As of 4/30/23, my blog posts will not be automatically uploaded to Twitter (see below). I will try to manually insert a link but there may be delays on many days. For those who access my blog through Twitter, a more reliable way to receive these posts is by signing up at gutsandgrowth.com.
Background: AASLD guidelines also suggest the use of budesonide with azathioprine as an alternative agent (to prednisone with azathioprine) in patients without cirrhosis or a severe acute presentation.1–3 However, particularly in pediatrics, there is concern that it is not as effective.
Methods: This was a retrospective, multicenter study of 105 naive AIH patients treated with budesonide as the first-line drug. The control group included 276 patients treated with prednisone.
Key findings:
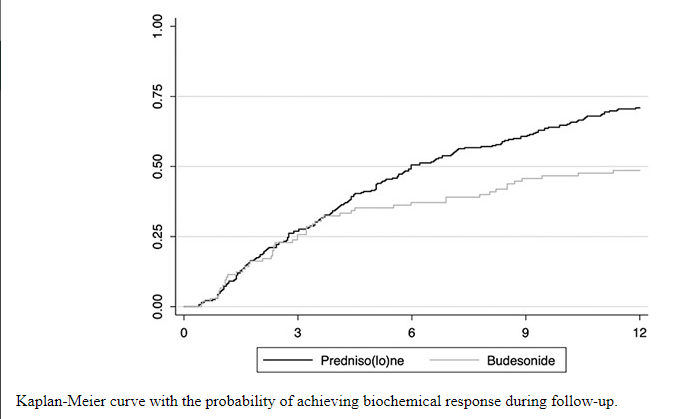
The biochemical response (BR) rate was significantly higher in patients treated with prednisone (87% vs. 49% of patients with budesonide, p < 0.001). BR was defined as normalization of both serum transaminases and IgG.
The probability of achieving BR was significantly lower in the budesonide group (OR = 0.20) at any time during follow-up, and at 6 (OR = 0.51) and 12 months after starting treatment (0.41)
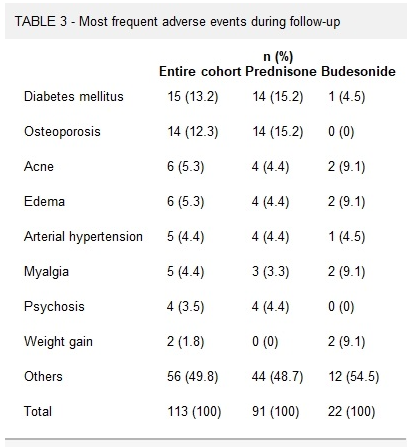
Prednisone treatment was significantly associated with a higher risk of adverse events (24.2% vs. 15.9%). These differences vanished when patients with cirrhosis were excluded from the analysis, showing a similar incidence of AEs in both groups (p = 0.119). Of the specific adverse effects, only the presence of osteoporosis was significantly higher in the prednisone group (mainly in those older than 60 years)
The authors note that budesonide was “only indicated in 5.4% of patients newly diagnosed with AIH… Budesonide was mainly employed in patients with low baseline transaminases, suggesting that this drug is preferred in patients with less severe disease.”
My take: “The use of budesonide in the real-life setting was low and was associated with a lower probability of achieving BR with respect to prednisone.” It likely needs to be restricted to those with mild disease, and those with adverse events with prednisone. Cost is less of an issue as budesonide can be obtained as a generic (Mark Cuban Costplus pharmacy: Budesonide).
The authors examined 29 RCTs (3772 patients). Key findings:
Only two medications (neither available in U.S.) were identified as being more effective than placebo for global symptoms of gastroparesis: clebopride (RR, 0.30) followed by domperidone (RR, 0.68)
Oral metoclopramide ranked first for nausea (RR 0.46), fullness (RR 0.67), and bloating. Though, use may result extrapyramidal adverse effects
I tend to abide by the recommendation proposed by Masaoka and Tack10 some years ago that one should use the term gastroparesis only “when persistently and severely delayed gastric emptying is found in the absence of mechanical obstruction.”
