When I lay down at night I thank the Lord above For giving me everything I ever could dream of
‘Cause I’ve got a roof over my head The woman I love laying in my bed And it’s alright, alright, alright, alright I got shoes under my feet Forever in her eyes staring back at me And it’s alright, alright, alright, yeah
I got all I need, yeah I got all I need And it’s alright by me, oh, yeah
This 38 page report has a ton of updated recommendations and useful advice –geared to adults with fatty liver disease. The last ~dozen pages are the 491 references.
Some of the useful points:
CVD and nonhepatic malignancies are the most common causes of mortality in patients with NAFLD without advanced fibrosis; death from liver disease predominates in patients with advanced fibrosis.
Initial lab evaluation in adults:
Statins are safe and recommended for CVD risk reduction in patients with NAFLD across the disease spectrum, including compensated cirrhosis.
Patients with NAFLD should be screened for the presence of T2DM. T2DM is the most impactful risk factor for the development of NAFLD, fibrosis progression, and HCC.108–111 Given the central pathogenic role that insulin resistance plays in the pathogenesis of both T2DM and NAFLD, it is not surprising that patients with T2DM have a higher prevalence of NAFLD (ranging from 30% to 75%)10,112,113 and a higher risk of developing NASH with fibrosis.93,114–117
Other important comorbidities: dyslipidemia, obstructive sleep apnea, cardiovascular disease, and chronic kidney disease
Lifestyle factors that can be beneficial:
Table 6 lists potential medications though there are no FDA approved treatments for fatty liver disease. Bariatric surgery is also a beneficial treatment option “in patients who meet criteria for metabolic weight loss surgery, as it effectively resolves NAFLD or NASH in the majority of patients without cirrhosis and reduces mortality from CVD and malignancy.”
Potentially useful medications include Vitamin E, Pioglitazone, Liraglutide, Semaglutide, Tirzepatide and SGLT-2i. “Semaglutide can be considered for its approved indications (T2DM/obesity) in patients with NASH, as it confers a cardiovascular benefit and improves NASH. Pioglitazone improves NASH and can be considered for patients with NASH in the context of patients with T2DM . Available data on semaglutide, pioglitazone, and vitamin E do not demonstrate an antifibrotic benefit, and none has been carefully studied in patients with cirrhosis.”
Treatments NOT Recommended: “Metformin, ursodeoxycholic acid, dipeptidyl peptidase-4, statins, and silymarin are well studied in NASH and should not be used as a treatment for NASH as they do not offer a meaningful histological benefit.”
When doctors use ChatGPT to find words to be more empathetic, they often hesitate to tell any but a few colleagues.
“Perhaps that’s because we are holding on to what we see as an intensely human part of our profession,” Dr. Moore said.
Or, as Dr. Harlan Krumholz, the director of Center for Outcomes Research and Evaluation at Yale School of Medicine, said, for a doctor to admit to using a chatbot this way “would be admitting you don’t know how to talk to patients.”
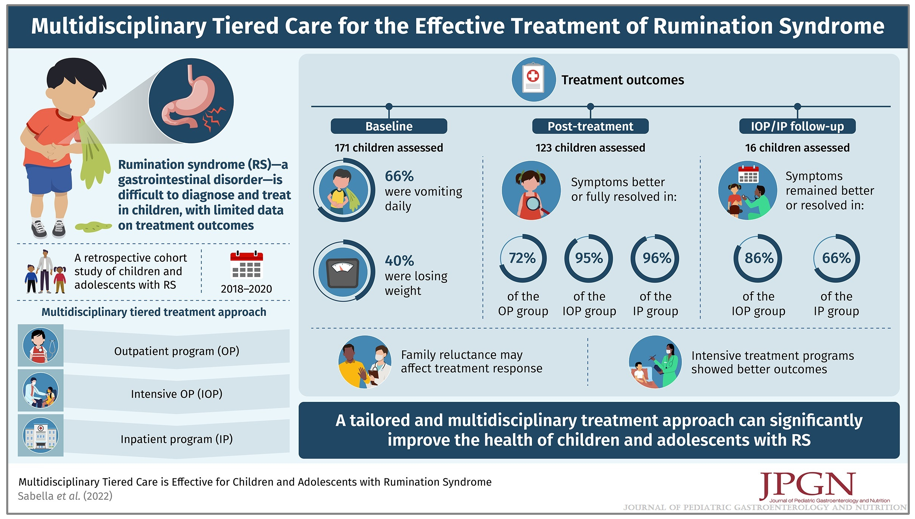
The was a retrospective single-center study (n=171). The median length of treatment was 6.5 months for outpatient care, four days for intensive outpatient care and nine days for intensive inpatient care.
