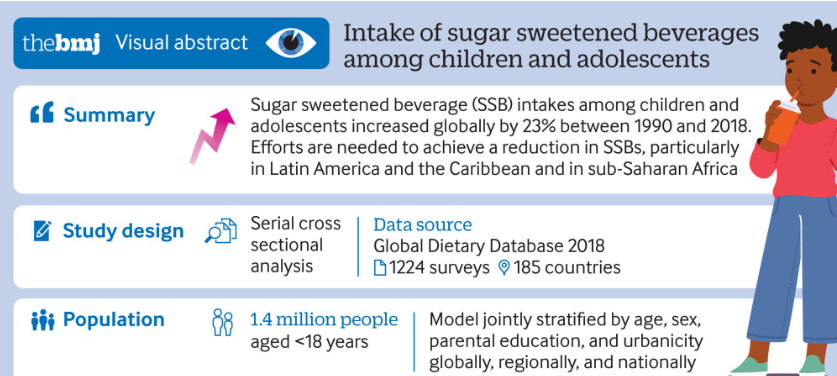
Intakes of SSBs among children and adolescents aged 3-19 years in 185 countries increased by 23% (0.68 servings/week (0.54 to 0.85)) from 1990 to 2018, parallel to the rise in prevalence of obesity among this population globally
High income countries experienced an overall decrease in intakes of SSBs from 2005 to 2018. This might be explained by the increasing scientific and public health attention on the harms of SSBs as well as obesity in these nations during this period, which may have led to increased media and public awareness about the harms to health associated with SSBs
National mean intakes of SSBs (standardized 248 g (8 oz) serving/week for this analysis) in children and adolescents aged 3-19 years across 185 countries in 2018. SSBs were defined as any beverage with added sugars and ≥209 kJ (50 kcal) per 237 g serving, including commercial or homemade beverages, soft drinks, energy drinks, fruit drinks, punch, lemonade, and aguas frescas. This definition excludes 100% fruit and vegetable juices, non-caloric artificially sweetened drinks, and sweetened milk
My take: Despite the knowledge that sugary beverages are detrimental, consumption continues to increase.
16 programs met the criteria for inclusion. None of these programs were in the Western U.S. Among feeding programs that were not included, there were 16 programs excluded due to lack of an intensive day program and 1 program excluded as admissions were on hold due to transition in leadership. .
“Results suggest current treatment capacity of <1000 slots per year.”
Estimates place pediatric feeding disorders as between 1 in 23 and 1 in 37 children under the age of 5 years. Thus, if 5% needed intensive care, this would equate to ~45,000 children under age 5 yrs. This estimate does not include children >5 yrs.
The discrepancy in need (~45,000) and availability (~1000) explains why wait times can be 12 months or longer.
My take: There is a huge mismatch between supply of intensive feeding therapy programs and demand. The potential barriers include training of sufficient numbers of qualified professionals, institutional support, and reimbursement,
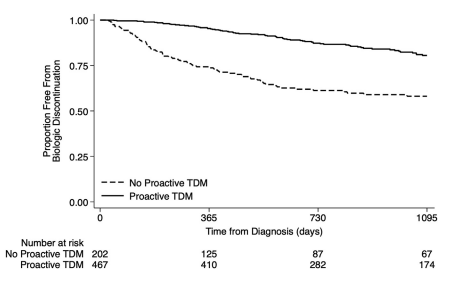
S Ali et al. Clinical Gastroenterology and Hepatology, Volume 22, Issue 10, 2075 – 2083.e1. Characterization of Biologic Discontinuation Among Pediatric Patients With Crohn’s Disease
Methods: Prospective ImproveCareNow registry data (n=823, from 7 centers) were supplemented with medical record abstraction.
Treatment/Monitoring:
86% started biologics (78% infliximab, 21% adalimumab, <1% others)
Twenty-six percent used concomitant immunomodulators for ≥12 months
Most (85%) measured TDM including 47% induction, 69% proactive, and 24% reactive
Key findings:
Twenty-nine percent discontinued their first biologic after median 793 days because of inefficacy (34%), anti-drug antibodies (8%), adverse events (8%), or non-adherence (12%)
Proactive TDM and concomitant immunomodulators were associated with 60% and 32% reduced biologic discontinuation
Half of patients discontinued biologics without trial of high-dose therapy and 14% without any evaluation
Among patients started with infliximab therapy, 62% of patients started at a dose of <6 mg/kg, 18% stared at a dose >8 mg/kg. 67% of patients underwent dose escalation. This is agreement with other studies indicating that as many as 80% of children need doses in excess of ‘standard’ dosing (5 mg/kg every 8 weeks)
In patients with anti-TNF medication inefficacy with TDM availability, 36% had infliximab or adalimumab levels below 5 mcg/mL. and 20% had levels between 6-8 mcg/mL.