An obsession with gastroparesis as the basic issue among patients with “gastroparesis-like” symptoms has translated into a therapeutic fixation on the acceleration of gastric emptying. This too has led to frustration and disappointment. As already mentioned, symptoms are a poor predictor of the rate of gastric emptying, and a normalization of delayed emptying has not consistently correlated with symptom responses and vice versa.11,12
Oblivious to research illustrating how upper gastrointestinal symptoms can result from several other derangements in foregut physiology, such as impaired accommodation of the upper stomach, visceral hypersensitivity, and antropyloric distensibility and dysmotility,13, 14, 15, 16
My take: Currently, pharmaceutical agents geared towards symptoms like nausea and sensory disorders are much more promising than prokinetic agents for gastroparesis
This retrospective study (n=263) examined the rate of venous thromboembolism (VTE) in pediatric patients who required parenteral nutrition for at least 90 consecutive days.
Key findings:
The cumulative incidence of VTE was 28.1%, with a rate of 0.32 VTEs per 1000 catheter-days
The number of catheters and early gestational age were noted to be independent risk factors for VTE
No patients had progression of thrombus while receiving therapeutic anticoagulation
Of those with acute DVTs (n=47), 24 (51%)resolved on repeat imaging, 14 (30%)were stable, and and 9 (19%) had decreased
4.4% (2 of 45) had a major bleed while on anticoagulation
The authors note that the true rate of VTE is likely even higher because only 42% categorized as not having a VTE had undergone dedicated venous imaging.
My take: A lot of patients with intestinal failure develop VTE. Given the risks of treatment, the role of prophylactic anticoagulation remains unclear. This is where a prospective study would be helpful.
Background: “Chronic inflammation can lead to tissue remodeling in the esophagus with fibrosis in the lamina propria that is partially responsible for symptoms and complications of EoE.3,4 At times, a firmness to the esophagus can be appreciated with a noticeable force required to obtain biopsies from EoE. This sensation has been described as the “tug” or “pull” sign.5,6“
Methods: in this prospective study with 159 patients (128 pediatric, 31 adult), the authors devised a digital force gauge to measure the force required to take biopsy specimens. The study included 88 patients with EoE and 71 controls.
Key finding:
EoE patients showed an increase in the mean force required to obtain biopsies: 14.9 Newton (N) compared to 11.6 in control group
Peak force was greater in EoE patients: 20.4 N compared to 15 N in control group.
The pediatric subgroup had higher peak force in EoE patients: 22.4 N compered to 16.1 N for control group
My take: I had not heard of the term “Tug” sign for EoE, though it is something that is intuitive for GI providers who care for these patients. This study quantifies this problem.
“When you can measure what you are speaking about and express it in numbers, you know something about it; but when you cannot express it in numbers, your knowledge is of a meagre and unsatisfactory kind” –Lord Kelvin 1883
Y Usui et al. NEJM 2023; 388: 1181-1190. Helicobacter pylori, Homologous-Recombination Genes, and Gastric Cancer
Background: Gastric cancer is the fifth most common neoplasm and the fourth leading cause of death from cancer worldwide.1Helicobacter pylori has been classified as a group I carcinogen and is an environmental risk factor for gastric cancer.2 Although H. pylori infection affects more than half the world population
Methods: This study evaluated the association between germline pathogenic variants in 27 cancer-predisposing genes and the risk of gastric cancer in a sample of 10,426 patients with gastric cancer and 38,153 controls from BioBank Japan. This retrospective study also assessed the combined effect of pathogenic variants and H. pylori infection status on the risk of gastric cancer and calculated the cumulative risk in 1433 patients with gastric cancer and 5997 controls from the Hospital-based Epidemiologic Research Program at Aichi Cancer Center (HERPACC).
Key findings:
Germline pathogenic variants in nine genes: (APC, ATM, BRCA1, BRCA2, CDH1, MLH1, MSH2, MSH6, and PALB2) were associated with the risk of gastric cancer.
At 85 years of age, persons with H. pylori infection and a pathogenic variant had a higher cumulative risk of gastric cancer than noncarriers infected with H. pylori (45.5% vs. 14.4%).
Limitation: The study population was from East Asia and thus, the findings may be different in other populations.
My take: H. pylori infection has a synergistic effect in increasing the risk of gastric cancer in individuals with germline pathogenic variants in homologous-recombination genes. To minimize the risk of gastric cancer, H pylori eradication is important; however, it is especially in those with cancer-predisposing variants.
