CD diagnosis; 5.7% within one year.
- Reviewed principles: conserve bowel, reserved for complications/does not cure Crohn’s disease, strictures can be treated without resection.
Perioperative care
- Preop-“no answer with regard to biologics,” steroids are detrimental (goal <20 mg of prednisone). Biologics may increase risk of infections (could be related to specific level) but this is unclear.
- Postop: thromboprophylaxis
Surgical problems (JPGN 2013; 57: 394 NASPGHAN Guidelines): Abscess, Fistula, Stricture
- Abscess: percutaneously drain abscess if >2 cm and can remove drain when having less than 10 mL/day. Surgery reserved if refractory to conservative treatment –?timing
- Strictures: steroids to minimize acute inflammation. Stricturolplasty rare in pediatrics –used only in those without fistulas. Most common stricturolplasty: Heineke-Mikulicz.
- In Crohn’s patients at Cincinnati children’s who have undergone ileostomy, long-term only 46% able to have intestinal continuity
Crohn’s and UC ‐ What to do when anti‐TNF isn’t working? –Athos Bousvaros (Boston Children’s) pg 190 in Syllabus
Off-label IBD drugs in children for medically-refractory disease.
Potential Rescue treatments
- Calcineurin inhibitors for UC (eg. tacrolimus, cyclosporine)
- Thalidomide for Crohn disease
- Natalizumab for Crohn disease –>not being used anymore. PML risk
- Vedolizumab for Crohn disease and UC
- Ustekinumab for Crohn disease
- Tofacitinib for UC
Before off-label drugs:
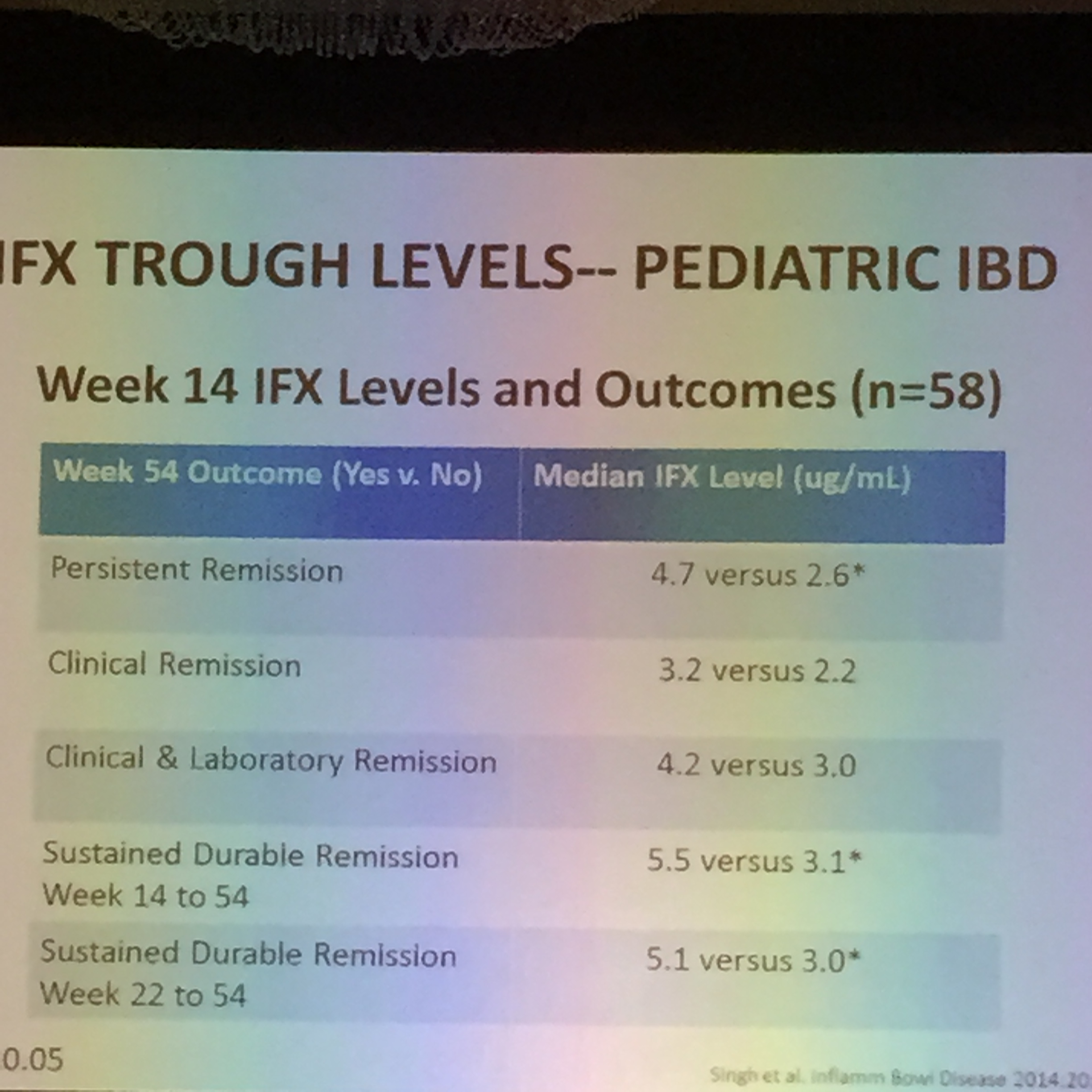
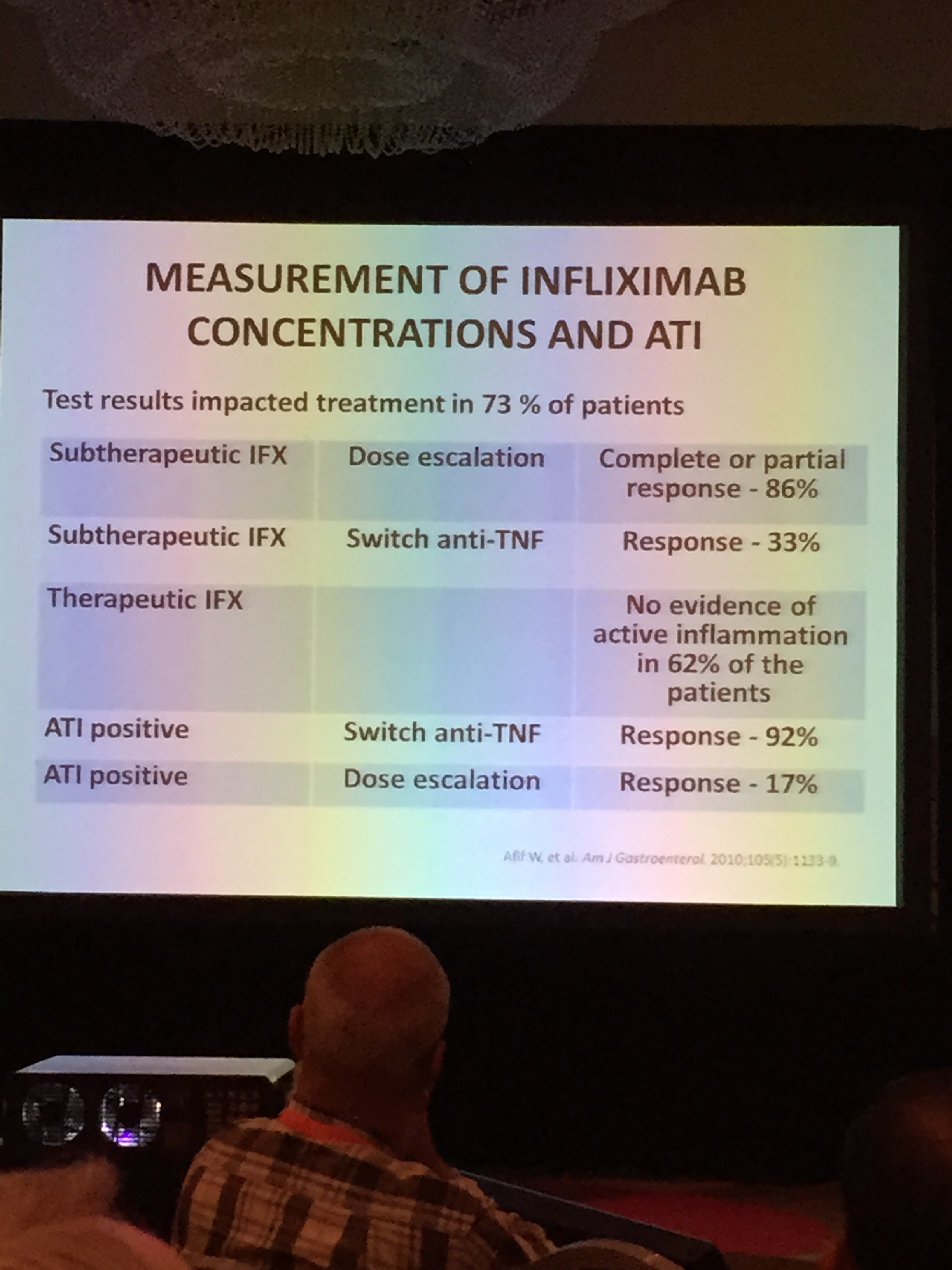
- Optimize TNF: Make sure the diagnosis is right (eg. exclude CGD), Minimize risk of loss of response (combination therapy, optimize dose, scheduled infusions)
- Consider surgery -strictures, ulcerative colitis, limited disease
Data for tacrolimus from Boston. n=46. (Watson et al, IBD Journal 2011). Used most frequently with severe UC.