Key findings:
After treatment, 72% of OP, 95% of IOP, and 96% of IP patients reported that symptoms were better or fully resolved compared to baseline
In a subset of 16 children, At follow-up (median 5.3 months), 86% of IOP and 66% of IP patients had symptoms that remained better or resolved.
The authors found “an association between patient or family reluctance to accept the diagnosis of rumination syndrome and a lack of response to treatment. Prior studies have demonstrated the importance of commitment and belief in the process of treatment and/or fully commit to the behavioral treatment process as a barrier to care.”
In a commentary on this article from Pediatrics Nationwide, Dr. Peter Lu noted: “What was striking to me was how effective the intensive treatment programs are. Both of those groups included the most severe of patients, oftentimes, they’ll have a feeding tube or a central line for parenteral nutrition. Even in that selected, very severe refractory group, we had very good response rates to treatment…RS is a disorder that cannot be effectively treated by a GI doctor alone…Treatment of RS involves a GI doctor and a GI psychologist, and we oftentimes will involve one of our GI dieticians”
My take: This study shows that treatment can be very effective in treating rumination syndrome, especially if the patient/family is amenable to therapy.
In this study with 39,734 commercially-insured initiators of IBD medications (18-64 year old), 34% had a colonoscopy by 12 months and 42% at 15 months. The authors state that “it is evident that patients without any colonoscopy during this interval are not being followed under an optimal long-term T2T (treat-to-target) paradigm.”
This retrospective study examined 123 patients with Crohn’s disease and 40 with ulcerative colitis who had dose intensification with ustekinumab (to either every 4 weeks, n=91, or every 6 weeks, n=72). Dose escalation was effective in both achieving and maintaining corticosteroid-free clinical remission for 61% of patients with Crohn’s disease and 40% with ulcerative colitis at 24 months; endoscopic remission was noted in 43% with Crohn’s disease and 55% with ulcerative colitis.
Using data from multiple studies with 1157 patients, only 9 tofacitinib patients developed Clostridioides difficile infection (CDI) which was lower than the placebo group. CDI were all mild–moderate in severity and resolved with treatment in 8 patients. Six of 9 patients continued tofacitinib treatment without interruption. The low rate of infection was likely in part due to screening for CDI prior to treatment. In addition, “it is possible than the lower rates of CDI …may be due to better-controlled disease…, thus reducing susceptibility to infection.”
One clinical pearl in the discussion: “When considering treatment [for CDI], initial therapy with oral vancomycin should be considered instead of metronidazole, and treating for at least 21 days should also be considered [in patients with IBD due to]…lower rates of CDI recurrence.”
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
“FDA has approved Linzess (linaclotide) capsules to treat functional constipation in pediatric patients 6 to 17 years of age. Linzess is the first treatment for pediatric functional constipation. The recommended dosage in pediatric patients 6 to 17 years is 72 mcg orally once daily.”
“The efficacy of Linzess for the treatment of functional constipation in pediatric patients 6 to 17 years of age was established in a 12-week double-blind, placebo-controlled, randomized, multicenter clinical trial (Trial 7; NCT04026113) and supported by efficacy data from adequate and well-controlled trials in adults with chronic idiopathic constipation (constipation that persists and isn’t connected to an underlying illness).”
Safety:
Most common adverse effect was diarrhea
Avoid in patients with known or suspected mechanical gastrointestinal obstruction (bowel blockage)
“Linzess contains a boxed warning that the medication should not be taken by patients less than 2 years of age”
My take: While this is good news to have the first FDA-approved treatment for pediatric functional constipation, it is worth remembering that the estimated cost for a monthly supply is between $514-$536 (in Atlanta pharmacies per GoodRx.com).