Among patients who discontinued anti-TNF medications, 60% had serum trough levels less than 10 mcg/mL.
The rate of biologic durability was lower for those (n=61) receiving a 2nd biologic who had rates of remaining on agent of 56% at 1 yr, 28% at 2 yrs, and 10% at 4 yrs. In contrast, the first biologic had durability of 90% at 1 year, 79% at 2 years, and 66% at 4 yrs.
My take: This study strongly supports the use of proactive therapeutic drug monitoring. In addition, the authors make a compelling argument to optimize a therapy and evaluate carefully before switching to a new medication/biologic. Finally, the use of concomitant immunomodulators can improve medication durability; it is particularly important if needing to switch from one anti-TNF agent to another due to anti-drug antibodies.
“The absorbent polymer beads are often marketed as colorful, slimy, sensory items for kids to play with. They can be as small as a stud earring — little enough to swallow — but grow to the size of a marble or even a golf ball when immersed in water. Once inside a child’s body, they can cause gastrointestinal blockages. The CPSC (Consumer Product Safety Commission) recorded nearly 7,000 water bead-related ingestion injuries in emergency rooms between 2018 and 2022.”
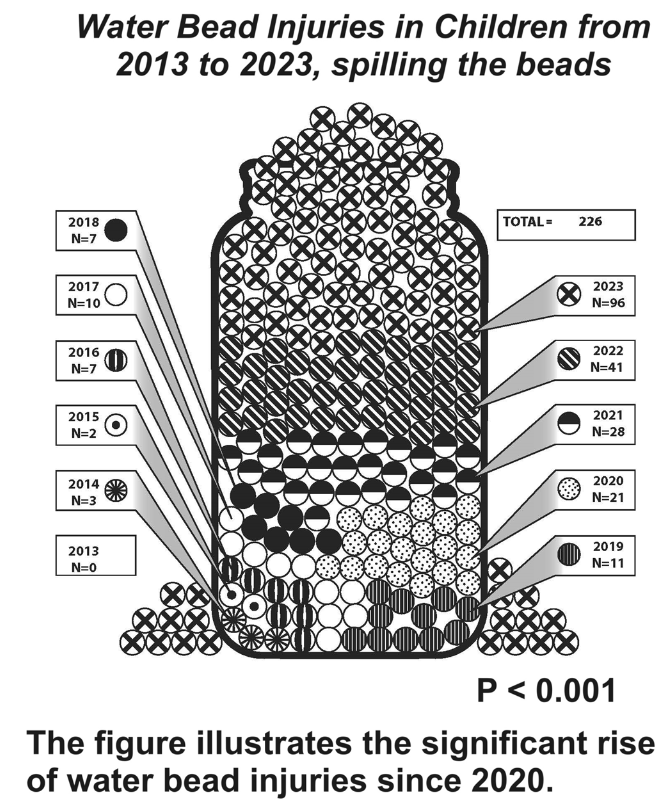
EA Pasman, MA Khan, NT Kolasinski, PT Reeves. JPGN 2024;79:752–757. Water bead injuries by children presenting to emergency departments 2013−2023: An expanding issue
CPSC issued a recall of more than 50,000 Chuckle & Roar Water Beads Activity Kits in 2023 after a 10-month-old child reportedly swallowed one of the water beads and died. (Ref: AAP News (American Academy of Pediatrics). Water bead toy kits recalled following death of 10-month-old child. Accessed Sept 21, 2024)
Methods: The authors used the National Electronic Injury Surveillance System (NEISS) to identify water bead injuries from 2013 to 2023. The nationally representative NEISS database catalogs ED encounters for injuries related to consumer products over a nationwide census and captures 500,000 injury-related encounters annually. The authors used more stringent criteria than CPSC; thus the numbers of injuries from water beads in their study are less than those reported by CPSC.
Key findings:
Children under age 2 years comprised 29% of injuries.
There was a significant uptrend in water bead injury frequency after 2020.
Discussion: Published NASPGHAN recommendations include “‘urgent’ endoscopy (<24 h from presentation, following usual NPO guidelines) for any absorptive object ingested and found to be in the stomach or small bowel. The report recommends emergent upper endoscopy for any absorptive object impacted in the esophagus causing sialorrhea.”
