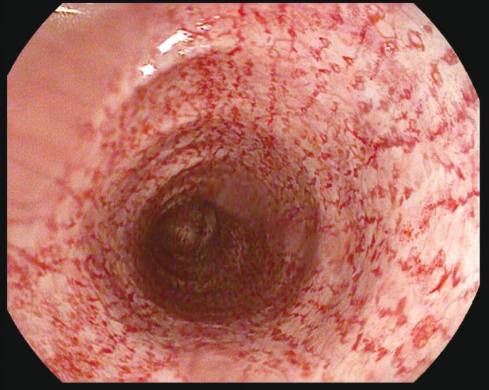
A Watson et al. JPGN 2024;79:1081–1083. Cat scratch colon in a patient with very early-onset Crohn’s disease with diverting ileostomy
Case report: This image is from the ascending colon of a 12 yo with Crohn’s disease sp diverting ileostomy.
“Cat scratch colon refers to the rare endoscopic finding of erythematous linear breaks that arise spontaneously, typically in the ascending colon and/or cecum, resembling scratches made by a cat, on otherwise unremarkable mucosa…It is presumed to be a benign condition likely caused by barotrauma from air insufflation during colonoscopy in a colon with altered elasticity or when the rate of insufflation exceeds the rate of air passage, such as in a diverted colon.2, 3“
My take: Surprisingly, the cat scratch colon finding is not consequential.
Using the ImproveCareNow prospective registry, the authors analyzed a total of 285,913 visits from 32,497 patients aged ≤ 21 years.
Key findings:
The occurrence of erythema nodousm (EN) was 1.57% and the occurrence of pyoderma gangrenosum (PG) was 0.90%. Co-occurrence of EN and PG was reported in 0.30% patients.
Both EN and PG were associated (p < 0.0001) with worse intestinal disease, lower remission, higher inflammatory markers, and extraintestinal manifestations (EIMs) arthritis and uveitis.
Limitations: “imperfect and incomplete data entry that may introduce bias. However, due to the extensive longitudinal data, we expect any bias to be minimal.”
My take: This study clarifies how common these dermatologic findings occur in pediatric patients with IBD. Prompt recognition of these disorders is important. Recently, our group cared for a 20 yo patient with inadequately-treated PG by multiple internal medicine physicians; this led to prolonged hospitalization.
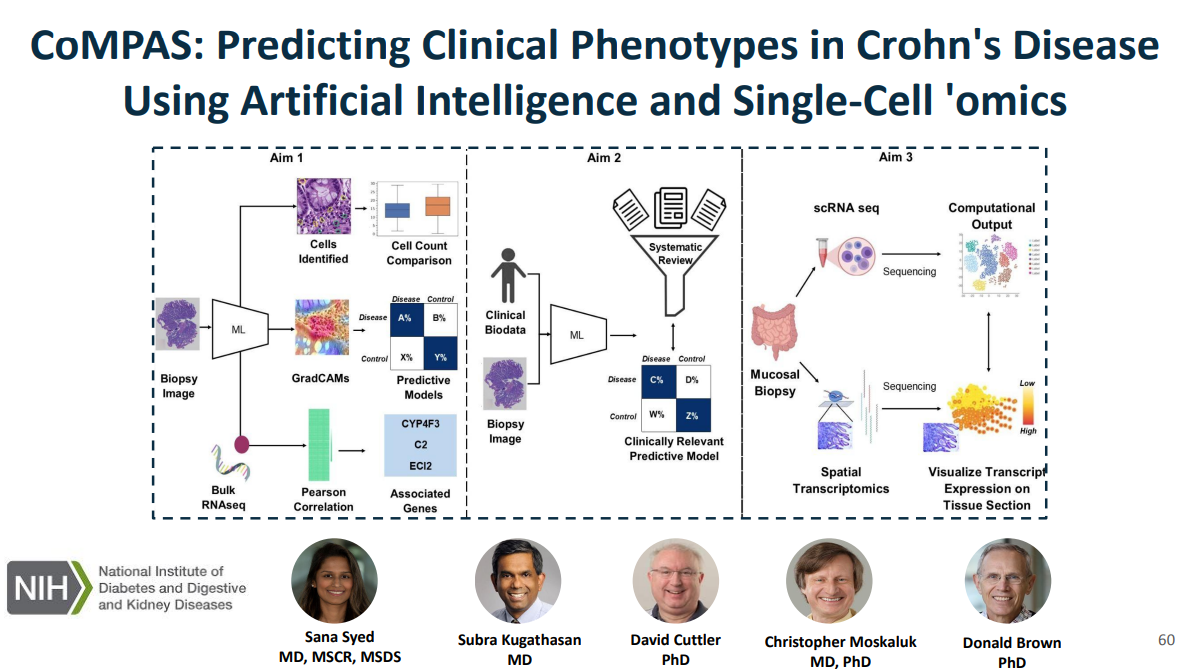
Recently, Dr. Sana Syed gave Children’s Healthcare of Atlanta Grand Rounds. She provided an excellent update on the development of artificial intelligence (AI) to select targeted therapies for pediatric gastroenterology diseases. My notes below may contain errors in transcription and in omission. Along with my notes, I have included many of her slides.
