Recently, this blog post reviewed a case presentation of hereditary angioedema which often presents with bouts of severe abdominal pain: “A Swell Diagnosis”
Now, a study has shown how this can be effectively treated with CRISPR gene editing:
HJ Longhurst et al. N Engl J Med 2024; 390:432-441. CRISPR-Cas9 In Vivo Gene Editing of KLKB1 for Hereditary Angioedema.
My take: Gene therapies have been very expensive. If this therapy is approved for hereditary angioedema it will be too. However, some of the current treatments for preventing hereditary angioedema are also quite costly.
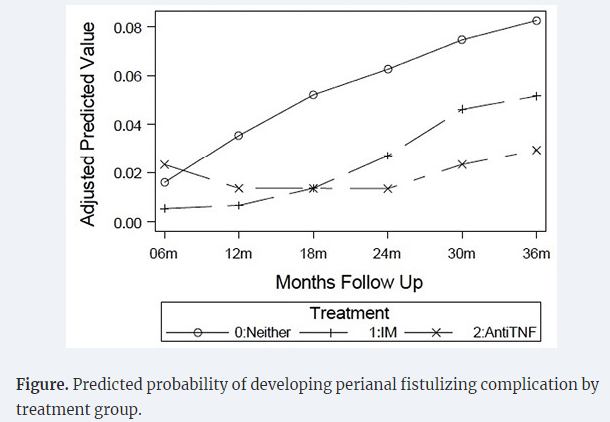
The authors utilized the prospectively-enrolled RISK cohort to assess the effect of early ANTI-TNF therapy and the development of perianal fistulizing complications (PFCs); this included 621 propensity-matched pediatric patients without PFCs at enrollment. ”The study included a moderately ill population, including 21% with growth delay, 43% with deep ulcers, and 70% with weighted pediatric Crohn’s disease activity index (wPCDAI) >30.”
Key findings:
Anti-TNF therapy was associated with 79% reduced odds of developing PFCs
The presence of perianal lesions increased the risk of PFCs more than 3-fold
My take: This study, in agreement with others (see below), shows that early treatment with effective therapy reduces the risk of disease complications like perianal fistulas.
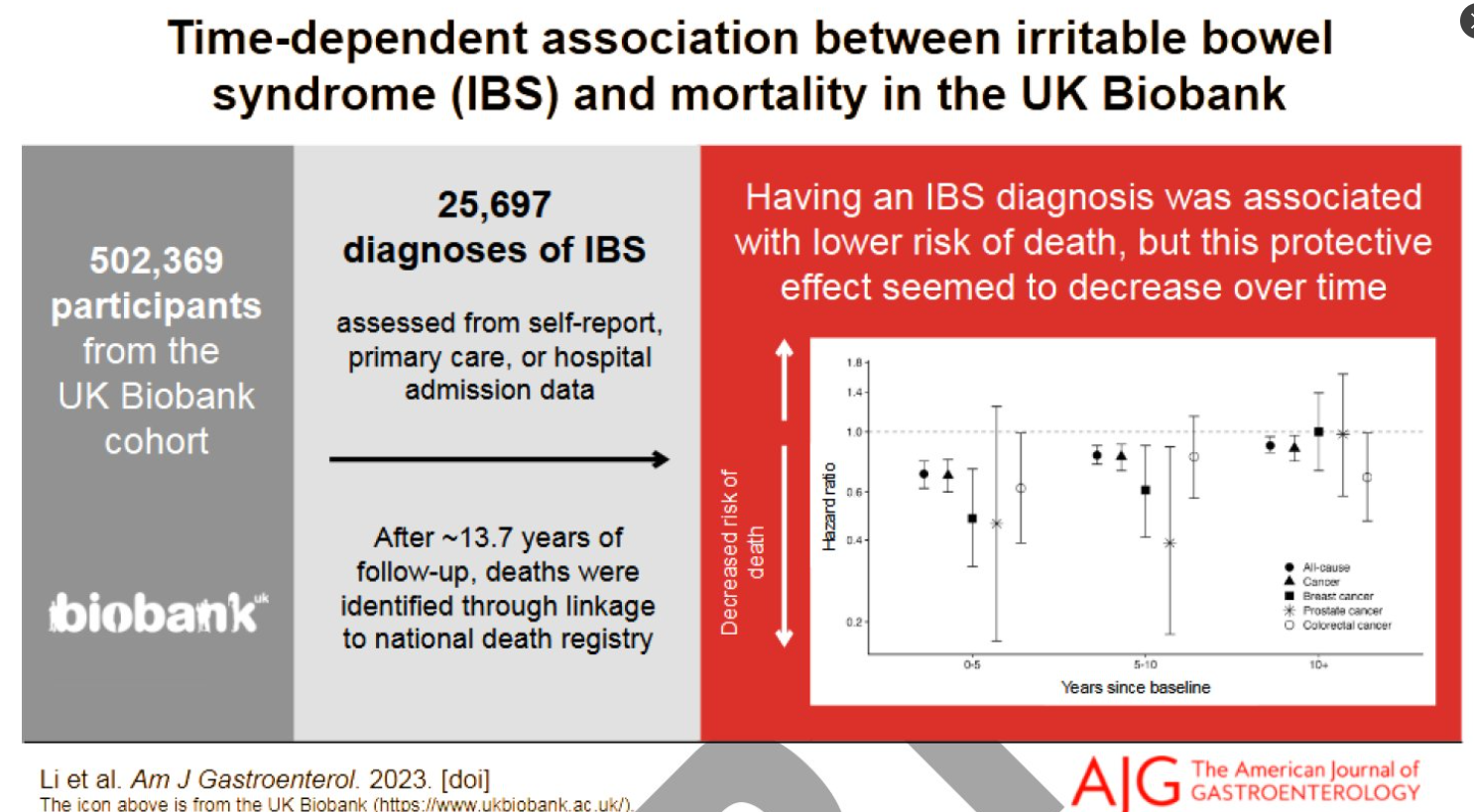
Having an IBS diagnosis was strongly associated with lower risks of all-cause (HR=0.70) and all cancer (HR=0.69) mortality in the first 5-years of follow-up. These associations were attenuated over follow-up, but even after 10 years of follow-up, associations remained inverse (all-cause: HR=0.89; all cancer: HR=0.87) after full adjustment.
Individuals with IBS had decreased risk of mortality from breast, prostate, and colorectal cancer in some of the follow-up time categories.
My take: Having IBS may cause suffering but appears to lower risk of death. The reason for this is not clear.