My take: The database captures only a fraction of these ingestions. These objects, even if they do not cause acute injury, could pose long-term harms due to potential carcinogenicity.
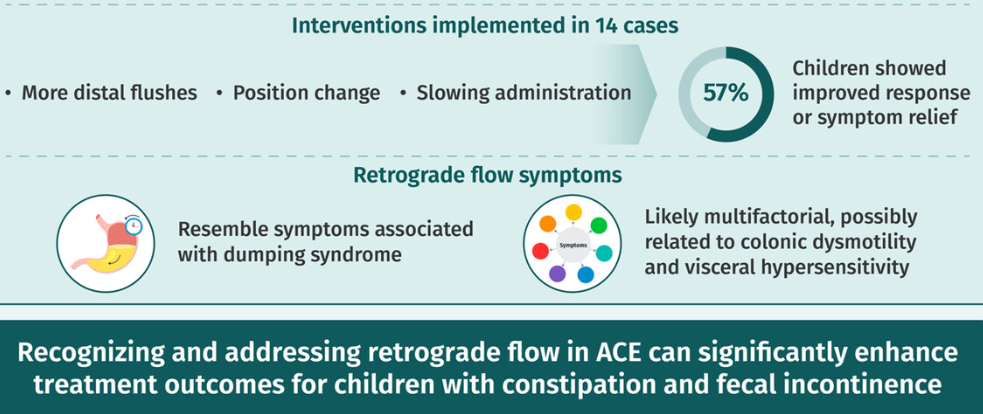
H Pearlstein et al. JPGN 2024;79:519–524. Significance of retrograde flow with antegrade continence enemas in children with fecal incontinence and constipation
Key findings:
Fifty-nine (36%) antegrade contrast studies showed retrograde flow: 28/59 children (48%) were not responding adequately and 21/59 (36%) had symptoms with ACE.
Children with retrograde flow were more likely to have symptoms with ACE than those without (36% vs. 15%, p < 0.01).
The authors hypothesize that symptoms, including nausea, abdominal pain, and vomiting, related to antegrade enemas are potentially similar to those experienced by patients with dumping syndrome related to the osmolar content of the flush and subsequent fluid shifts under hormonal and autonomic control.
My take: Our motility team follow most of our patients with ACEs. This study helps provide a better explanation why some children do not do well with ACEs and potential interventions.
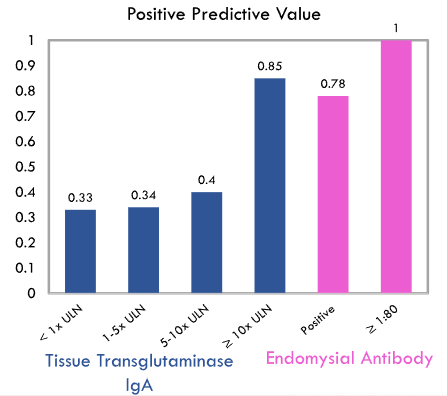
This was a retrospective single-center study with 123 patients -60% had biopsy-proven celiac disease (CD).
Key findings:
Higher titers were more likely to be associated with CD. The degree of TTG IgA elevation in patients with T1DM is correlated with the risk of CD; for every 10‐fold increase in TTG IgA, there is a 4.7× increased risk of celiac diagnosis.
However, even with TTG IgA >10 x ULN, only 85% had CD.
My take: Currently, the non-biopsy approach for CD diagnosis should not be used in patients with type 1 diabetes mellitus.
