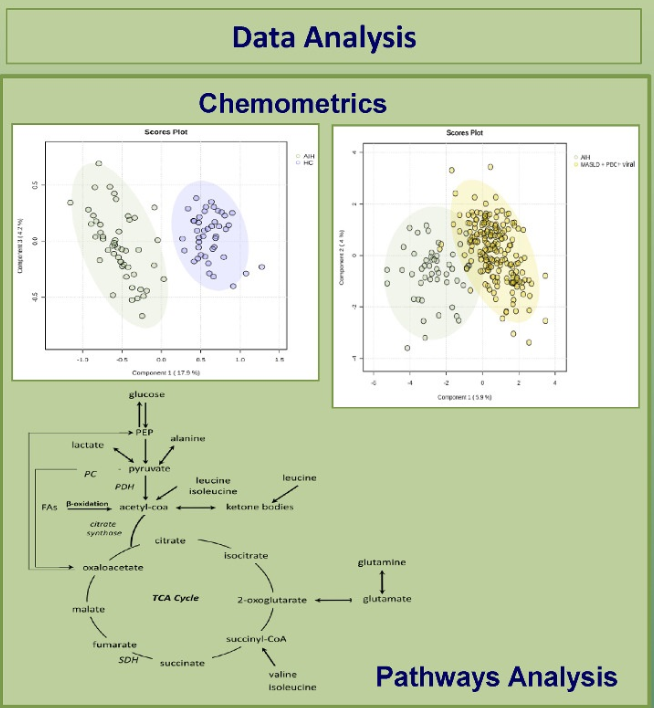
Methods: The authors examined treatment-naive patients with well-established AIH and compared them to healthy controls and those with other liver diseases.
Key Finding:
Fifteen metabolites (out of a total of 52 analyzed) differentiated AIH from disease controls (PBC+chronic viral hepatitis+metabolic dysfunction–associated liver disease) (95% sensitivity and 92% specificity)
In their discussion, the authors review the metabolism of the various metabolites and why they may be altered in AIH. “Our study found that cirrhosis did not seem to affect our results.” In ongoing studies, the authors are trying to determine how these metabolites change with treatment and whether they could be a predictive marker.
My take: Metabolite measurement could be helpful in the diagnosis of AIH as “NMR technology dose not need much sample handling, is highly reproducible, and with low costs.
6-Thioguanine Levels in Autoimmune Hepatitis The associated editorial (pg 2-3, N Kerkar) cautions that while “lower levels are sufficient for maintaining biochemical remission…higher levels, similar to that used in IBD, are required for inducing remission.”
D Turner et al. JPGN 2024; 79:315–324. Ustekinumab in paediatric patients with moderately to severely active Crohn’s disease: UniStar study long-term extension results
Dosing: “Patients were randomised 1:1 and stratified by body weight (<40 or ≥40 kg) to receive a single induction dose of lower- or higher-dose IV ustekinumab (lower dose: 3 mg/kg [<40 kg] and 130 mg [≥40 kg]; higher dose: 9 mg/kg [<40 kg] and 390 mg [≥40 kg]). Doses specified as higher were selected to deliver ustekinumab exposure comparable to a reference adult population with CD.7, 12 At Week 8, patients received a single SC maintenance dose of ustekinumab (2 mg/kg [<40 kg]; 90 mg [≥40 kg]).”
Key findings:
Of the 34 patients who entered the LTE, 25 patients with evaluable data completed Week 48, and 41.2% (14/34) achieved clinical remission at Week 48
Efficacy and PK through 1 year in ustekinumab-treated paediatric patients were comparable to those previously reported in adults. No new safety or immunogenicity signals were reported through 4 years of ustekinumab treatment.
My take (borrowed in part from authors): “Overall, long-term data support the SC dose regimens of 90 mg as maintenance therapy for the treatment of CD for a paediatric population with ≥40 kg body weight. A phase 3 study of ustekinumab (ClinicalTrials.gov Identifier: NCT04673357) is ongoing to further evaluate dose regimens for paediatric patients <40 kg and ≥40 kg.” This type of data is essential to support the use of advanced therapies like ustekinumab until they receive specific regulatory approval for children (often 8-10 years after approval in adults).
Methods: The authors developed an agent-based model (ABM) “simulating the dynamics of HCV transmission and demographic changes from 2006 to 2030, using data from Ontario, Canada.14 Predicted long-term health outcome effects for current HCV policies (status quo) and those following the implementation of various scale-up interventions were compared to the elimination goals set by the WHO.”
Key findings:
Under the current status quo of risk-based screening, we predict the incidence of CHC-induced decompensated cirrhosis, HCC, and liver-related deaths would decrease by 79.4%, 76.1%, and 62.1%, respectively, between 2015 and 2030
However, chronic hepatitis C (CHC) incidence would only decrease by 11.1% (WHO goal by 2030 is a reduction of 80%)
From the editorial:
“According to the study by Tian et al,3 the future incidence of HCV infection will be mainly related to HCV transmission, stressing the fact that harm reduction strategies, in addition to the highest treatment rate, are paramount to reducing the further HCV spread and reinfection risk, especially in marginalized populations. In high‐income countries, HCV treatment rates among people who use drugs remain inadequate due to a lack of simplified HCV testing, scale‐up of harm reduction‐based HCV treatment programs, and numerous additional barriers to HCV services.”
“It is not just a matter of time until high-income countries get rid of HCV infection. The ongoing mass screening campaign in Italy shows that having political will and financial coverage is insufficient to achieve the HCV elimination targets. In high-income countries, encouraging and convincing people to get tested is among the most challenging and underrated.”