Takeda conducted two multicenter, randomized, placebo-controlled trials in patients 11 to 56 years and 11 to 42 years, respectively. The first found 53% of the treatment group achieved histologic remission compared to 1% receiving a placebo. The second found 38% of the treatment group achieved remission vs. 2% of the placebo group, according to Takeda…
Patients [need] to refrain from eating or drinking for at least 30 minutes after taking Eohilia. After 30 minutes, patients should rinse their mouth and spit to reduce the risk of developing thrush.
My take: Budesonide has been used effectively for EoE for a long time; it is good news that it is recognized by FDA with a specific EoE indication. However, it is a little concerning that the label indication is for 12 weeks when we know that this is chronic disease. Also, I am eager to see how much this formulation costs in comparison to the budesonide ampules.
A Berkwitt et al. NEJM 2024; 390: 358-366.Case 3-2024: An 8-Week-Old Male Infant with Inconsolable Crying and Weakness
This case report describes an 8 week old who been well until 7 days before the current presentation, when irritability, less frequent stooling and frequent crying developed. He was seen by his primary care clinic and symptoms were attributed to gas. Several days later, he presented to the emergency department with persistent crying but he had developed lethargy and weakness.
This case report details potential reasons for irritability in infants:
Infections
Neurologic causes including hydrocephalus
Ocular/skin such as a corneal abrasion and hair tourniquet
Cardiopulmonary causes such as heart failure and myocarditis
Gastrointestinal causes like colic, constipation gas, and reflux
Genitourinary like hernia and torsion
Musculoskeletal like fractures
Cancer including neuroblastoma and leukemia
Metabolic causes
Ingestions/Toxins
Then, the authors turn their attention to potential reasons for hypotonia:
CNS disease -accounts for 60 to 80% of cases of hypotonia, specifically hypoxic–ischemic encephalopathy and cerebral palsy
PNS disease -need to be considered in those with normal neuroimaging. To have an acquired PNS disease, the authors considered mainly botulism and Guillain-Barre syndrome.