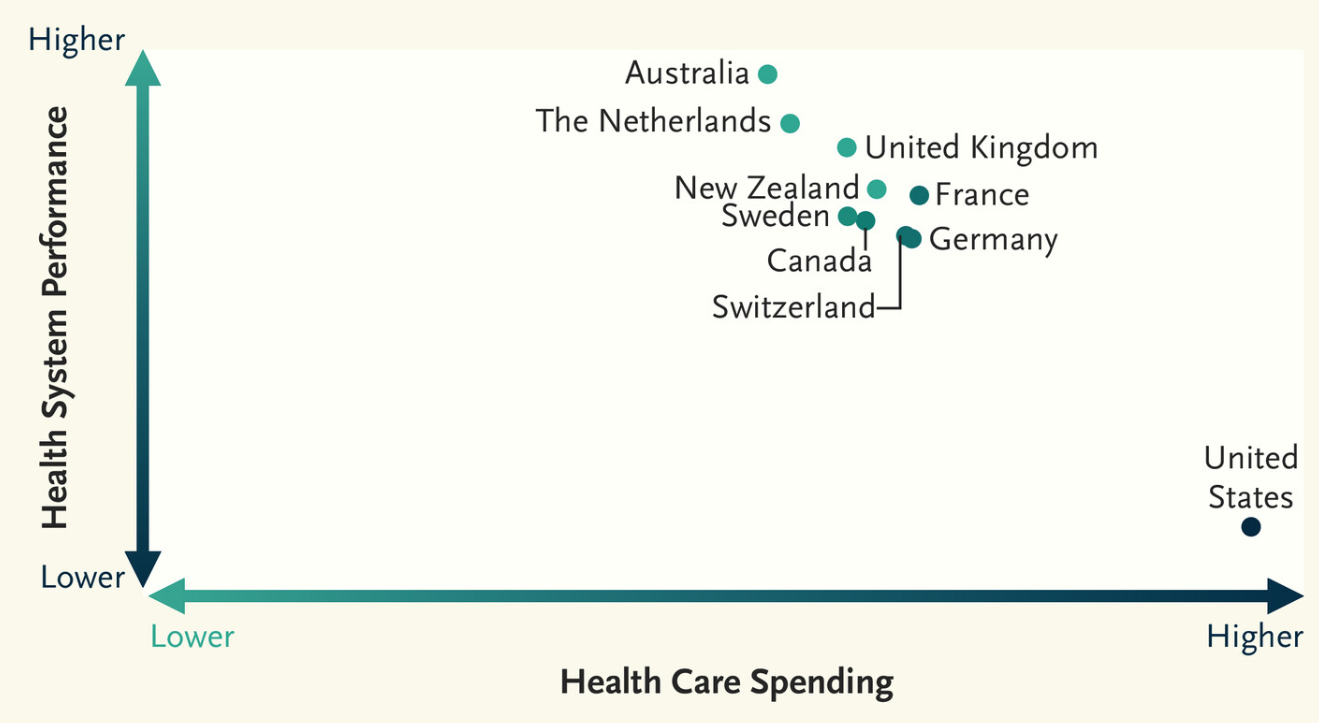
D Blumenthal et al; NEJM 2024;DOI: 10.1056/NEJMp241085. The Failing U.S. Health System
This article succinctly explains why the U.S. health system spends a lot and has the worst performance of similar countries.
Some excerpts:
“In Mirror, Mirror 2024, the Commonwealth Fund’s eighth report since 2004 comparing the health systems of 10 high-income countries…The United States has the lowest life expectancy among the 10 countries we studied, 4 years less than the 10-country average.”
“It also ranks last on measures of preventable mortality and “treatable mortality”…These measures capture deaths that could have been averted by means of preventive services or timely and effective treatment, such as deaths from hypertension, diabetes, cerebrovascular disease, ischemic heart disease, or renal failure. The United States had the highest excess mortality attributable to Covid-19 among people younger than 75 years of age in 2021. It also has the highest rate among the 10 countries of death from self-harm, which includes deaths by suicide, and the highest rate — by orders of magnitude — of death from assault, which includes deaths caused by gun violence.”
“The United States ranks last on measures of access to care and equity of care…Another contributor to access barriers is inadequate coverage among insured Americans because of high deductibles and copayments.”
” The Affordable Care Act and related policies reduced the proportion of uninsured people to its current level of 7 to 8%. But 26 million Americans still lack insurance.”
“Providing insurance, however, will not be sufficient. The U.S. health care delivery system has profound problems … One such problem is the country’s worsening shortage of primary care clinicians”
” the high prices charged by U.S. health care facilities and professionals, which far exceed prices in other health systems.3 … One of the reasons health care organizations are able to charge such high prices is that they have obtained increasing economic power in local markets as a result of consolidation — both horizontal consolidation among hospitals and vertical consolidation, which involves large organizations acquiring physician practices. The arrival of private equity investors who “roll up” physician practices in local markets and then raise prices has also contributed to the escalation of U.S. health care costs.4“
“The United States lags behind comparator countries when it comes to addressing the social determinants of health, such as poverty, homelessness, inequality, and hunger.”
My take (borrowed from authors): “What is the future of a country that allows an untold number of its people to suffer and die unnecessarily because of a lack of access to basic health services, inadequate public health measures, and a tattered social safety net?”