Key points:
One of the goals of using AI is to identify the right therapy at the time of diagnosis. Currently, diseases like eosinophilic esophagitis (EoE) and Crohn’s disease have multiple treatment options. However, many patients do not respond to first-line treatments; many develop complications due to not responding to treatment.
Currently we are lacking adequate biomarkers for individualized therapy. AI has the potential to sort through massive amounts of data (histologic, genetic, pharmacokinetics, transcriptome, metabolomics, etc) to allow for precision therapy.
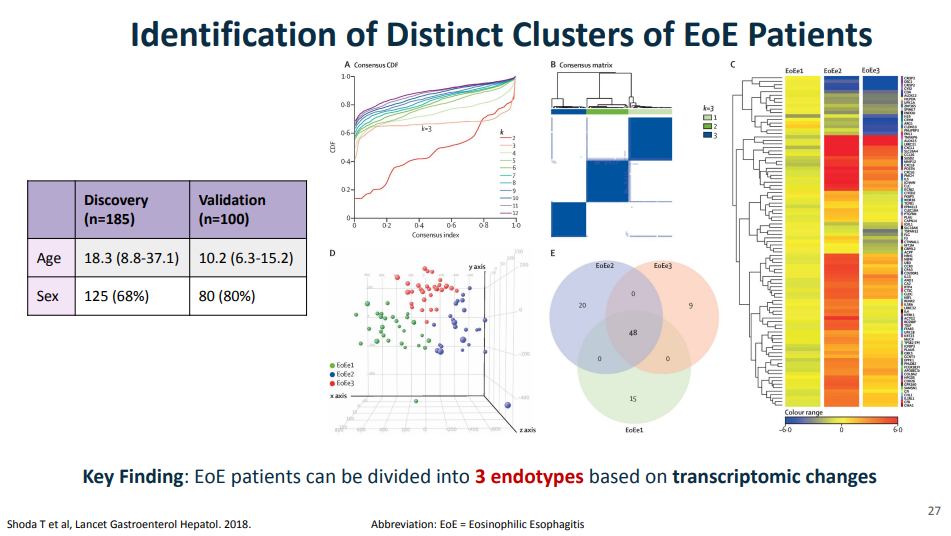
For EoE, machine-learning has already identified three subtypes that may affect clinical management. EoE1 is associated with a normal-appearing esophagus. EoE2 is associated with being steroid refractory. EoE3, when compared to the other two endotypes, is associated with adult-onset and narrow-caliber esophagus or stricturing.
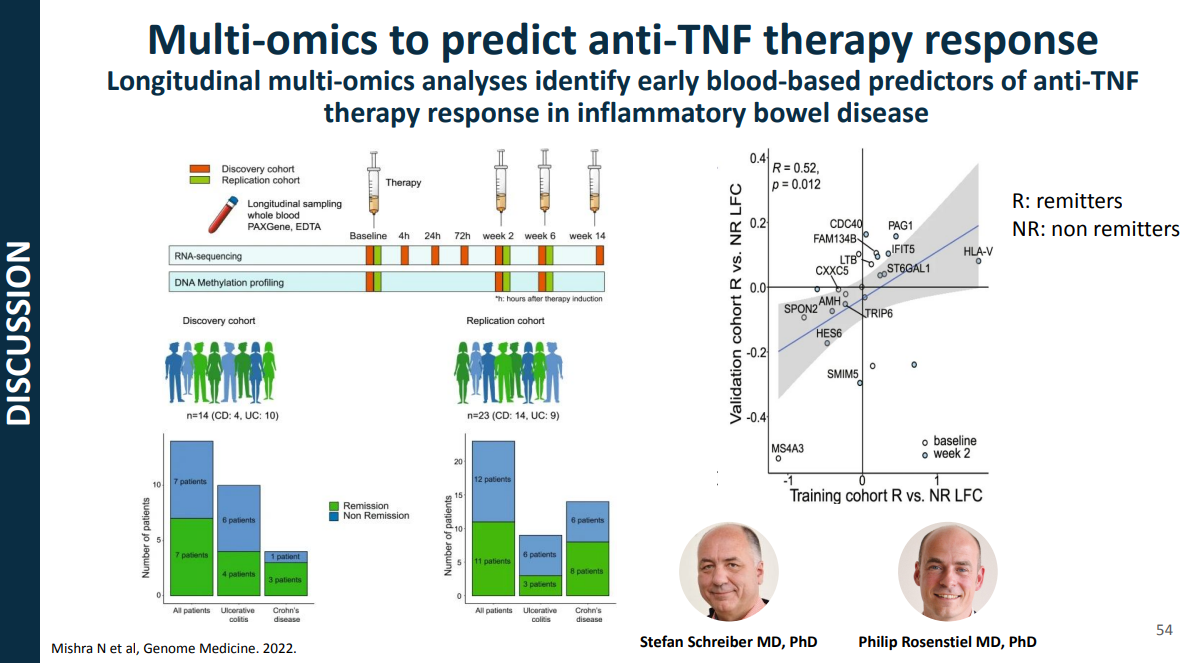
For Crohn’s disease, research has shown that younger age has been associated with an increased risk of not responding to anti-TNF therapy
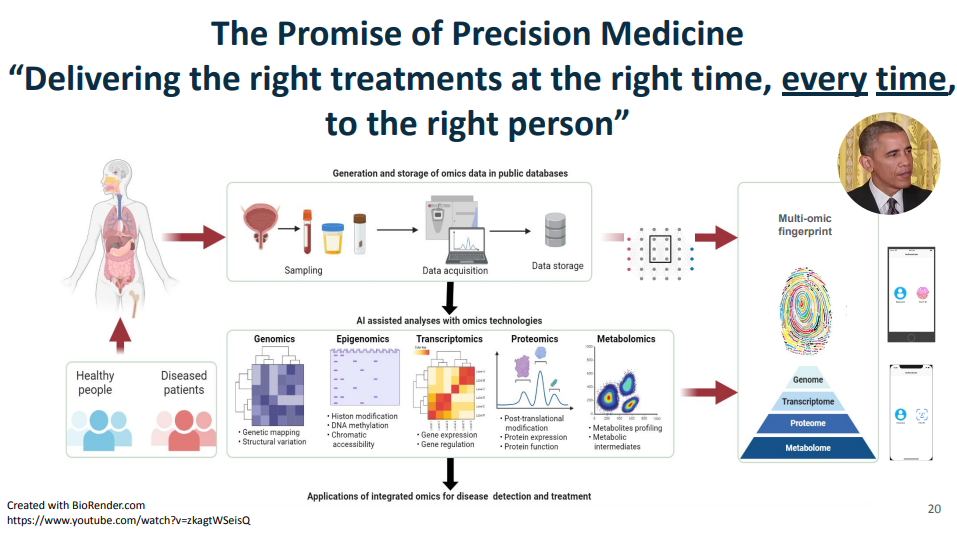
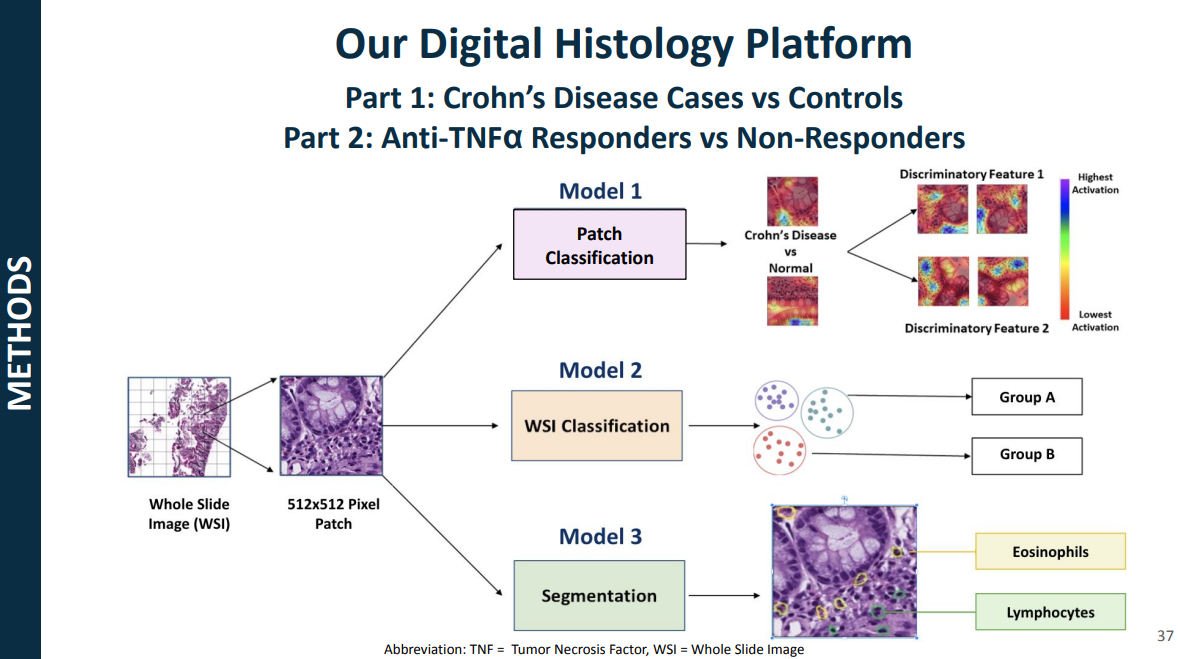
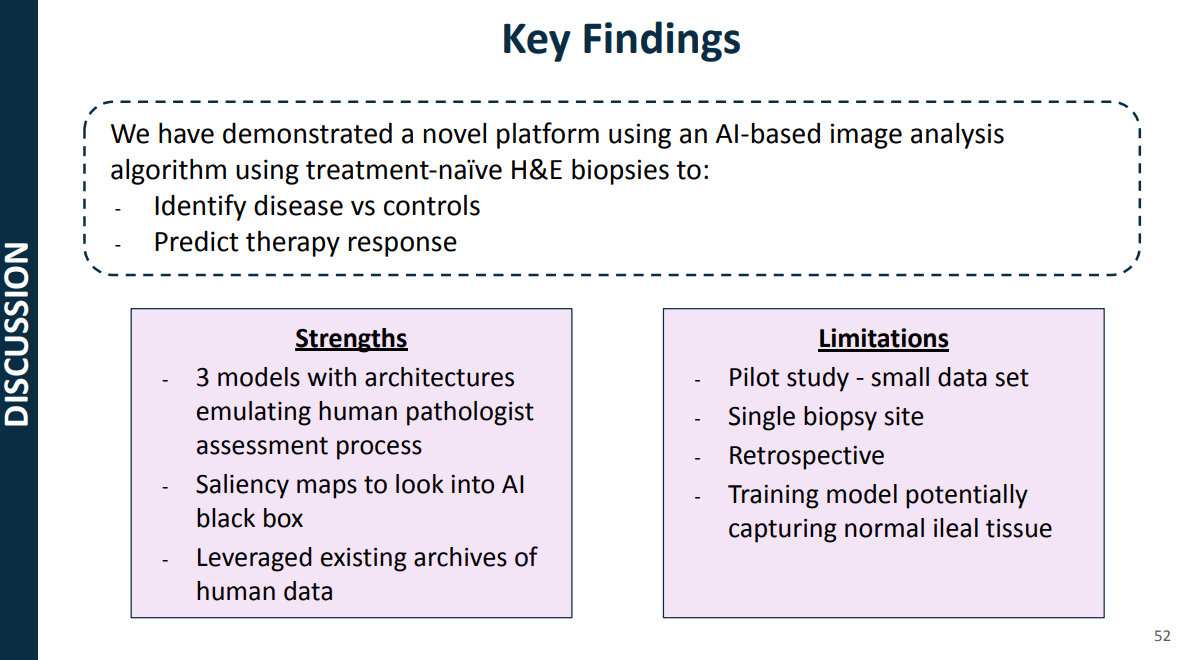
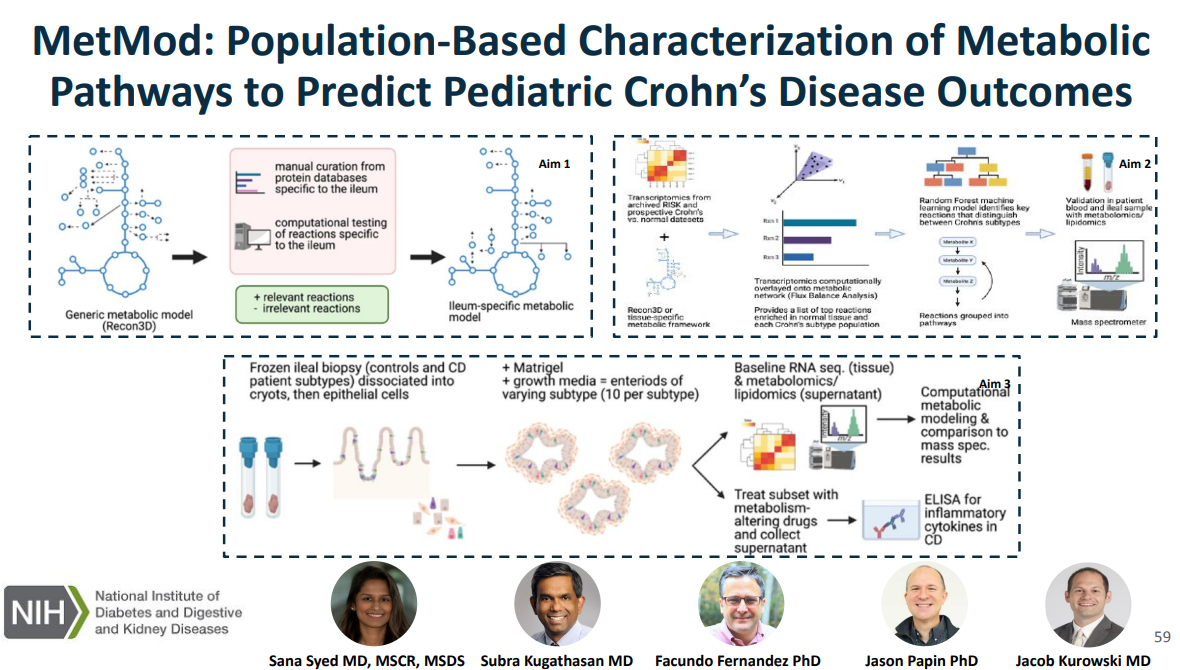
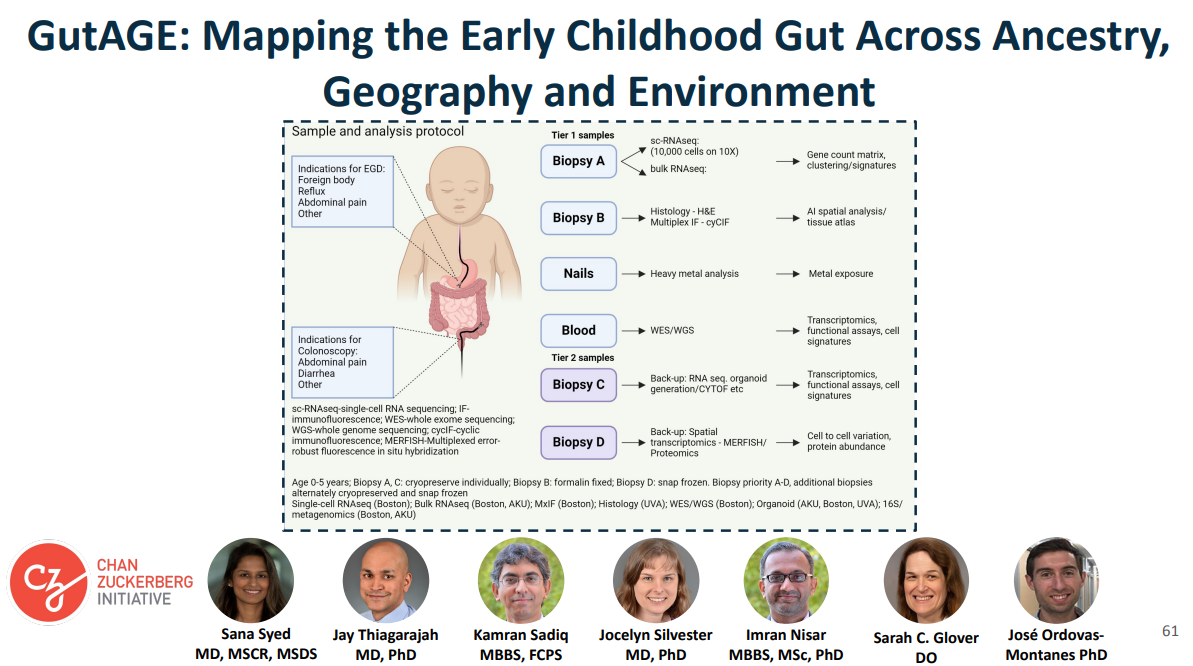