FDA has approved Daybue (trofinetide) oral solution as the first treatment for Rett syndrome, a rare, genetic neurological disorder. Daybue is approved for the treatment of Rett syndrome in adults and children 2 years of age and older.
Patients take Daybue either orally or via gastrostomy tube. The recommended dose is based on patient weight. Daybue is taken twice daily, morning and evening, with or without food.
Disease or Condition
Rett syndrome is a rare, genetic neurological and developmental disorder that affects the way the brain develops. Patients with Rett syndrome experience a progressive loss of motor skills and language. Most babies with Rett syndrome seem to develop as expected for the first six months of life. These babies then lose skills they previously had attained at approximately six to 18 months of age — such as the ability to crawl, walk, communicate, or use their hands. The hallmark of Rett syndrome is near constant repetitive hand movements, such as rubbing or clapping. Rett syndrome leads to severe impairments affecting nearly every aspect of life, including the ability to speak, walk, eat, and breathe.
The syndrome primarily affects females (1 in 10,000) and even more rarely affects males.
Effectiveness
The efficacy and safety of Daybue was evaluated in a randomized, double-blind, placebo-controlled, 12-week study (Study 1; NCT04181723) of patients with Rett syndrome five to 20 years of age. Patients were randomized to receive Daybue (N=93) or matching placebo (N=94) for 12 weeks. The dose of Daybue was based on patient weight to achieve similar exposure in all patients.
The co-primary efficacy measures were change from baseline in the Rett Syndrome Behavior Questionnaire (RSBQ) total score and the Clinical Global Impression-Improvement (CGI-I) score at week 12. The RSBQ is a 45-item rating scale completed by the caregiver that assesses a range of signs and symptoms of Rett syndrome. Lower scores represented lesser severity in signs and symptoms of Rett syndrome. The CGI-I is a 7-point scale rated by clinicians to assess how much a patient’s illness has improved or worsened. A decrease in CGI-I score indicates improvement.
Patients treated with Daybue demonstrated a statistically significant difference compared to placebo on the co-primary efficacy endpoints, as measured by the change from baseline in the RSBQ total score and the CGI-I score at week 12.
Safety Information
Most common adverse reactions, occurring in at least 10% of Daybue-treated patients and twice the rate of placebo, included diarrhea (81%) and vomiting (27%).
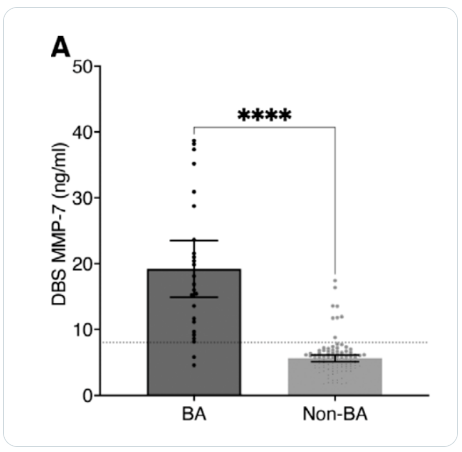
Methods: The study used stored DBS samples collected from 48 to 72 hours of life were retrieved from newborn screening centers in Taiwan (n=25 biliary atresia (BA), 107 non-BA)
Key findings:
MMP-7 levels of BA patients on the DBS were significantly higher than those of non-BA patients (19.2 ± 10.4 vs 5.6 ± 2.7 ng/mL, P value < 0.0001).
BA patients in this cohort underwent Kasai operation at a mean of 43 days. 32% (n=8) had surgery before 30 days of life, and 24% (n=6) had surgery after 60 days.
In this cohort, at time of publication, 9 (36%) of BA patients had received a liver transplantation at a mean of 2.4 years. Patients with their native liver tended to have had an earlier Kasai (38 days vs 54 days, P=0.057).
In their discussion, the authors note that BA starts very early in life. Increase in MMP-7 within 3 days of birth, supports “speculation that most BA ” may start before birth (JPGN 2019; 69: 396-403, What Is The Evidence That Biliary Atresia Starts in Utero?).
My take: Incorporating MMP-7 testing with newborn screening needs to be looked at in a bigger study. Efforts to identify BA cases earlier have largely been unsuccessful over the past several decades despite the knowledge that delayed diagnosis leads to worse outcomes.
