JW Chang et al. Clin Gastroenterol Hepatol 2023; 21: 1690-1698. Open access! Development of a Practical Guide to Implement and Monitor Diet Therapy for Eosinophilic Esophagitis
- The authors note that dietary therapy is underutilized–“successful clinical implementation is hampered by the need for a multidisciplinary approach including dietitian support and provider expertise.”
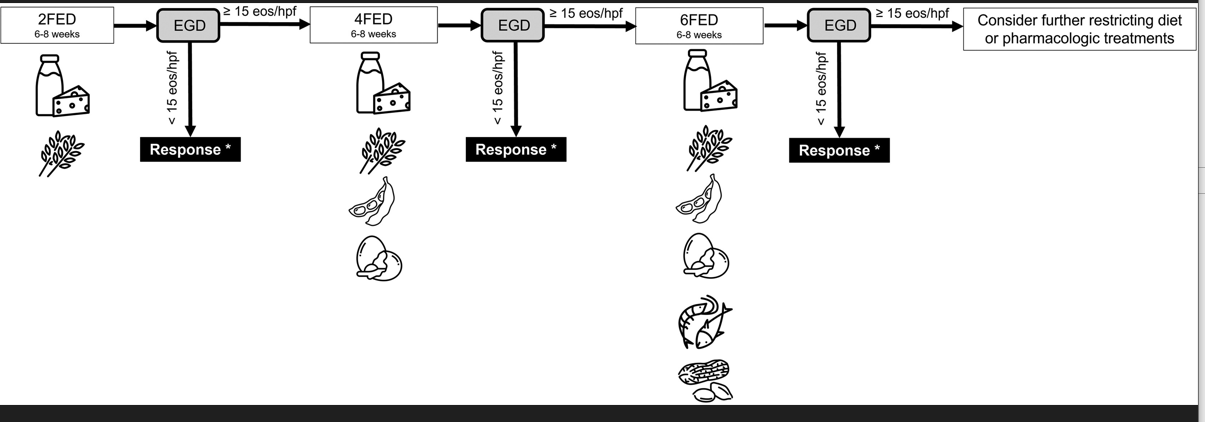
- “Because symptoms are often discordant with underlying disease activity, symptoms alone should not be used to make decisions about treatment changes.56 Relying on symptoms in isolation to guide food elimination or reintroduction is insufficient and can result in false identification of food triggers and unnecessarily prolonged dietary restriction. Patients should be warned that their trigger foods are not necessarily the foods that cause immediate symptoms related to obstruction (eg, commonly meats, bread, sticky textures). Endoscopy with biopsy is the gold standard for monitoring response to therapy and is recommended at least 6–8 weeks after a change in therapy, including elimination and reintroduction phases to identify of food triggers.57“
- “The most identified food triggers for EoE are animal milk (up to 90%) and wheat (up to 75%), and up to half of patients who undergo dietary therapy will have more than 1 dietary trigger. 58,62 In a recent study of adult patients undergoing dietary therapy with the SFED, 69% of patients had only 1 food trigger identified, making this a reasonable option for long-term therapy.59“
- “The most common reasons for nonresponse to the elimination phase include purposeful or inadvertent dietary nonadherence, cross-contamination, and incorrect or inadequate removal of potential food triggers”
- While medications used for EoE treatment are expensive, repeated endoscopy for dietary therapy may be costly and is an important consideration
- The Consortium of Eosinophilic Gastrointestinal Disease Researchers (CEGIR) 58 page Supplement in article: Resource Supplement for Dietary Management for Patients/families -includes guidance for selecting food, apps, websites


Related blog posts:
- “Tug” Sign For Eosinophilic Esophagitis and EoE Bowel Sounds Tips
- Eat More Chicken? (for EoE)
- FLUTE Study: Fluticasone ODT for EoE -Phase 2b Study Shows Efficacy
- What is EoE?
- How Useful Are 3-site Esophageal Biopsies for Eosinophilic Esophagitis
- Long-Term Treatment of Eosinophilic Esophagitis with Budesonide
- Dupilumab: FDA Approval for Eosinophilic Esophagitis
- Expecting Change in Eosinophilic Esophagitis Treatment | gutsandgrowth
- 4-14-4 Rule: More Biopsies Recommended for EoE
- Too Good To Be True: Two Lessons For Eosinophilic Esophagitis | gutsandgrowth
- 2020 Eosinophilic Guidelines (AGA)
- Eosinophilic Esophagitis -FAQs
- EoE Update 2018 (Dr. Seth Marcus)
- Eosinophilic Esophagitis -Up to Date Dietary Management Review
- Changing the Dietary Approach with Eosinophilic Esophagitis