This is a quote from President Obama when his administration announced massive funding toward precision medicine in January of 2015, that the promise of precision medicine is ”delivering the right treatments at the right time, every time to the right person.” This figure illustrates some of the kinds of data that Dr. Syed had access to as faculty at UVA, including genomics, epigenome, transcriptomics, proteomics, metabolomics, etc.Shoda and colleagues, used a combination of histology data, endoscopic features, histologic and endoscopic scoring indices, and transcripts that make up the eosinophilic esophagitis diagnostic panel, a quantitative PCR assay with 96 EoE representative genes. The key message from all of those visualizations is that they found that EoE can be divided into three distinct endotypes after analyzing transcriptomics changes via partition-around-medoid clustering, a machine-learning method.In this project, the researcher intend to curate a novel metabolic network specific to the ileum, which is relevant to Crohn’s disease, link metabolic processes with Crohn’s disease phenotypes using in silico metabolic network modeling and ‘omics and characterize and target metabolic pathways in an organoid model generated from patient-derived Crohn’s disease tissue.In CoMPAS, the researchers aim to leverage artificial intelligence methods (AI) methods to build predictive models for CD using histology slides and single-cell RNA sequencing, allowing for risk stratification of B1 patients who will respond to anti-TNF therapyThe goal of our project is to create a multi-omics reference dataset with scRNA-seq data coupled with contextual data on tissue morphology, ancestry, social determinants of health, and the environment. The cohort for this study is enrolling patients who have clinical indications for endoscopy like foreign body removal, reflux, abdominal pain
My take: This work is necessary to identify the right treatments for each patient and will lead to better outcomes. We are already seeing the early stages of machine-learning’s impact on clinical care. In many other fields, AI work is much further along (especially in oncology). A recent study in Nature identified JAK inhibitors as potential life-saving therapy with toxic epidermal necrolysis (TEN).
Reference: Nordmann, T.M., Anderton, H., Hasegawa, A. et al. Spatial proteomics identifies JAKi as treatment for a lethal skin disease. Nature (2024). https://doi.org/10.1038/s41586-024-08061-0
Summary from Eric Topol (Ground Truths) focusing on spatial omics: Thierry Nordmann, Matthias Mann and their international consortium, used deep visual proteomics from 3μm PPFE sections of skin biopsies in patients affected by TEN…
