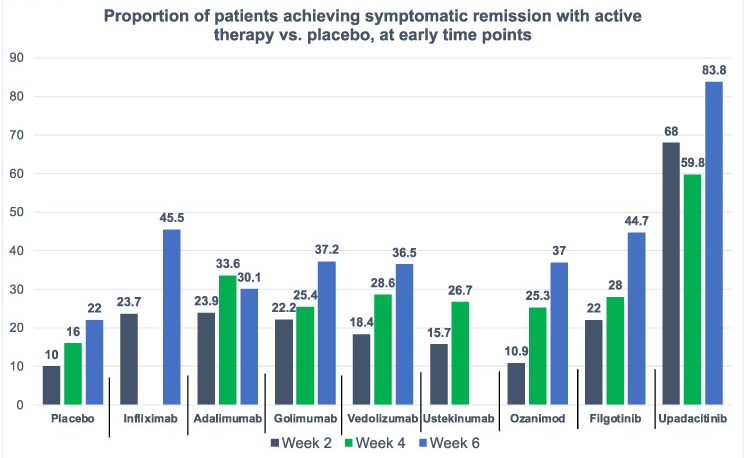
On network meta-analysis of 14 RCTs, upadacitinib was more effective than all agents in achieving symptomatic remission at weeks 2 (range of RR, 2.85–6.27), 4 (range of RR, 1.78–2.37), and 6 (range of RR, 1.84–2.79).
This study has a number of limitations including the following:
Potential differences in patient-level characteristics between these trials
Symptoms may not always correlate with endoscopic findings
Data from some medications (eg. tofacitinib) were incomplete and not included
My take: This study indicates an impressive early symptomatic response to upadacitinib compared to other agents for ulcerative colitis.
This article offers best practice advice -here are two of them:
#2: A Fibrosis 4 Index score <1.3 is associated with strong negative predictive value for advanced hepatic fibrosis and may be useful for exclusion of advanced hepatic fibrosis in patients with NAFLD.
#8 Patients with NAFLD and NITs (noninvasive tests) results suggestive of advanced fibrosis (F3) or cirrhosis (F4) should be considered for surveillance of liver complications (eg, hepatocellular carcinoma screening and variceal screening per Baveno criteria). Patients with NAFLD and NITs suggestive of advanced hepatic fibrosis (F3) or (F4), should be monitored with serial liver stiffness measurement; vibration controlled transient elastography; or magnetic resonance elastography, given its correlation with clinically significant portal hypertension and clinical decompensation.
In this study from U.S., patients (n=2523) were divided into three categories based on FIB-4 scores: (A) Fibrosis-4 (FIB-4) <1.3 and/or liver-stiffness measurement (LSM) measured by Fibroscan <8 kp, (B) FIB-4 1.31‒2.6 and/or LSM 8.1-12.5 kp, and (C) FIB-4 >2.6 and/or LSM >12.5 kp. However, those in class A with aspartate transaminase:alanine transaminase ratio >1 or platelets <150,000/mm3, or class B with aspartate transaminase:alanine transaminase ratio >1 or platelets <150,000/mm3 were upstaged by one class. The data were reviewed retrospectively from a prospective longitudinal cohort (TARGET-NASH)
Key findings: All adverse outcomes including liver and cardiovascular (see below) were correlated with FIB-4 staging.
Key findings: The prevalence of steatosis, severe steatosis, advanced fibrosis, and cirrhosis was 44.39%, 10.57%, 2.85%, and 0.87%, respectively in Chinese adults
Limitation: This data was derived from a health checkup cohort which could give different results than a random population sampling. Patients at health checkups may be more health conscious and/or be aware of underlying health concerns.
Prevalence of different grades of liver fibrosis in different age groups.
My take: Steatotic liver disease is a huge worldwide problem. The growing prevalence is going to result in extensive health issues.
—————
This year’s pumpkin 910/31/23):
It does not look like I will become a professional pumpkin artist anytime soon!
Methods: Consecutive adult patients (n=393) with refractory heartburn/regurgitation symptoms underwent standard 24-hour pH-impedance monitoring and completed questionnaires assessing past and current gastrointestinal and psychological health. Refractory reflux meant that they continued to have symptoms after completing at least 12 weeks of PPI (twice per day) treatment.
Key findings: Psychological symptoms were significantly associated with reflux symptom severity, and physiological reflux variables (eg, number of reflux episodes) were not.