Data for thalidomide –31 of 49 achieved remission. Lazzerini et al, JAMA. 2013;310(20):2164‐2173. Side effects -birth defects, neuropathy. STEPS program.
Data for vedolizumab. Feagan et al NEJM 2013; 369:699. Remission (in the responders) for ulcerative colitis at 52 weeks:
- 45% of patients getting vedolizumab monthly
- 42% of patients getting it every other month
- 16% of patients randomized to placebo
For Crohns’ disease , Vedolizumab also works in Crohn’s disease, but it takes time (Sands et al: Gastroenterology 2014 147:618‐627)
Off-label does not equate to experimental! pg 199:
FDA Statement: The FD&C Act does not, however, limit the manner in which a physician may use an approved drug. Once a product has been approved for marketing, a physician may prescribe it for uses or in treatment regimens or patient populations that are not included in approved labeling. Such “unapproved” or, more precisely, “unlabeled” uses may be appropriate and rational in certain circumstances, and may, in fact, reflect approaches to drug therapy that have been extensively reported in medical literature.
“Luminitis:” When Inflammation is Not IBD (Microscopic Colitides) –Robbyn Sockolow (Weill Cornell Medical School) pg 180 in Syllabus
Microscopic Colitis -pediatric prevalence unknown (JPGN 2013;57:557-561). Nonbloody diarrhea with normal-appearance grossly.
- Lymphocytic Colitis (>20 intraepithelial lymphocytes/100 colonocytes) -Normal crypt architecture
- Collagenous Colitis -Thick layer (up to 30 micrometers) of collagen in the tissue and increased lymphocytes in colon
Eosinophilic colitis
- At-risk groups? Infants & post-transplant patients (tacrolimus trigger?) (Saeed et al Pediatr Transplantation 2006: 10: 730–735)
- Associated with food allergy, IBD, autoimmune diseases
- Elevated serum IgE.