More than 5,000 proteins were quantified from single cells—keratinocyte and immune cells—using mass spec, for the 4 different skin conditions (proteome cluster in Figure below, left panel). This led to the finding that the TEN patients had marked increased in Type 1 and 2 interferon signaling and activation of phosphorylated STAT1, which invoked the janus kinase (JAK/STAT) pathway. Subsequent steps were to test JAK inhibitors in cell culture (with live cell imaging) and in two different mouse models, all showing highly potent, dose-dependent impact on inhibition of the intense inflammatory process and disease severity…
They went on to treat seven patients at Fuian Medical University, the course of one patient shown below, treated with a JAKi on day 4 after diagnosis, and manifesting a marked response starting within 48 hours. All 7 patients fully resolved, with no side effects…
For spatial medicine, there are multiple analytical challenges that invoke the need for machine learning and A.I., including segmentation of cell types, automated capture of cells of microdissection, extracting useful information from the >5,000 proteins quantified per cell, and ultimately, as we’ll see more in the future, A.I. powering the construction of high-resolution 3D maps.
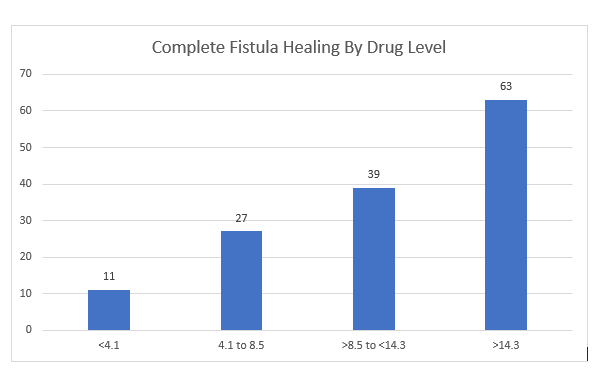
In this multicenter retrospective review with 183 patients, the adalimumab (ADM) levels were examined with respect to healing of perianal fistulas. Most patients (82%) had complex perianal fistulizing CD.