My take: The development of highly effective HCV treatments has been a remarkable feat, reducing the rate of death and complications from HCV. Nevertheless, it has not brought about a big improvement in HCV transmission. To achieve this, it looks like a vaccine will be necessary. Until then, our fight against HCV is akin to the ‘rope a dope‘ boxing strategy –we are not getting a knock-out anytime soon against this opponent.
KA Hommel et al. JPGN 2024; 78:1273–1278. Pilot and feasibility of the SMART IBD mobile app to improve self-management in pediatric inflammatory bowel disease
The Self‐Management Assistance with Recommended Treatment (SMART) IBD app –Key findings:
Patients rated the app quality as good and accessed the app adequately overall, with some pages being used often.
Medication adherence increased over the course of the study and was associated with sleep duration, mood, and stool consistency and blood content.
My take: IBD Management apps could be quite helpful, especially for teens and young adults.
S Hsiang et al. Inflammatory Bowel Diseases, Volume 30, Issue 8, August 2024, Pages 1284–1294, https://doi.org/10.1093/ibd/izad166. Safety, Effectiveness, and Treatment Persistence of Subcutaneous Vedolizumab in IBD: A Multicenter Study From the United Kingdom
Methods: IBD patients (n=563) on IV vedolizumab across 11 UK sites agreed to transition to SC injections or otherwise continued IV treatment
Key findings:
Data from 563 patients, demonstrated no differences in disease activity, remission rates, and quality of life between the SC and IV groups at all time points
Drug persistence at week 52 was similar (81.1% vs 81.2%; P = .98)
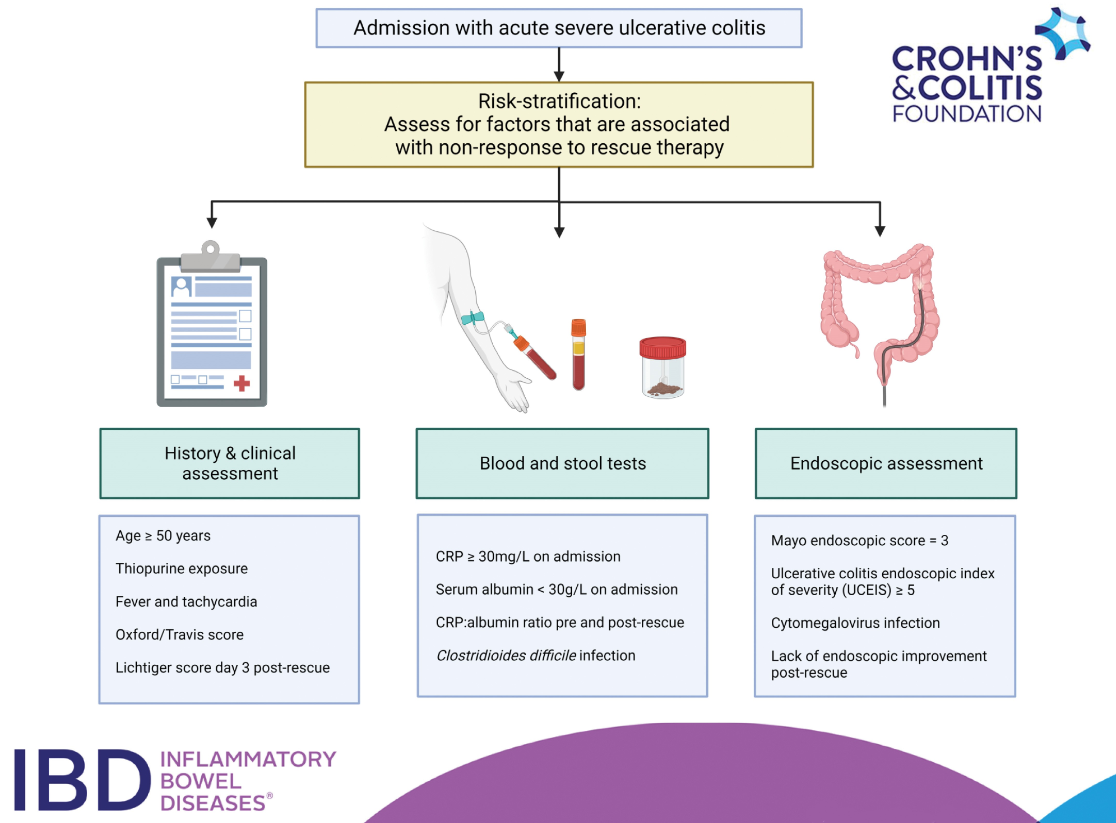
CFD Li Wai Suen, et al. Inflammatory Bowel Diseases, Volume 30, Issue 8, August 2024, Pages 1389–1405, https://doi.org/10.1093/ibd/izad183. Factors Associated With Response to Rescue Therapy in Acute Severe Ulcerative Colitis
This systematic review identified 101 completed studies were eligible for inclusion.