S Travis et al. NEJM 2023; 388: 1191-1200. Vedolizumab for the Treatment of Chronic Pouchitis
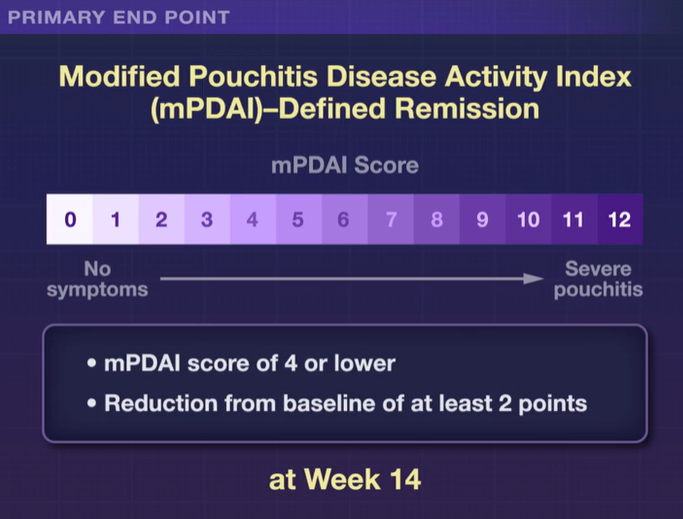
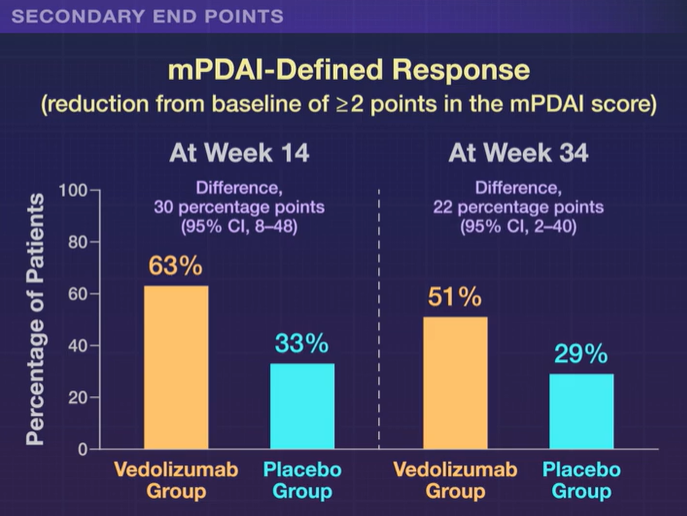
Methods: This was a a phase 4, double-blind, randomized trial (n=102 adults,EARNEST trial) to evaluate vedolizumab in adult patients in whom chronic pouchitis had developed after undergoing IPAA for ulcerative colitis.All patients received 4 weeks of ciprofloxacin and the treatment group received standard vedolizumab dosing. The primary end point was modified Pouchitis Disease Activity Index (mPDAI)–defined remission (an mPDAI score of ≤4 and a reduction from baseline of ≥2 points in the mPDAI total score; scores range from 0 to 12, with higher scores indicating more severe pouchitis) at week 14. The mPDAI is based on clinical symptoms and endoscopic findings.
Key findings:
The incidence of mPDAI-defined remission at week 14 was 31% (16 of 51 patients) with vedolizumab and 10% (5 of 51 patients) with placebo
Differences in favor of vedolizumab over placebo were also seen with respect to mPDAI-defined remission at week 34 (difference, 17 percentage points, 35% vs 18%)
My take: Vedolizumab is an effective treatment for chronic pouchitis.
Methods: This study analyzed postresection pediatric (≤18 years) CD patients (n=434) identified in the 2007–2018 IQVIA Legacy PharMetrics administrative claims database
Key findings:
Risk of surgical recurrence was 3.5%, 4.6%, and 5.3% at 1, 3, and 5 years, respectively
Postoperatively, patients were most commonly prescribed an immune modulator (33%), anti-tumor necrosis factor agent (32%), or antibiotic (27%)
My take: Current recommendations include postoperative endoscopic surveillance 6-12 months after surgery. Would the surgical recurrence rate have been lower if there had been higher postoperatively endoscopic evaluation?