Ultimately, the authors concluded that the infant likely had botulism which was in fact the correct diagnosis, confirmed by a stool test for Clostridium botulinum toxin type A (generally available only through local public health departments). Also, “On further interviewing, the patient’s family members reported that he typically had hard stools every 2 to 3 days. Two days before admission, the infant appeared to have abdominal discomfort, which his family members presumed was from constipation or gas. Honey was given to try to soothe him.”
Teaching points:
Don’t give honey or corn syrup to a baby, though “clearly defined food exposures, such as exposures to honey or corn syrup, account for only a minority of cases.8..Often, there is a history involving rural living, dust production, or nearby soil perturbation.9“
Give Baby BIG (infant botulism immune globulin) while waiting for results.
Try to ascertain dietary exposures when obtaining a history.
Of patients not achieving clinical response during 12-week induction, 53.7% achieved response following extended induction (additional 3 doses of IV infusion every 4 weeks)
With “extended induction,” total of 80.3% mirikizumab-treated patients achieved clinical response by W24
Methods: A network meta-analysis (NMA) was conducted to evaluate comparative efficacy of licensed biologics. Phase 3 randomized controlled-trials (RCTs) evaluating biologics approved by the European Medicines Agency or United States Food and Drug Administration as of 31 March 2023 for maintenance treatment of adult patients with moderate-to-severe CD were included, i.e. infliximab (IFX) intravenous (IV) and SC, adalimumab (ADL) SC, vedolizumab (VDZ) IV and SC, ustekinumab (UST) SC, and risankizumab (RZB) SC.
Key findings:
Among 8 comparator arms, IFX SC 120 mg every 2 weeks (Q2W) showed the highest odds ratio (95% credible interval) vs. PBO for clinical remission during the maintenance phase (3.52 [2.18–5.65]).
My take: This meta-analysis shows a favorable response for IFX SC; however, head-to-head trials are needed to really determine which biologic has the highest efficacy.
In this cross-sectional study with 104 children (24 with fatigue), biological parameters (CRP, fecal calprotectin) did not discriminate fatigued from non-fatigued patient
In this multicenter prospective study with 117 patients, the authors examined the success rate of adalimumab (ADA) in patients with CD with an intra-abdominal abscess resolved without surgery.
Key findings:
At W24, the survival rate without abscess recurrence or surgery was 74% (n=87)
Abscess drainage was significantly associated with ADA failure at W24 (odds ratio, 4.18)
My take (borrowed from authors): Provided that the abscess was carefully managed before initiating medical treatment, this study showed the high efficacy of ADA in the short and long term in biologic-naïve patients with CD complicated by an intra-abdominal abscess
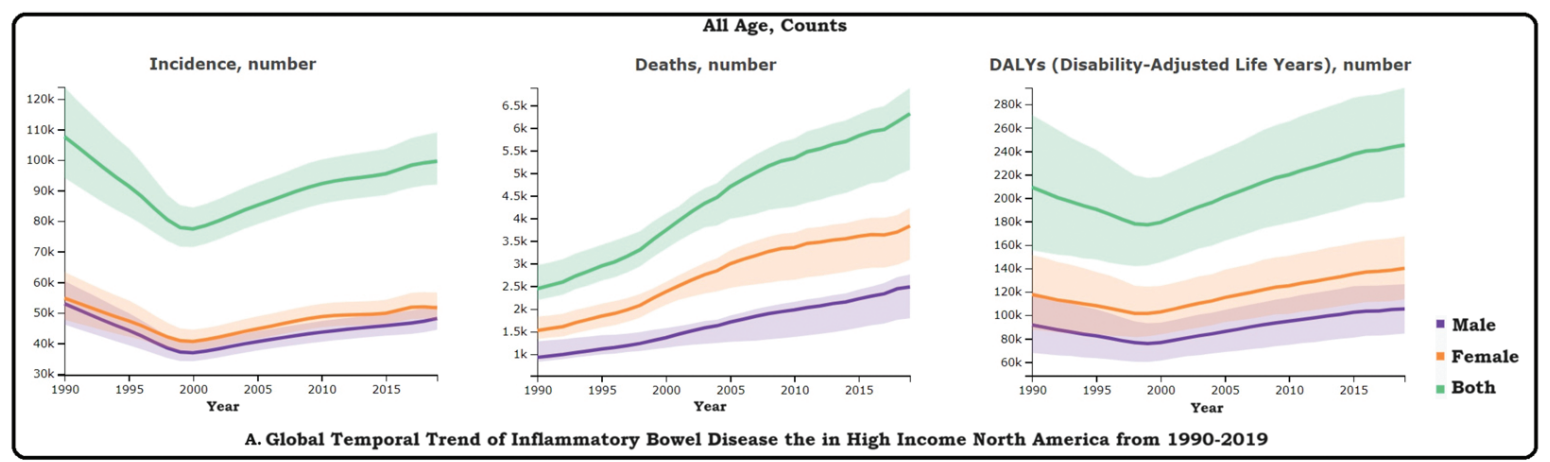
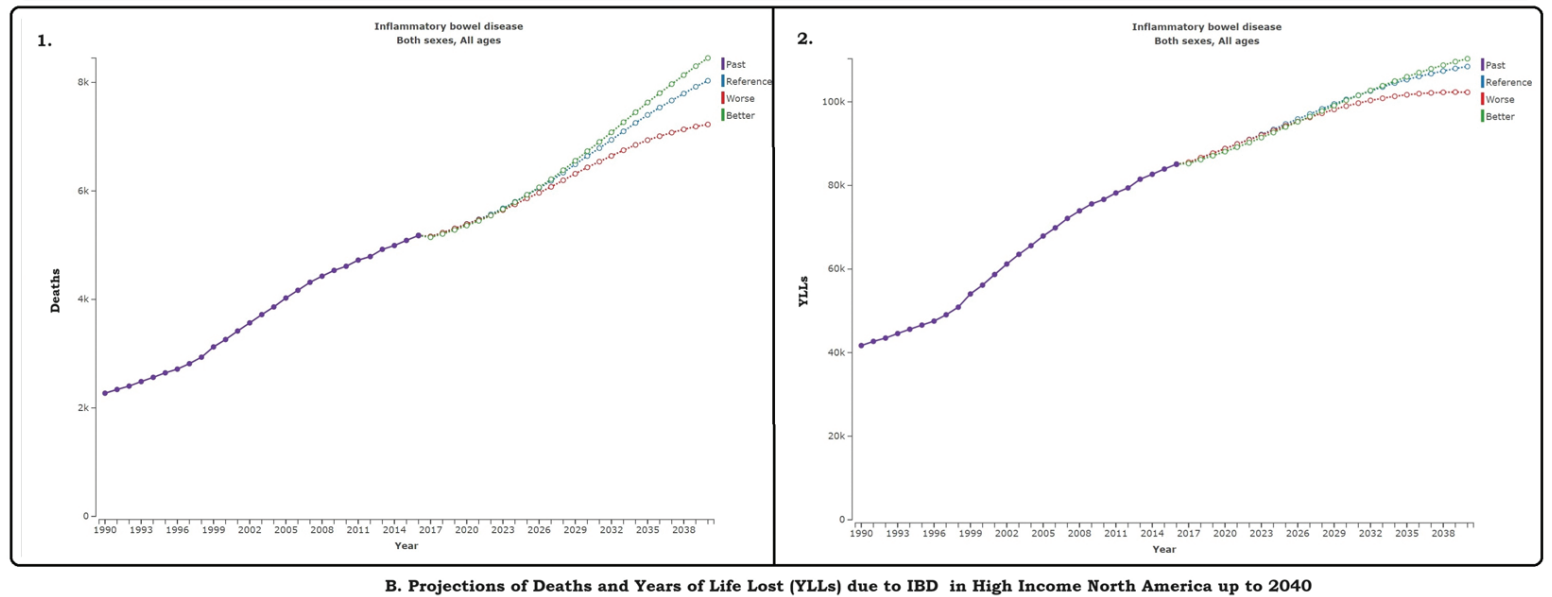
Methods: “Utilizing Global Burden of DIsease tool, we estimated IBD prevalence, incidence, mortality, and Disability Adjusted Life Years (DALYs) of IBD in High-Income North America. Standardized statistical techniques facilitated comparisons by age, sex, year within this specific region. The DisMod-MR 2.1 tool was employed to estimate incidence and prevalence, while mortality rates were discerned using the Cause of Death Ensemble Model (CODEm). Additionally, we projected the deaths and Years of Life Lost (YLLs) up to 2040 using regression analysis.”