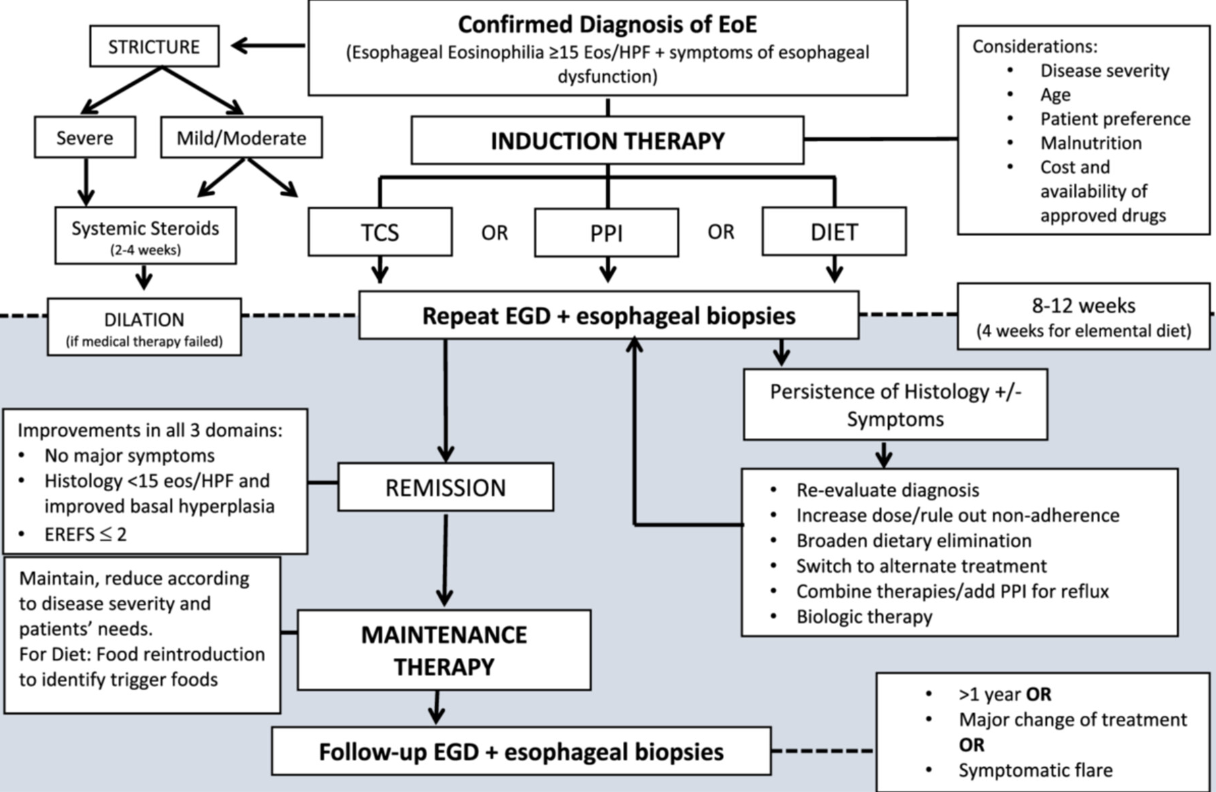
This report makes 52 statements and 44 recommendations. Overall this is a helpful report but there are many statements and recommendations that have NO value for pediatric gastroenterologists (except for those trapped in a cave for the last 10 years). Here are a couple examples of that:
“ESPGHAN EGID WG recommends that pediatricians should be aware of the higher incidence of EoE in relatives.”
“ESPGHAN EGID WG recommends that a high index of suspicion for EoE must be maintained in children with concomitant atopic disease.”
“ESPGHAN EGID WG recommends the peak value of 15 eos/HPF as the cut‐off value in esophageal biopsy specimens, for the histological diagnosis of EoE in an appropriate clinical context”
Some helpful recommendations:
“ESPGHAN EGID WG recommends against using available allergy tests to predict dietary triggers of EoE.” This is not new information but helpful to have clearly stated in guidelines.”
“ESPGHAN EGID WG recommends maintenance therapy to all patients after achieving histological remission” Commentary: “There are no prospective data on the best duration of maintenance therapy in pediatric EoE…[In a large study of adults} sustained untreated combined remission was seen in only 1.3% of patients who discontinued treatment.”
“ESPGHAN EGID WG suggests endoscopic and histological re‐evaluation after 1‐3 years during the maintenance phase in cases of stable clinical remission”
“ESPGHAN EGID WG recommends that dupilumab can be used in selected cases of children over1 year old weighing >15 kg with EoE refractory to conventional treatment and in those with concomitant atopic burden with approved indications for biologics”
“ESPGHAN EGID WG suggests that a short course of systemic steroids be considered as an alternative to dilation in the presence of moderate to severe esophageal strictures with severe symptoms.” “Treatment with short term systemic steroids can significantly reduce the need for mechanical esophageal dilation in moderate to severe strictures associated with pediatric EoE”
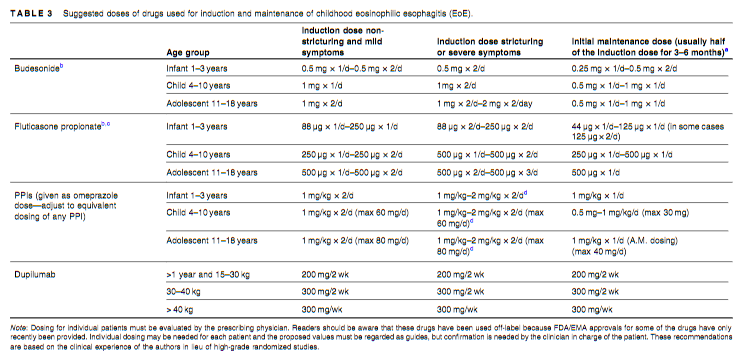
Suggested drug dosing is noted in Table 3 (see below)
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
I signed up for this webinar mainly to hear my partner Jose Garza’s presentation (who presented last), though all the speakers were good. I took a couple screenshots on my phone during the presentations. The webinar is available/archived at NASPGHAN website.
Dr. El-Chammas’ presentation gave a quick review on normal swallowing physiology, modalities for evaluation (eg. VSS, FEES) and showed some cool slides particularly with regard to pharyngeal manometry.