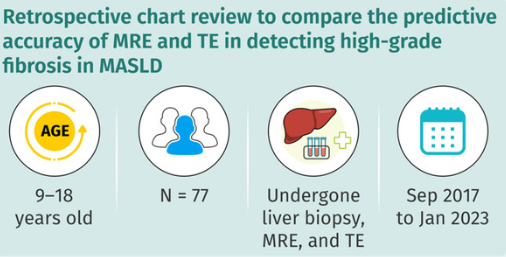
TE and MRE did not have high correlation with liver biopsy in the detection of high-grade fibrosis
Fibrosis was identified in 90% of liver biopsies with bridging fibrosis in 15 (19%) and cirrhosis in 1 (1%)
AUROC curves of MRE and TE for detection of high-grade fibrosis were 0.817 and 0.750, respectively, and not significantly different.
The authors note that previous adults studies suggest that MRE is more accurate in the identification of liver fibrosis than TE (MRE detected ≥ F1 fibrosis with an AUROC of 0.82, while TE detected fibrosis with an AUROC of 0.67).20
My take: Trying to identify accurate non-invasive testing is crucial to help identify patients most in need of treatment and for limiting costs.
Using a nationally representative database spanning the years 2006-2021 with 1412 recipients, Lieber et al describe the patient financial burden after LT. Key findings:
21% had extreme liability > $10K for 1-year post-LT care
69% paid between $1 and 10K, with 48% having liability >$5K in the initial year following LT
Medication costs comprised ~30% of outpatient financial liability
Potential indirect costs from wages lost were $2,201–$6,073 per person
Ufere et al surveyed 207 adult recipients of liver transplant across 5 US transplant centers. Key finding: Nearly 1 in 4 experienced high financial burden (>/= 10% annual income spent on out-of-pocket costs)
The editorial by Ladner et al. notes that “LT is the only curative treatment for cirrhosis, with a 5-year survival of over 80% and, in most cases, returning patients from a chronic disease state to full physical and mental health.6 However, LT is resource-intensive, associated with an average cost of >$700,000, and is only performed in ~10,000 patients every year due to many barriers, including limited organ supply.7 Hence, this lifesaving therapy is currently provided to less than 1% of the patients affected by cirrhosis.8“
Ladner et al note that the financial burden of cirrhosis, though, is reduced after LT. “Without LT, the best that a patient can anticipate is to continue living with chronic liver disease/cirrhosis, with a baseline out-of-pocket cost of $19,390 per year. In this context, receiving an LT appears to be cost-saving for most (>80%) recipients of LT rather than a financial burden—with only 21% of recipients of LT having out-of-pocket costs >$10,000 during the first year after LT. In fact, the average out-of-pocket costs following LT appear quite similar to the $5,567 costs reported by patients without liver disease.5“
My take: LT is expensive. The financial burden needs to addressed with patients. However, for patients with cirrhosis, LT is usually a good value with lower out-of-pocket costs for 80% of recipients along with better quality of life, and longevity.
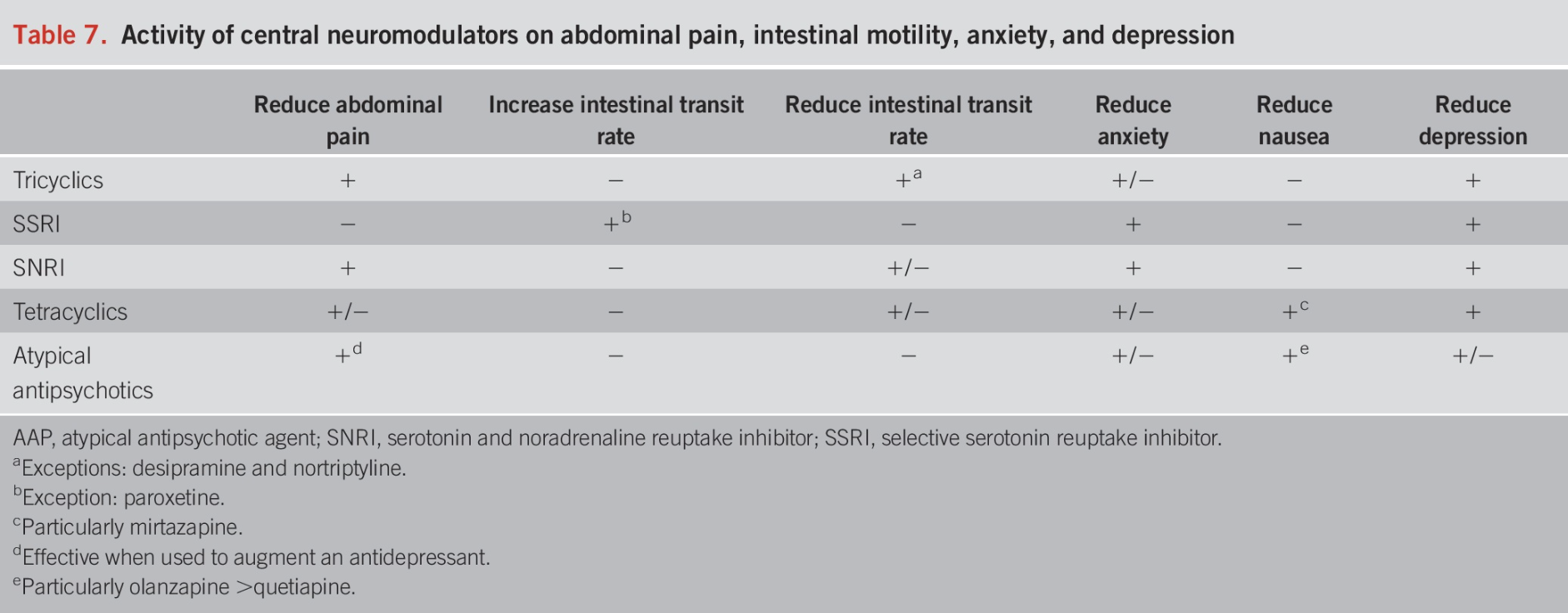
This is a terrific review article. The authors detail the rationale for neuromodulators, strategies for selecting among them, side effects, and dosing.