In the discussion, the authors note that ” prior research demonstrates psychological symptoms, including depression, anxiety, and post-traumatic stress, are associated with reflux symptom severity.25, 26, 27 Indeed, psychological processes are believed to impact the brain–gut axis, particularly its central components,28 leading to enhanced esophageal symptom perception and reporting.6,29,30“
My take: Psychological factors (depression, anxiety, post-traumatic stress, and poor sleep) are important factors in refractory reflux and they need to be considered early in the evaluation.
A related article: NY Times Magazine 10/4/23, M Velasques-Manoff. The Mystery of My Burning Esophagus. In this article, the writer describes burning pain associated with his diagnosis of eosinophilic esophagitis. This article has some useful information about eosinophilic esophagitis and about lingering symptoms after responding to treatment.
“My new gastroenterologist had a theory to explain the all-consuming pain under my sternum. Sometimes patients develop a hypersensitivity syndrome, she told me. The original insult — in my case, inflammation of some kind — might be long gone, but the nerves that convey pain can become overactive and begin firing at the slightest provocation…Scientists don’t completely understand how antidepressants help pain syndromes, but certain ones seem to impede pain signals in the nervous system…
Doctors are increasingly aware of these kinds of pain syndromes in many disorders, including GERD. The condition, whose primary symptom is known colloquially as heartburn, is pervasive, afflicting an estimated one in five Americans. Some of these patients continue to feel intense pain even after their stomach acid has been reduced with antacids, a malady most likely caused by a hypersensitivity syndrome similar to mine.”
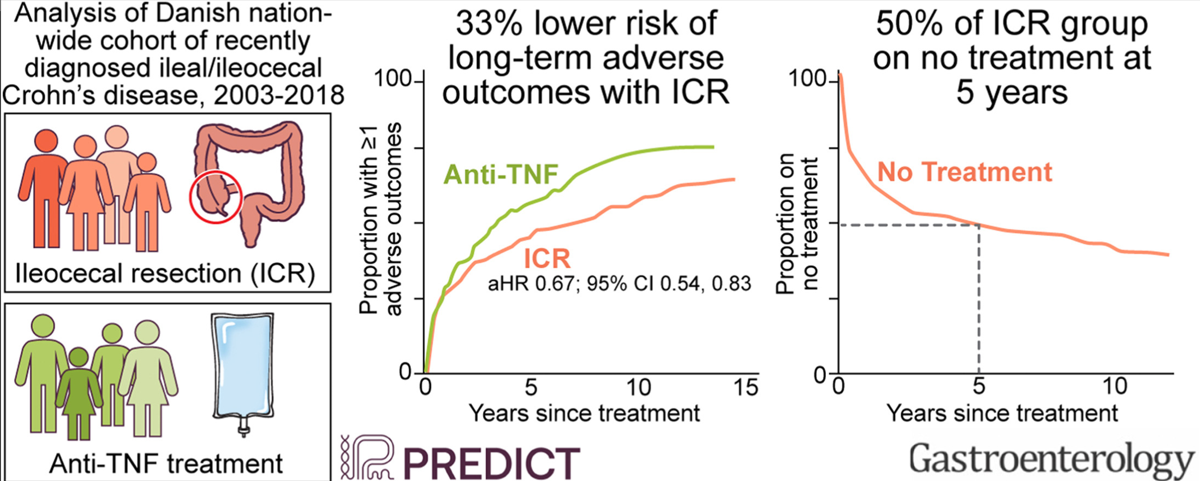
In this study from Denmark (2003-2018) using the Danish National Patient and Prescription Registries, the role of early ileocecal resection (CR), n=581, was compared with anti-TNF treatment, n=698. The primary outcome was a composite of ≥1 of the following: CD-related hospitalization, systemic corticosteroid exposure, CD-related surgery, and perianal CD. Only 178 patients (13.9%) were less than 17 years old. ICR cohort had surgery within 5 months of diagnosis in 85%, and in all within 1 yr of diagnosis. Key findings:
The risk of the composite outcome was 33% lower with ICR compared with anti-TNF (adjusted hazard ratio, 0.67; 95% confidence interval, 0.54–0.83). ICR was associated with reduced risk of systemic corticosteroid exposure and CD-related surgery, but not other secondary outcomes
Of individuals who underwent ICR, the Kaplan-Meier estimate of the proportion who postoperatively initiated IMM, initiated anti-TNF treatment, underwent another intestinal resection, or were on no treatment at 5 years of postoperative follow-up was 46.3%, 16.8%, 1.8% and 49.7%,
Of those who were initiated on infliximab as primary therapy, the Kaplan-Meier estimate of the proportion who underwent ICR, switched to a different biologic agent, or continued infliximab at 5 years of follow-up was 17.7%, 40.8%, and 47.3%
The authors note that their cohort had infrequent complicated disease: “Before ICR, 21% were diagnosed with a stricture, ileus, internal fistula, or abscess, indicative of complicated CD and representative of the real world. In contrast, only 1.7% in the anti-TNF group had complicated CD.”