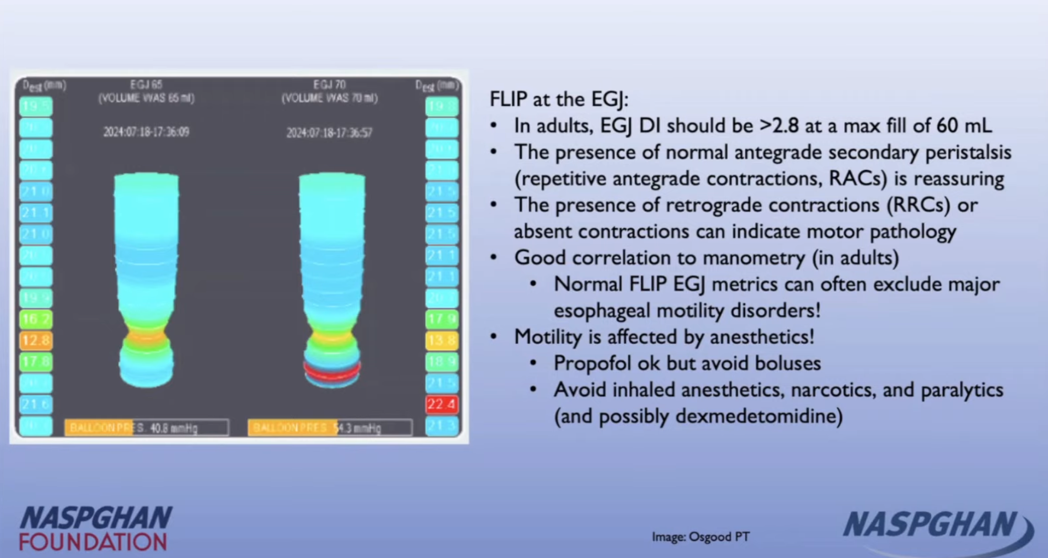
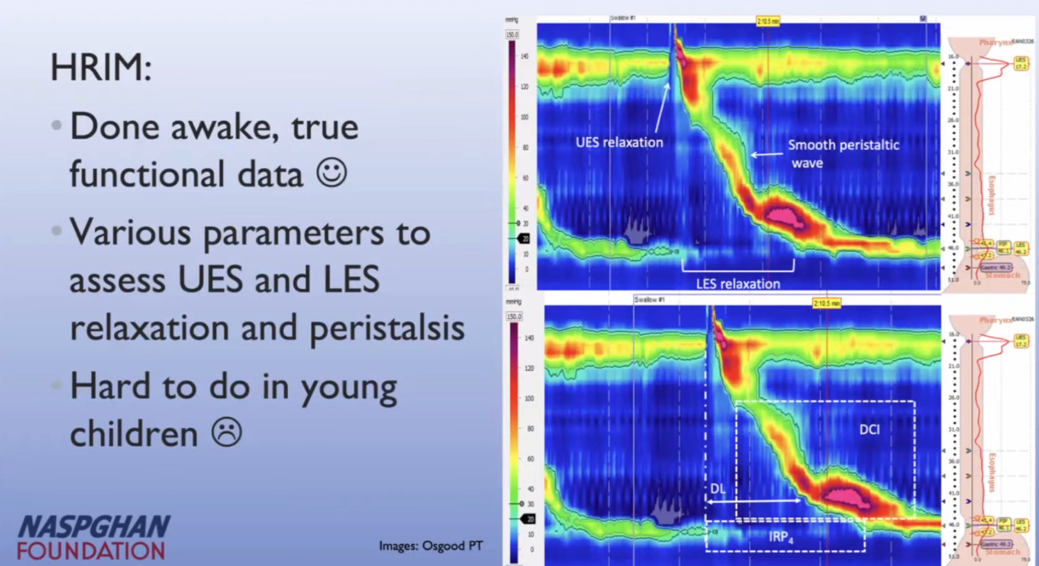
Dr. Osgood reviewed the etiologies/workup for dysphagia including helpful slides on esophagrams, FLIP and manometry.
Manometry typical of Type 2 Achalasia
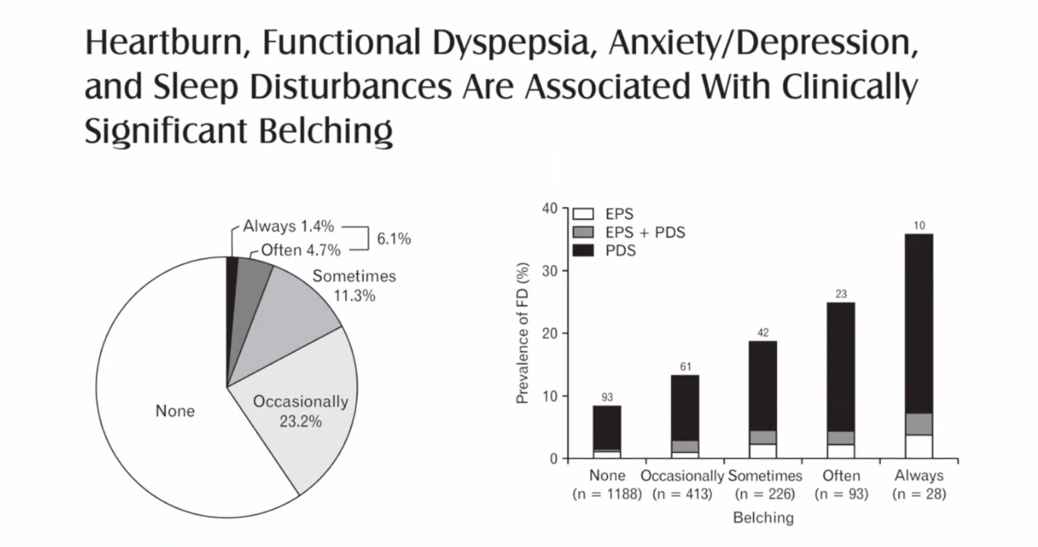
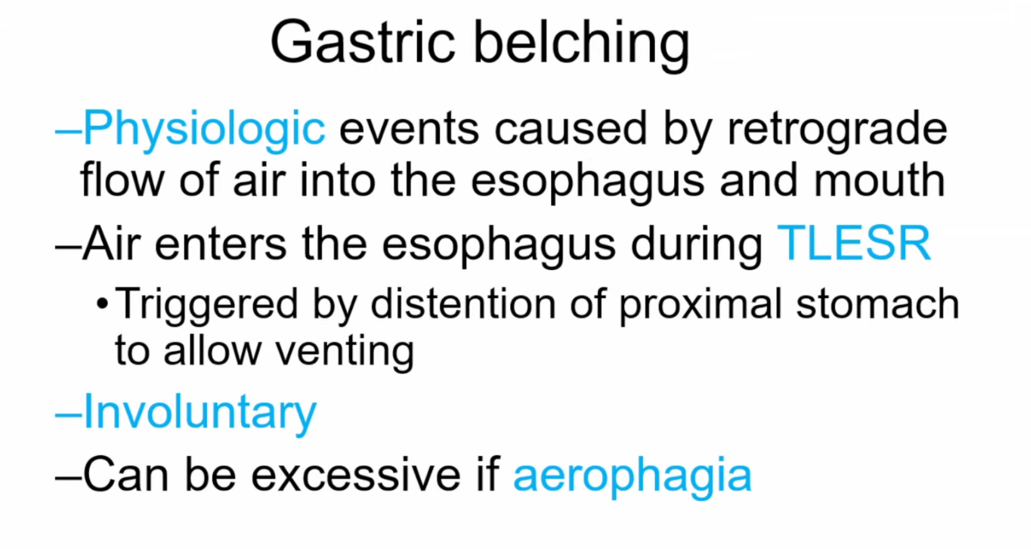
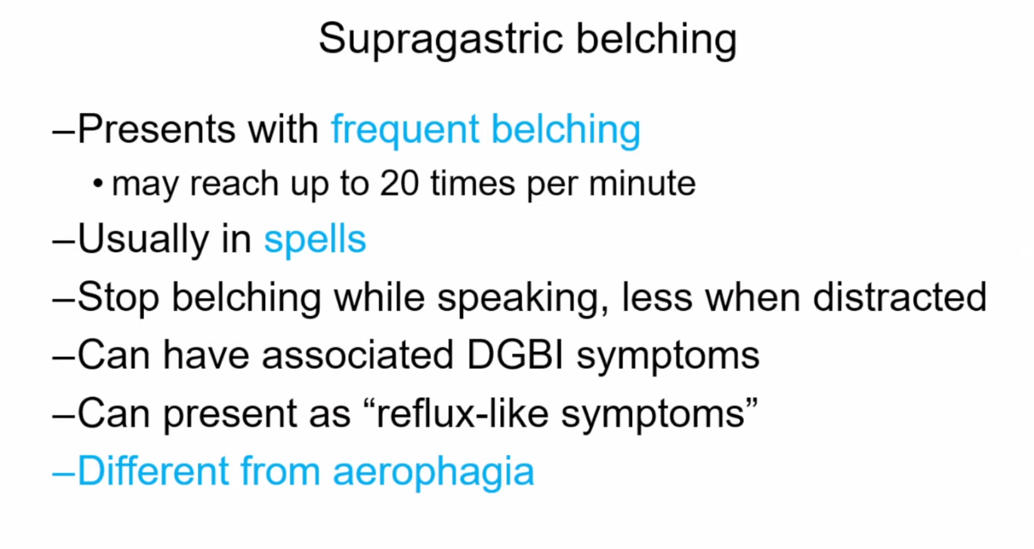
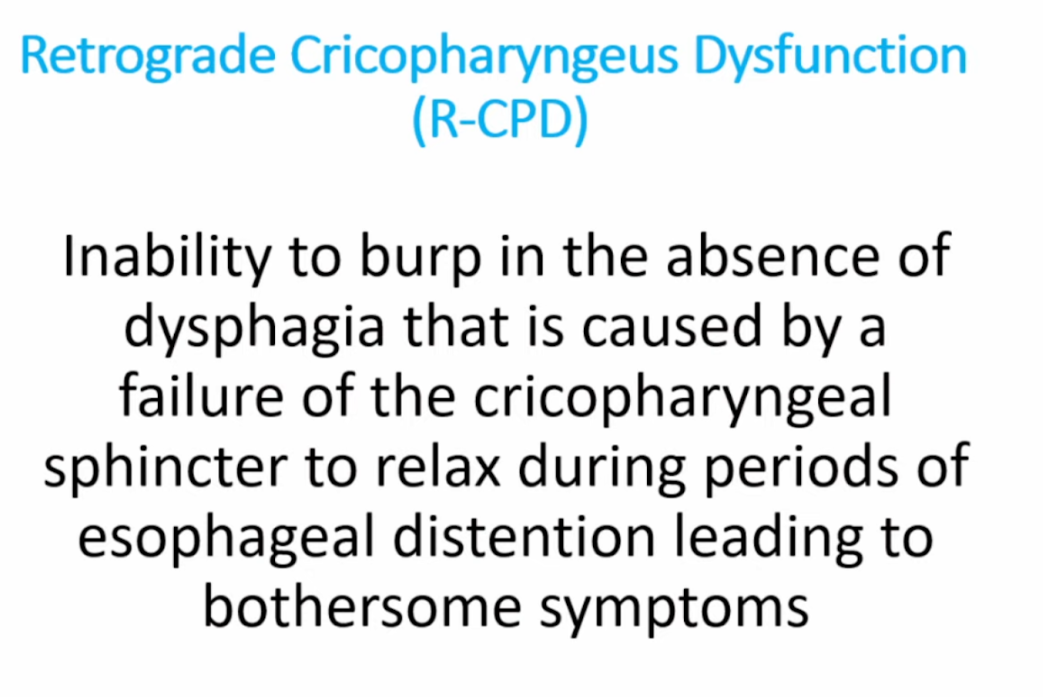
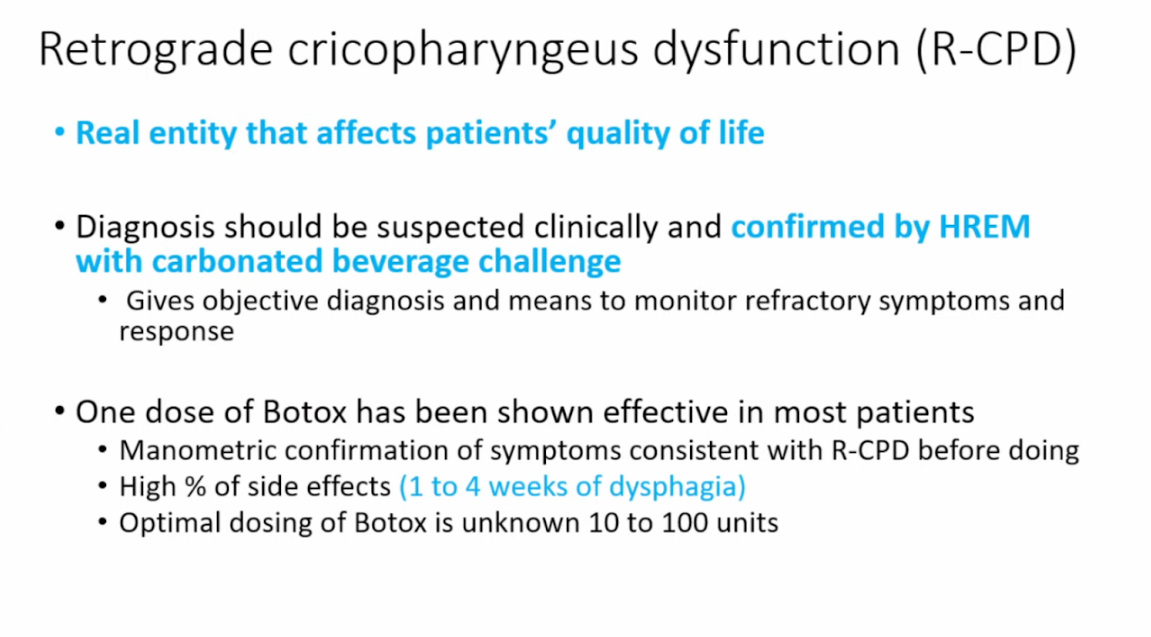
Dr. Garza provided insightful information on gastric vs supragastric belching. Supragastric belching can be treated with diaphragmatic breathing