Background: “IBS is frequently associated with neuropsychiatric disorders such as depression and anxiety, which are considered triggers for the onset of symptoms or occur in response to having them (3). In the Rome Foundation global study that included 54,127 participants, subjects with psychological distress or clinically relevant somatic symptoms were 4.45 times more likely to have 1 or more DGBI than those without psychological distress. The same study reported that those who met specific criteria for bowel disorders presented clinically relevant psychological distress or somatic symptoms in 55.5% of cases (4). In addition, in a meta-analysis that included 7,095 subjects with IBS exclusively, the global prevalence of depression was 36%…Anxiety was present in 44% of patients with IBS….Central neuromodulators act on receptors along the brain-gut axis, so they are useful in treating psychiatric comorbidities, modifying gut motility, improving central downregulation of visceral signals, and enhancing neurogenesis in patients with IBS… Neuromodulator treatment is still considered off-label, many of the recommendations herein are based on expert consensus (6)”
Key points:
“The first-line treatment for pain management in IBS is using tricyclic antidepressants.” Nortriptyline and desipramine are less likely to cause constipation.
“Selective serotonin reuptake inhibitors (SSRIs) are useful when symptoms of anxiety and hypervigilance are dominant but are not helpful for treating abdominal pain….The SSRIs include fluoxetine, fluvoxamine, sertraline, paroxetine, citalopram, and escitalopram. …Sertraline, citalopram, and escitalopram tend to have the fewest pharmacokinetic drug interactions”
“SSRIs are first-line pharmacologic agents for treating anxiety disorders, but they have the potential to induce restlessness and exacerbate anxiety when the drug is initiated. They are typically initiated at half of the usual starting dose to minimize these potential anxiogenic adverse effects. The dose may gradually increase to the regular starting dose after about 1 week… SSRIs should be considered when a significant component of anxiety without pain is present.”
SNRIs: “In addition to showing benefits with depression and painful disorders, SNRIs have shown significant improvement in anxiety.” Thus, they may be useful as monotherapy for patients with pain and anxiety.
Tetracyclics: “The most representative agent of this class is nirtazapine (Table 5). However, their effects seem to be mainly on anxiety, early satiety, nausea, and other symptoms associated with esophageal and gastroduodenal disorders, so their use in IBS is limited.”
“It is important to explain to the patients, …neuromodulators are not necessarily used for the treatment of depression but are a therapeutic alternative in the management of DGBI. It helps to use the term “neuromodulator” instead of “antidepressant” (6,8) It also helps to clarify that these medications can treat pain and other GI symptoms independent of treating depression, and the dosages are often lower than those used for treating major depression. This will preclude any patient concerns that their symptoms are being underestimated or considered to be in their head (6,8).”
Using central neuromodulators for IBS requires long-term treatment. From our experience, 6–12 months of treatment or more are needed to increase the likelihood of remission.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.