In the first study by Chehade et al, the authors analyzed six RCTs involving 324 patients. Key findings:
Compared with placebo, FMT has significant benefit in inducing combined clinical and endoscopic remission (odds ratio, 4.11; 95% confidence interval, 2.19-7.72; P < .0001)
clinical remission with FMT was 46.2% compared 22.5% for placebo
clinical response with FMT was 51.6% compared to 30.1% for placebo
endoscopic remission with FMT was 18.9% compared to 6.1% for placebo
endoscopic response with FMT was 36.7% compared to 22.4% for placebo
Discussion Points:
“The studies included in our article indicate that there is a shift in the microbiota composition of responders in the FMT group to resemble the profile of healthy donors”
FMT delivery via upper GI tract was equally effective as delivery via lower GI tract in these studies in inducing combined remission
“The understanding of FMT effectiveness for IBD is in its infancy.”
In the case report by Alomomen et al, a 34 year old with refractory ulcerative colitis and PSC (post-transplant) had not responded to infliximab, vedolizumab, adalimumab, tofacitinib or 10 months of ustekinumab (every 4 weeks). In addition, he was receiving tacrolimus therapy due to his liver transplant. His colonoscopy demonstrated a continuous Mayo 3 colitis. Subsequently, vancomycin therapy was added to his treatment (500 mg BID); he continued ustekimumab. Six months afterwards, his fecal calprotectin had dropped to 277 from 1600 and his CRP and hemoglobin had normalized. Repeat colonoscopy demonstrated complete endoscopic healing.
My take: There are many patients who do not respond to current IBD therapies. These two studies show that both FMT and vancomycin could be useful in selected patients.
Lego Art at Tucson Botanical GardensLego LionLego Panther
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
In this retrospective single-center pediatric (n=124) study, the authors analyzed complications that occurred up to 1 year after placement. Key findings:
29 (14.4%) major and 173 (85.6%) minor complications were reported
This study highlights at least 1 complication (regardless of severity) in 106 (85.5%) patients and reports a significantly lower complication rate in the PEG group (major and minor combined) compared to the surgical group (laparoscopy and laparotomy) (OR, 0.3; 95% CI, 0.07–0.9) (P = 0.001).
In the endoscopic group, patients with concomitant neurological disease had significantly more early complications (25.8 vs. 3.6%; OR, 9.1)
In the surgical group, patients with undernutrition had significantly more major complications (12.1% vs. 40%; OR, 4.7; 95% CI, 1.2–18; P = 0.01)
Discussion:
The authors note that although their results found fewer complications in the PEG group, other studies have reported lower complications in surgically-placed GTs. “Baker et al (4). report, like Sanderg et al (9)., an advantage of the laparoscopic technique compared to the endoscopy technique in terms of major complication (OR, 0.29; 95% CI, 0.17–0.51; P = 0.0001). Several other studies (9,20,21) show similar results.”
“Although a single prophylactic antibiotic therapy with cefazolin is systematically administered before each procedure, the rate of infectious complications remains high: 13 cases of abdominal wall abscess or cellulitis (6.4% of total complications) and 33 cases of minor infection (16.3% of total complications) requiring local treatment.”
The strengths of this study are an exhaustive collection of detailed data permitting a precise analysis of complications
My take: The majority of studies suggest that laparoscopic GT placement is safer, unlike this study. A more definitive answer would require a randomized prospective study with rigorously-collected data. Also, GT complications are common, ~85% in this study; thus, family education is important both before and after GT placement.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
In this cross sectional study (2010-2022) the authors calculated the proportion of infants (n=883) underweight and wasting with z scores below −2 SDs monthly from birth to 6 months of age at a single tertiary care center. Key findings:
Compared with expected proportion of underweight infants (2.3%), a larger proportion of infants with orofacial clefts were underweight between birth and 1 month (10.6%), peaking between 2 and 3 months (27.1%), and remaining high between 5 and 6 months (16.3%).
Compared with the expected proportion of infants with wasting (2.3%), a higher proportion of infants with orofacial clefts experienced wasting between birth and 1 month (7.3%), peaking between 2 and 3 months (12.8%), and remaining high between 5 and 6 months (5.3%).
Similar findings were observed for all cleft types and regardless of comorbidities.
“The mean prevalence of underweight in our sample exceeded that observed in children in African countries such as Tanzania and Uganda.”
My take: This study shows a high prevalence of underweight and wasting in infants with orofacial clefts.