and cognitive behavioral therapy. Supragastric belching has shown poor response to pharmacologic therapy. He also explained the physiology behind the inability to burp.
Important to distinguish reason for belching as this affect managementThis study shows that with gastric belching the air works its way from the stomach up and with supragastric belching air is swallowed and expelled from the esophagus
My take: Our motility colleagues have some cool toys. When the treatments are as good as the toys, being a motility specialist will be even more fun.
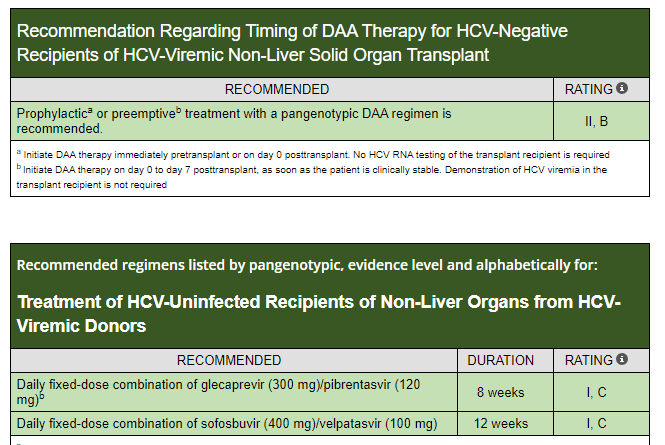
A recent report in Gastroenterology and HepatologyNews (July 2024: Shortened Protocol Can Prevent Infection in Recipients of HCV+ Organs) highlighted the recommended use of 1 week empiric treatment to prevent the development of hepatitis C in transplant recipients of HCV+ organs.
The cost for a one week course of “the Toronto Protocol” which includes glecaprevir-pibrentasvir along with ezetimbe is ~$2800. This is much less than a full course which likely would cost ~$30,000. Ezetimbe, cholesterol-lowering agent, has the ability to prevent HCV from entering cells.