Key findings:
87 patients (48%) received intensified dosing at the time of therapeutic drug monitoring (TDM)
Patients with complete fistula healing (CFH) had higher median ADM levels: 12.9 compared to 6.1 for those witout CFH
“Optimal ADM concentration associated with CFH was 12.2 mcg/mL” which had positive predictive value of 64% and negative predictive value of 80%. Among those with ADM >12.1, CFH was achieved in 64% compared to 20.5% in those with concentrations <12.1 (Odds ratio, 5.7). “Even higher drug levels may be needed.”
There were 46 patients in each drug level category
My take: There is a lot of data supporting TDM, including proactive TDM, with anti-TNF agents like adalimumab and infliximab. This study shows that with fistulizing disease higher drug levels are needed to achieve better outcomes.
A Simard et al. J Pediatr Gastroenterol Nutr. 2024;79:800–806. Role of ileal diversion in pediatric inflammatory bowel disease
Indications:
Severe, medically refractory colitis
Complex and medically refractory perianal disease
In combination with bowel resection for irreversible bowel damage (e.g., fistulae, abscesses, or strictures)
Diversion “provides the opportunity to reduce steroid use, improve growth and observe the natural history of the disease in a more controlled manner. It may also enhance quality of life”
My take: This is a handy article when considering ileal diversion in a patient with medically-refractory inflammatory bowel disease.
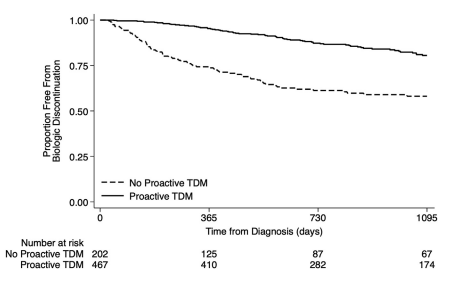
S Ali et al. Clinical Gastroenterology and Hepatology, Volume 22, Issue 10, 2075 – 2083.e1. Characterization of Biologic Discontinuation Among Pediatric Patients With Crohn’s Disease
Methods: Prospective ImproveCareNow registry data (n=823, from 7 centers) were supplemented with medical record abstraction.
Treatment/Monitoring:
86% started biologics (78% infliximab, 21% adalimumab, <1% others)
Twenty-six percent used concomitant immunomodulators for ≥12 months
Most (85%) measured TDM including 47% induction, 69% proactive, and 24% reactive
Key findings:
Twenty-nine percent discontinued their first biologic after median 793 days because of inefficacy (34%), anti-drug antibodies (8%), adverse events (8%), or non-adherence (12%)
Proactive TDM and concomitant immunomodulators were associated with 60% and 32% reduced biologic discontinuation
Half of patients discontinued biologics without trial of high-dose therapy and 14% without any evaluation
Among patients started with infliximab therapy, 62% of patients started at a dose of <6 mg/kg, 18% stared at a dose >8 mg/kg. 67% of patients underwent dose escalation. This is agreement with other studies indicating that as many as 80% of children need doses in excess of ‘standard’ dosing (5 mg/kg every 8 weeks)
In patients with anti-TNF medication inefficacy with TDM availability, 36% had infliximab or adalimumab levels below 5 mcg/mL. and 20% had levels between 6-8 mcg/mL.
Among patients who discontinued anti-TNF medications, 60% had serum trough levels less than 10 mcg/mL.
The rate of biologic durability was lower for those (n=61) receiving a 2nd biologic who had rates of remaining on agent of 56% at 1 yr, 28% at 2 yrs, and 10% at 4 yrs. In contrast, the first biologic had durability of 90% at 1 year, 79% at 2 years, and 66% at 4 yrs.
My take: This study strongly supports the use of proactive therapeutic drug monitoring. In addition, the authors make a compelling argument to optimize a therapy and evaluate carefully before switching to a new medication/biologic. Finally, the use of concomitant immunomodulators can improve medication durability; it is particularly important if needing to switch from one anti-TNF agent to another due to anti-drug antibodies.
Background: “Placebo-controlled trials are especially important during the early phases of drug development, as use of placebo aids early detection of efficacy or futility.”
Methods: The authors performed a systematic review which identified 47 trials including 20,987 patients (14 267 [68·0%] receiving active drug and 6720 [32·0%] receiving placebo) were eligible. The studies involved multiple RCTs of biologics and small molecules in IBD.
Key findings:
The risks of worsening of IBD activity (Active treatment vs placebo: 563/13,473 [4·2%] vs 530/6252 [8·5%];RR 0·48)
Withdrawal due to adverse event (Active treatment vs placebo: 401/13 363 [3·0%] vs 299/6267 [4·8%]; RR 0·62)
Serious adverse event (Active treatment vs placebo: 682/14,267 [4·8%] vs 483/6720 [7·2%]; RR 0·69)
Serious infection (Active treatment vs placebo: 140/14 ,194 [1·0%] vs 91/6647 [1·4%]; RR 0·67)
Serious worsening of IBD activity (Active treatment vs placebo: 187/11,271 [1·7%] vs 189/5056 [3·7%]; RR 0·4)
VTEs (Active treatment vs placebo: 13/7542 [0·2%] vs 12/2981 [0·4%]; RR 0·45)
All of these adverse outcomes were significantly lower with active drug than placebo.