My take: This study suggests that ICR may be a reasonable option in many cases of Crohn’s disease at an earlier stage rather than reserved for only those with refractory disease and complications. However, in pediatric patients, I would be more reluctant to start with a surgical approach given even longer time frame in which further surgery could be needed.
In 2022, a study in JPGN showed that the rate of Hepatitis B virus (HBV) vaccination and immunity was similar in individuals with and without celiac disease (CD). In addition, there was no increased risk of HBV infection detected in CD patients. Thus, routinely checking hepatitis B status in all patients with CD was no longer justified. (See: Celiac Disease, Hepatitis B and Paul Harvey).
The same researchers in this study expand their findings to inflammatory bowel disease (IBD) and CD. In this retrospective cohort (2000-2019), using the Rochester Epidemiology Project which includes data from 162,847 residents. Key findings:
1264 incident cases of IBD/CD, only 6 HBV infections were diagnosed before the index date; 5 of the 6 had risk factors including IV drug use or living in endemic region.
No new HBV infection developed in any of 1258 patients with IBD/CD during a median follow-up of 9.4 years
The proportion of patients with HBV-protective titers (≥10 mIU/mL) decreased with time before plateauing, with protective titer rates of 45% at 5 up to 10 years and 41% at 15 up to 20 years after the last HBV vaccination. The control population with protective titers also decreased similarly with time though was consistently higher than the levels of patients with IBD/CD within 15 years after the last HBV vaccination
Context/Discussion:
Only 16% of vaccine recipients have measurable protective titers by age 18 years, according to the CDC.32
“Time-related waning of Ab levels to HBV after vaccination has unclear clinical significance. Although screening persons for HBV immunity by using anti-HBs titers is widely accepted, prior study results have shown that cellular immunity can also provide long-term HBV protection, even in the setting of nonprotective titers.”
Reactivation of HBV is a well-documented complication of immunosuppression in patients with IBD, and screening for dormant infection is of paramount importance at diagnosis
Limitations: the study population had a low rate of HBV acquisition; thus, the study findings may not apply to areas with higher risk for HBV.
My take: This study shows that treating low hepatitis B surface antibody levels with reimmunization is likely NOT needed in either the IBD or the celiac disease population, except perhaps in those at high risk. Checking HBV status prior to immunosuppressive therapy, though, is still needed to prevent reactivation of HBV in those at risk.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Yesterday’s post was meant to be published on Halloween –will need to fire my editor.
———-
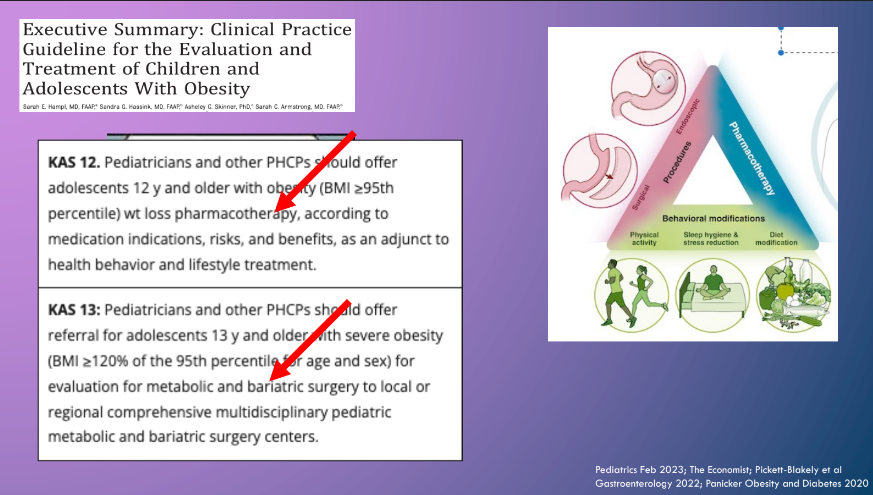
One of the highlights of NASPGHAN’s annual meeting is the Year in Review lecture. Sandeep Gupta, the editor of JPGN, provided a fantastic review. Here are some of the slides:
This review article makes a number of useful points:
Almost all of the IBD medications (Anti-TNF, Vedolizumab, Ustekinumab, Tofacitinib, Ozanimod) should not be used in patients with untreated hepatitis B surface antigen positivity. Antiviral prophylaxis is recommended even patients with inactive disease (HBV DNA <2000 IU/mL/normal ALT) starting 2 weeks prior to immunosuppression up to 12 weeks after immunosuppression discontinuation.