For liver transplant recipients of HCV+ donor, a 12 week course of treatment is recommended
SJ Martinez-Dominguez et al. Inflammatory Bowel Diseases, Volume 30, Issue 8, August 2024, Pages 1274–1283, https://doi.org/10.1093/ibd/izad175 Open Acess! Inflammatory Bowel Disease Is an Independent Risk Factor for Metabolic Dysfunction–Associated Steatotic Liver Disease in Lean Individuals
Methods: This was a cross-sectional, case-control study including 300 lean cases with IBD and 80 lean controls without IBD, matched by sex and age (median age ~45 yrs). All participants underwent a liver ultrasound, transient elastography, and laboratory tests. All patients with current or previous use of systemic steroid in the last 2 years were excluded from the analysis
Key Findings:
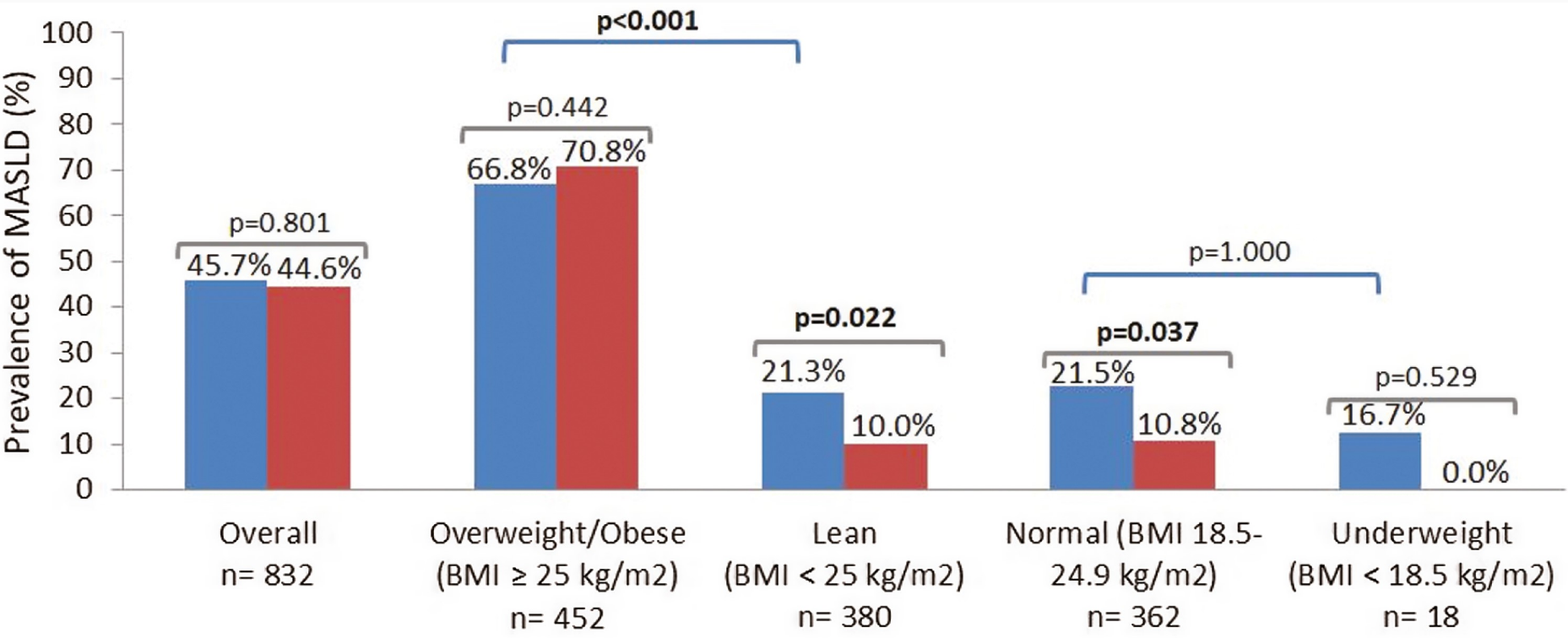
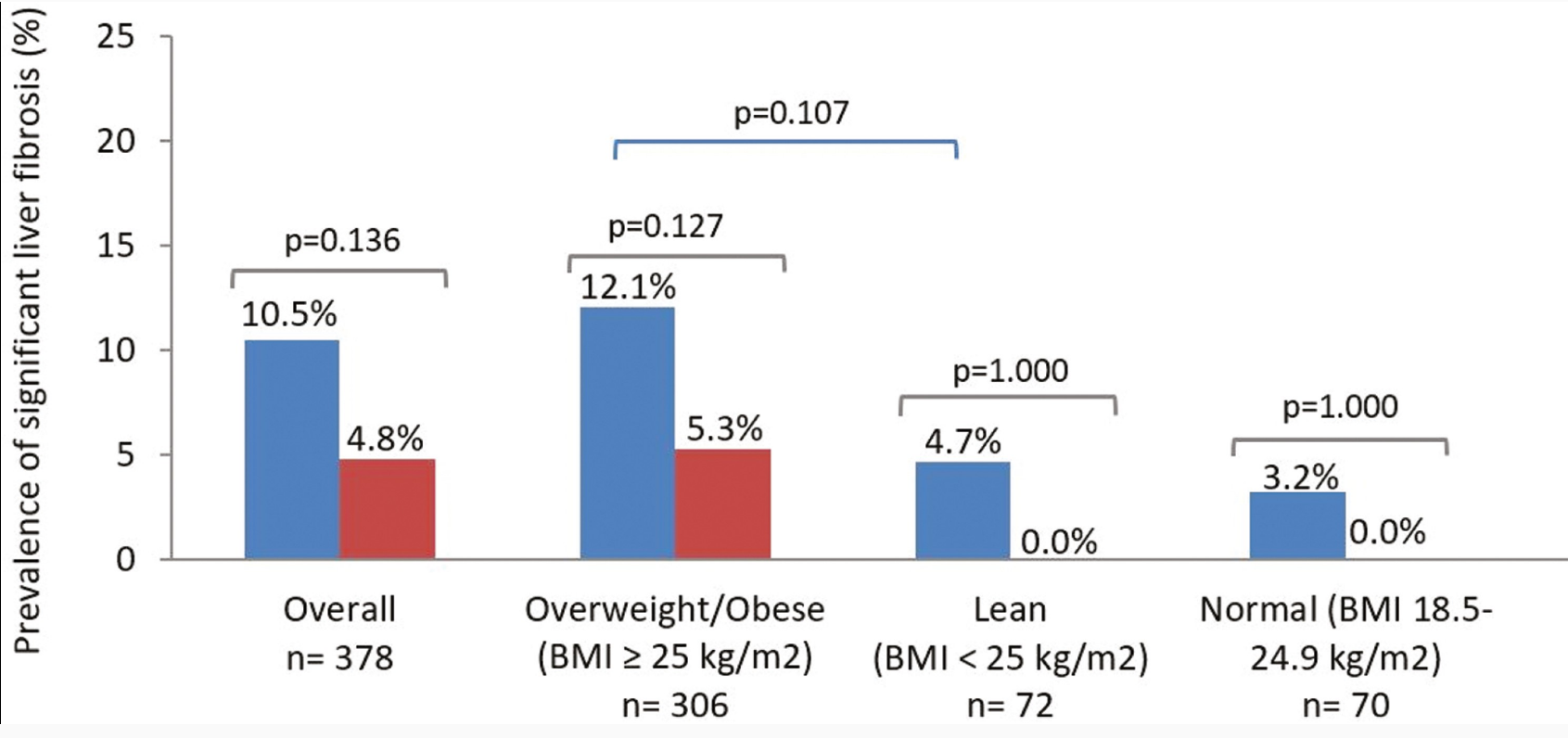
The lean IBD group showed a significantly higher prevalence of MASLD compared with lean non-IBD group (21.3% vs 10%; P = .022), but no differences were observed in the prevalence of significant liver fibrosis (4.7% vs 0.0%; P = 1.000)
No differences were found between the prevalence of MASLD in IBD and non-IBD participants who were overweight/obese (66.8% vs 70.8%; P = .442)
IBD was an independent risk factor for MASLD in lean participants (odds ratio [OR], 2.71) after adjusting for classic metabolic risk factors and prior history of systemic steroid use
Prevalence of metabolic dysfunction–associated steatotic liver disease (MASLD) in cases and controls according to body mass index (BMI) status. Blue bars: cases (inflammatory bowel disease). Red bars: controls (non–inflammatory bowel disease). P values in bold indicate statistical significance (P < .05).
