SA Ballal et al. J Pediatr 2024; 264: 113737. Comparing Gastrointestinal Endoscopy Findings in Children with Autism, Developmental Delay, or Typical Development
This retrospective study compared the findings of children with probable autism (ASD) to age- and gender-matched controls with developmental delay (DD) or with typical development (TD), (n= 526 ASD, 526 DD, 1052 TD). Key findings:
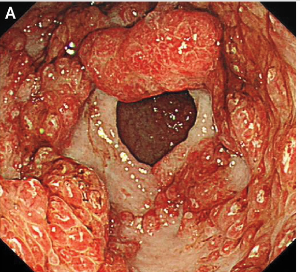
- Children with ASD had higher rates of abnormal esophageal histology (ASD 38.4%; DD 33.4%; TD 30.4%, P = .008)
- Stomach findings did not differ significantly among the groups: histologic inflammation was identified in ASD 13.3%, DD 18.5%, and TD 22.4% (P=.10).
- In the duodenum, histologic abnormalities were observed with lower frequency in ASD (ASD 17.0%; DD 20.1%; TD 24.2%, P = .005).
The authors emphasize the importance of the esophageal findings (increased rates of esophagitis). However, there are some important caveats that are not discussed in the paper:
- At baseline (prior to study), it was known that the ASD and DD groups had higher rates of eosinophilic esophagitis: ASD 9.1%, DD 9.5%, and TD 7.4% (Table 1). In addition, both of these groups had higher rates of gastroesophageal reflux at baseline: ASD 7.6%, DD 8.0%, and TD 6.5%. This selection bias is likely to negate much of the esophageal differences observed in their study. Also, the ASD group had much higher numbers receiving H2 blockers at time of procedure: ASD 11.4%, DD 10.3%, and TD 6.4%.
- In addition, the TD group had a much higher rate of abdominal pain as the indication for endoscopy (TD 26.6%, ASD 17.5%, and DD 20.2%). It is well-recognized that isolated abdominal pain has a low yield on endoscopy.
- The authors do not discuss the elephant in the room. What is the significance of microscopic esophagitis (or microscopic gastritis or microscopic duodenitis)? Previous authors have noted that “15% of healthy individuals may have microscopic esophagitis” (Gastroenterology 2018 (volume 154; pages 263-451 -see page 291). When we were looking at the variation of diagnostic yield for endoscopy, we decided to focus on colonoscopy because of the high rates of microscopic inflammation in the upper GI tract (related blog post: Our Study: Provider Level Variability in Colonoscopy Yield)
My take: In their discussion, the authors state that this study represents “significant progress in the understanding of gastrointestinal pathophysiology in children with ASD…suggest a unique fingerprint of findings in children with ASD.” In my view, the authors showed similar yield of EGD histologic abnormalities in all three groups and these microscopic findings are of uncertain significance.
Related blog posts:
- Esophageal Diseases Special
- Is Intestinal Function in Children with Autism Different?
- Briefly Noted: Microscopic Duodenitis and Autism
- Is It a ‘Waste’ to Do Colonic Manometry in Kids with Autism?
- Little Evidence to Support Dietary Intervention in Autism Spectrum Disorders