My take: Now that there are proven medications that are effective for moderate-to-severe Crohn’s disease, head-to-head trials of novel drugs against existing drugs with proven efficacy, rather than placebo-controlled trials, should be prioritized.
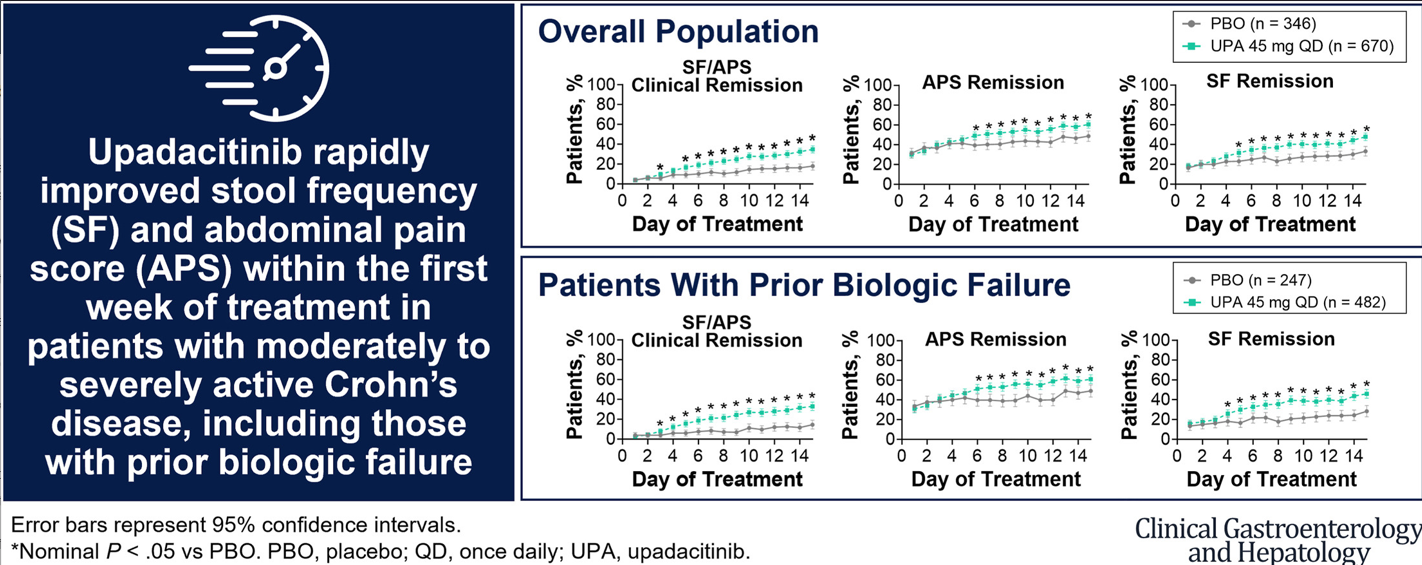
This study was a post hoc analysis included pooled data from 2 phase 3, multicenter, double-blind, 12-week induction trials (U-EXCEL and U-EXCEED) and 1 maintenance trial (U-ENDURE). The study included 1021 patients with Crohn’s disease (CD) (n = 674 UPA45; n = 347 PBO).
Key findings:
Upadacitinib 45 mg taken once daily resulted in rapid relief from CD symptoms within 5 to 6 days of treatment initiation and improved clinical outcomes starting at week 2.
The present analysis demonstrates symptomatic relief as early as day 5 to 6 for patients receiving UPA, with 16.7% of patients experiencing daily SF/APS clinical remission by day 5.
The first achievement of daily stool frequency/abdominal pain score (SF/APS) clinical remission occurred earlier with UPA45 (median, 13 d) vs PBO (median, 32 d)
Patients treated with UPA45 showed improved rates of SF/APS clinical remission (21.1% UPA45 vs 8.9% PBO) and clinical response (58.8% UPA45 vs 37.9% PBO) starting at week 2 (both P ≤ .01).
In their discussion, the authors note that time to response to treatment with upadacitinib compares favorably to other advanced therapies:
“Vedolizumab resulted in symptomatic improvement within 2 to 4 weeks of treatment initiation16; ustekinumab led to clinical response and remission at week 3 or 6, depending on the dose.17 Similarly, of the time points analyzed, clinical response and/or clinical remission was observed as early as week 2 for risankizumab, 5 infliximab,18 and certolizumab pegol,19 and as early as week 1 for adalimumab.20,21“
My take: The rapid response seen in many patients indicate that upadacitinib can be a steroid-sparing therapy in patients with Crohn’s disease.
Key findings: Among the 975 patients with moderate to severe ulcerative colitis, analyzed in the induction trial, 1200 mg of risankizumab significantly increased the rates of clinical remission at 12-week follow-up compared with placebo (20.3% vs 6.2%, respectively). Among 548 patients included in the primary efficacy analysis for the maintenance trial, 180 mg of risankizumab and 360 mg of risankizumab significantly increased the rates of clinical remission (40.2% and 37.6%, respectively) compared with placebo (25.1%).