My take: This study suggests that “chronic inflammation could play a role in MASLD development.” Also, this indicates that MASLD could be a reason for elevated LFTs in patients with IBD, even in lean patients.
Methods: Among 1410 adolescents (12–19 years) in NHANES (2017-March, 2020), the controlled attenuation parameter (CAP) of transient elastography (TE) was used to define steatosis and fibrosis (TE ≥ 7.4 kPa). Obesity and alanine aminotransferase (ALT) ≥ 80 U/L were used to identify adolescents qualifying for hepatology referral according to practice guidelines.
Key findings:
At the supplier (EchoSens)-recommended CAP threshold of 240 dB/m, 30.5% of adolescents had steatotic liver disease (SLD) and about 85% of adolescents with NAFLD met criteria for MASLD. At a CAP threshold of 270 dB/m, SLD prevalence was about 16% in adolescents. The other 15% of NAFLD patients do not meet diagnostic criteria MASLD and would receive a diagnosis of cryptogenic SLD or possible MASLD
At higher CAP thresholds, MASLD/NAFLD concordance increased and approached 100%.
Among adolescents with MASLD-fibrosis, only 8.8% had overweight/obese and ALT ≥ 80 U/L. Thus, more than 90% of adolescents in this group would not merit hepatology evaluation based on current guidelines.
My take: This study identifies potential problems with current thresholds for which patients need to be seen by pediatric hepatologists. This will be even more important as effective pharmaceuticals become available.
Y-C Ling et al. JPGN 2024;79:222–228. Performance of Baveno VII criteria for the screening of varices needing treatment in patients with biliary atresia
Methods: This retrospective study enrolled 48 BA patients (23 females and 25 males) who underwent an esophagogastroduodenoscopy (EGD) and transient elastography at a mean age of 11.18 ± 1.48 years. Transient elastography (Fibroscan® 502 Touch; Echosens) was applied for the LSM assessment in all BA patients recruited in this study.
CSPH of Baveno VII criteria was defined as LSM ≥ 25 kPa and excluded patients with LSM < 15 kPa and platelet count ≥150 × 10-9 /L. Subjects with LSM between 20 and 25 kPa and platelets <150 × 10-9 /L or LSM between 15 and 20 kPa and platelets <110 × 10-9/L are also defined as CSPH. (Ref: Baveno VII criteria Ref: M Mendizabal et al. Annals of Hepatology; 2024: 29: 101180. Evolving portal hypertension through Baveno VII recommendations)
Key findings:
The sensitivity and negative predictive value of Baveno VI and Baveno VII criteria for the prediction of varices needing treatment (VNT) in BA patients were both 100% and100%, respectively
In the discussion, the authors note that the utility of the Baveno VII criteria for adults. “The real‐world data showed the CSPH defined by Baveno VII criteria predicts a five‐times increase in the risk of liver decompensation in chronic active liver disease patients.”
My take: This study shows that the combination of LSM and platelet counts using the Baveno VI or VII criteria help select patients with BA who need upper endoscopy to screen for varices needing treatment. These criteria also identify patients needing liver transplantation.
Related blog posts:
Time to Adjust the Knowledge Doubling Curve in Hepatology (2021) The 2nd guidance in this review discusses procedures for bleeding in patients with chronic liver disease. “For Platelets in the setting of cirrhosis: “Given the low risk of bleeding of many common procedures, potential risks of platelet transfusion, lack of evidence that elevating the platelet count reduces bleeding risk, and ability to use effective interventions, including transfusion and hemostasis if bleeding occurs, it is reasonable to perform both low‐ and high‐risk procedures without prophylactically correcting the platelet count...An individualized approach to patients with severe thrombocytopenia before procedures is recommended.” And, ““The INR should not be used to gauge procedural bleeding risk in patients with cirrhosis who are not taking vitamin K antagonists (VKAs)…Measures aimed at reducing the INR are not recommended before procedures in patients with cirrhosis who are not taking VKAs…FFP transfusion before procedures is associated with risks and no proven benefits.”
Channel Islands off California coastView from Griffith Park, Los Angeles
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.