Anti-TNF, Vedolizumab, and Ustekinumab can be safely used in patients with cirrhosis, tofacitinib requires a dose reduction, and ozanimod is NOT recommended
Autoimmune hepatitis may be triggered (rarely) by use of anti-TNFs; however, these agents have been uses off-label as a rescue therapy for AIH as well.
Anti-TNFs do not appear worsen liver function in PSC and may be associated with improvement in MASH (NASH)
Drug-induced liver injury (DILI) is common with anti-TNFs, often seen between the second and fifth doses. It is “generally transient and asymptomatic.” DILI may occur with ustekinumab, tofacitinib and ozanimod.
Tofacitinib may have a favorable effect on PSC. A retrospective study with 5 patients reported a 28% and 39% decrease respectively in total bilirubin and alkaline phosphatase within 6 months of starting therapy, A separate study with 42 patients showed a non-significant drop in alkaline phosphatase from 150 U/L to 132 U/L at 12 month followup.
The authors note that in patients with cirrhosis and posttransplantation, “vedolizumab and ustekinumab should be preferred due to their safer profile linked to infectious risk.”
“Patients with hepatobiliary disorders are often excluded from pivotal trials.” This contributes to a significant knowledge gap for patients with these comorbid conditions which are frequent in patients with IBD
My take: I don’t think I will be too popular if I hand out copies of this article to the kids I see later today –despite the useful advice. (This post was meant to be published on Halloween)
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
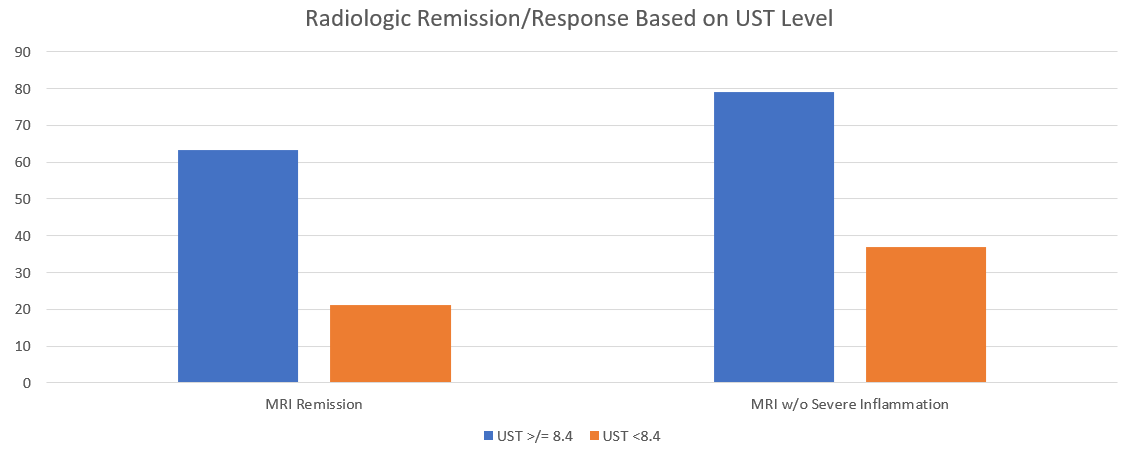
This retrospective trial included thirty three patients with Crohn’s disease (CD) receiving maintenance ustekinumab (UST). The simplified Magnetic Resonance Index of Activity (sMARIA) and biomarkers were correlated with UST levels. The authors utilized a homologous mobility shift assay (HMSA) (Prometheus) for their UST levels.