My IT advisor (my youngest son) recommends using the Stolen Device Protection setting on the iPhone. The link below explains the rationale for this change, what’s affected, and how to adjust your settings.
N Hadzic et al. NEJM 2024; 390: 284-286.JAK Inhibition in STAT1 Gain-of-Function–Mediated Treatment-Resistant Autoimmune Hepatitis
In this case report, the authors describe a 21 month old who presented with jaundice and abnormal liver tests. Diagnostic evaluation identified high titers of LKM antibodies (1:10,520) along with liver biopsy findings consistent with type 2 autoimmune hepatitis (AIH). After 6 months of treatment with steroids and subsequently azathioprine, the patient continued with severe biochemical relapses and a liver biopsy showed only a partial response.
Subsequently, “genetic testing found the patient had a heterozygous c.821G→A p.(Arg274Gln) pathogenic variant in the gene encoding signal transducer and activator of transcription 1 (STAT1)… Functional assays in the patient repeatedly showed abnormally high STAT1 phosphorylation as compared with healthy controls; this confirmed an autosomal dominant STAT1 gain-of-function defect.”
Treatment with “baricitinib, an inhibitor of Janus kinase 1 (JAK1) and 2 (JAK2), was started. Within weeks, the patient’s aminotransferase levels normalized. ..A liver-biopsy sample that was obtained 4 months after the initiation of baricitinib therapy showed an absence of appreciable inflammation with residual mild fibrosis…She was weaned off mycophenolate and is continuing to receive daily baricitinib (8 mg) and prednisolone (2.5 mg) along with fluconazole and azithromycin for infection prophylaxis.”
My take: In children with refractory autoimmune hepatitis, genetic testing is worthwhile and may allow targeted therapy.
Patterns and Puzzles with VEO-IBD This is a very good review and the image on this day has one of my favorite patient t-shirts. STAT gain-of-function defects can cause VEO-IBD picture as well.
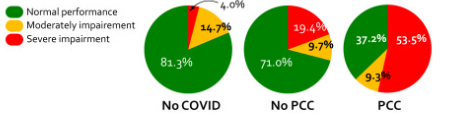
Methods: To examine cognitive slowing, patients with post-COVID-19 conditions (PCC) completed two short web-based cognitive tasks, Simple Reaction Time (SRT) and Number Vigilance Test (NVT). 270 patients diagnosed with PCC at two different clinics in UK and Germany were compared to two control groups: individuals who contracted COVID-19 before but did not experience PCC after recovery. For the SRT, participants were required to press the spacebar when a large red circle appeared in the center of the screen.
.**The simple reaction time task and the number vigilance task can be tried online at [https://octalportal.com/pcc]..
Key finding:
There was pronounced cognitive slowing in patients with PCC, which distinguished them from age-matched healthy individuals who previously had symptomatic COVID-19 but did not manifest PCC. Cognitive slowing was evident even on a 30-s task measuring simple reaction time (SRT), with patients with PCC responding to stimuli ∼3 standard deviations slower than healthy controls. 53.5% of patients with PCC’s response speed was slower than 2 standard deviations from the control mean, indicating a high prevalence of cognitive slowing in PCC.
Comorbidities such as fatigue, depression, anxiety, sleep disturbance, and post-traumatic stress disorder did not account for the extent of cognitive slowing in patients with PCC.
Cognitive slowing on the SRT was highly correlated with the poor performance of patients with PCC on the NVT measure of sustained attention.
Results of simple reaction time
My take (borrowed from authors): Using a 30-s web-based, self-administered psychomotor task, cognitive slowing in PCC can be reliably and easily measured as part of diagnostic work-up, and has potential to be a biomarker to track the progress of rehabilitation of PCC.
**The simple reaction time task and the number vigilance task can be tried online at [https://octalportal.com/pcc].