Key findings:
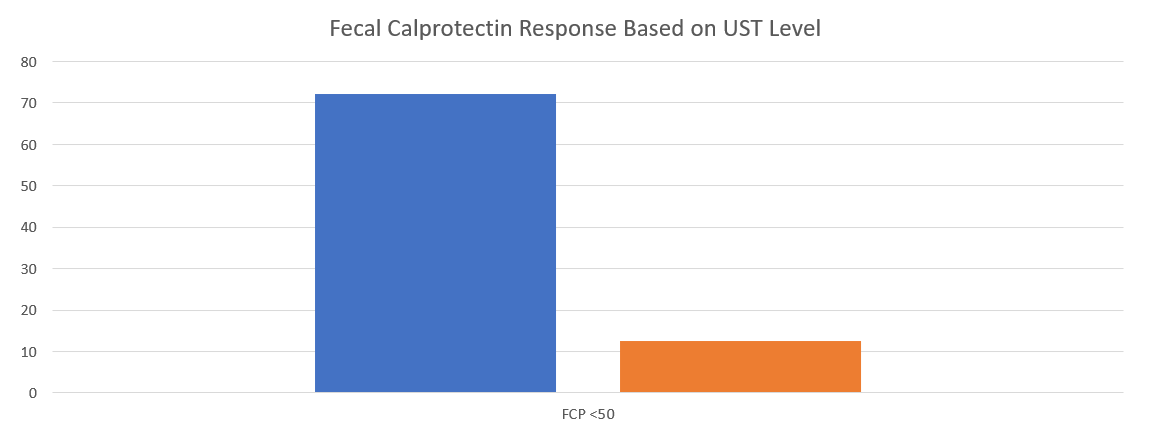
With UST level greater or equal to 8.4, radiologic remission was seen in 63% compared to 21% in those with levels <8.4. Similarly, the absence of severe inflammation was seen in 78.9% of those with higher levels compared with only 36.8% in those with levels below 8.4. Both findings were clinically-significant P=.01With UST levels greater or equal to 6.1, FCP less than 50 was seen in 72.2% compared to only 12.5% in those with a level less than 6.1. P<.01
My take: This study show the need for higher levels of UST to achieve optimal outcomes. Levels of at least 8.4 appear to be a good target.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
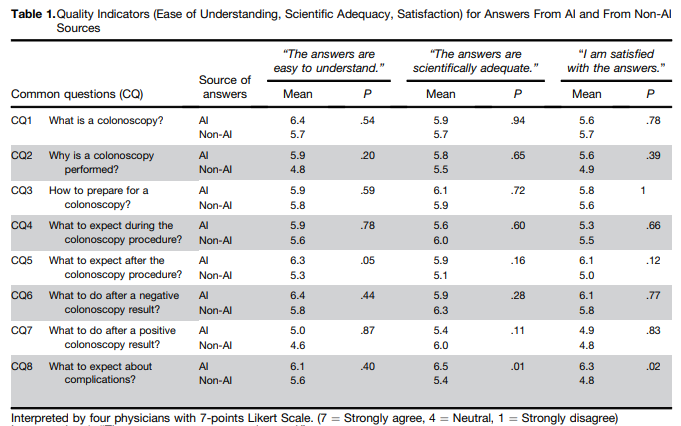
In this study, ChatGPT answers to questions about colonoscopy were compared to publicly available webpages of 3 randomly selected hospitals from the top-20 list of the US News & World Report Best Hospitals for Gastroenterology and GI Surgery.
Methods: To objectively interpret the quality of ChatGPT-generated answers, 4 gastroenterologists (2 senior gastroenterologists and 2 fellows) rated 36 pairs of CQs and answers, randomly displayed, for the following quality indicators on a 7-point Likert scale: (1) ease of understanding, (2) scientific adequacy, and (3) satisfaction with the answer (Table 1) Raters were also requested to interpret whether the answers were AI generated or not.
Key findings:
ChatGPT answers were similar to non-AI answers, but had higher mean scores with regard to ease of understanding, scientific adequacy, and satisfaction.
The physician raters demonstrated only 48% accuracy in identifying ChatGPT generated answers
My take: This is yet another study, this time focused on gastroenterology, that show how physicians/patients may benefit from leveraging chatbots to improve communication.
The authors used data from ASPirin in Reducing Events in the Elderly (ASPREE), a randomized prospective trial of aspirin in the United States and Australia, including 18,934 community-based adults ≥65 years of all races/ethnicities (enrollment 2010-2014). Final cognitive testing was done in 2017. Key Findings:
Baseline PPI use vs nonuse was not associated with incident dementia (multivariable hazard ratio, 0.88, cognitive impairment without dementia (multivariable hazard ratio, 1.00), or with changes in overall cognitive test scores over time.
Also, no associations were observed between H2RA use and all cognitive endpoints.
My take: ” These data provide reassurance about the safety of long-term use of PPIs among older adults.” PPIs are unlikely to have negative effects on cognition.