D Turner et al. JPGN 2024; 79:315–324. Ustekinumab in paediatric patients with moderately to severely active Crohn’s disease: UniStar study long-term extension results
Dosing: “Patients were randomised 1:1 and stratified by body weight (<40 or ≥40 kg) to receive a single induction dose of lower- or higher-dose IV ustekinumab (lower dose: 3 mg/kg [<40 kg] and 130 mg [≥40 kg]; higher dose: 9 mg/kg [<40 kg] and 390 mg [≥40 kg]). Doses specified as higher were selected to deliver ustekinumab exposure comparable to a reference adult population with CD.7, 12 At Week 8, patients received a single SC maintenance dose of ustekinumab (2 mg/kg [<40 kg]; 90 mg [≥40 kg]).”
Key findings:
Of the 34 patients who entered the LTE, 25 patients with evaluable data completed Week 48, and 41.2% (14/34) achieved clinical remission at Week 48
Efficacy and PK through 1 year in ustekinumab-treated paediatric patients were comparable to those previously reported in adults. No new safety or immunogenicity signals were reported through 4 years of ustekinumab treatment.
My take (borrowed in part from authors): “Overall, long-term data support the SC dose regimens of 90 mg as maintenance therapy for the treatment of CD for a paediatric population with ≥40 kg body weight. A phase 3 study of ustekinumab (ClinicalTrials.gov Identifier: NCT04673357) is ongoing to further evaluate dose regimens for paediatric patients <40 kg and ≥40 kg.” This type of data is essential to support the use of advanced therapies like ustekinumab until they receive specific regulatory approval for children (often 8-10 years after approval in adults).
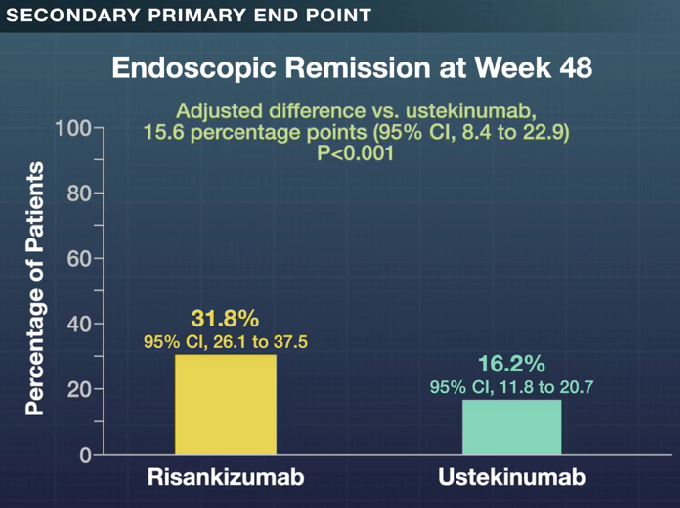
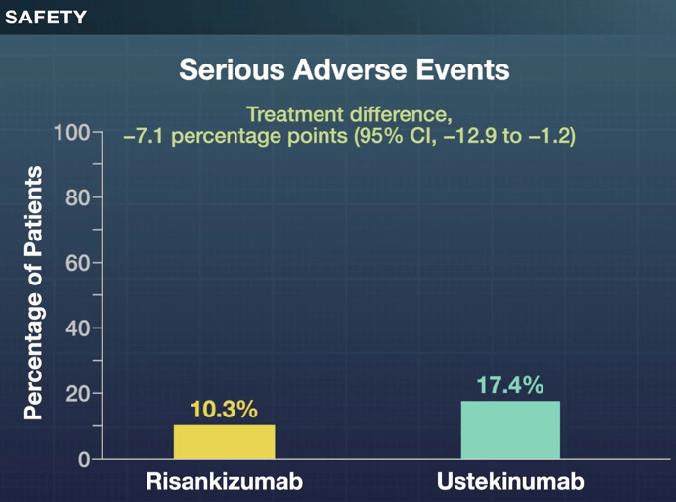
L Peyrin-Biroulet et al. NEJM 2024; 391:213-223. Risankizumab versus Ustekinumab for Moderate-to-Severe Crohn’s Disease
Background: “Interleukin-23 is a heterodimeric proinflammatory cytokine comprising a p40 subunit shared with interleukin-12 and a unique p19 subunit that plays a key role in skin, joint, and gastrointestinal inflammation.16 Ustekinumab and risankizumab are humanized IgG1 monoclonal antibodies; ustekinumab selectively binds p40, and risankizumab selectively binds p19…In head-to-head trials directly comparing their efficacy in psoriasis, risankizumab was superior to ustekinumab, which suggests greater efficacy with p19 blockade than with p40 blockade.”
This “SEQUENCE” trial was a phase 3b, multicenter, open-label, randomized controlled trial with 527 patients with moderate-to-severe Crohn’s disease who either had an inadequate response or had intolerance to anti-TNF agents, received either risankizumab or ustekinumab.
Key Findings:
A higher percentage of patients in the risankizumab group than in the ustekinumab group completed all the assigned treatment (90.2% [230 of 255 patients] vs. 72.8% [193 of 265 patients]). The primary reason for discontinuation of risankizumab was an adverse event (3.1% [8 of 255 patients]), and the primary reason for discontinuation of ustekinumab was lack of efficacy (13.2% [35 of 265 patients]
Clinical remission at 48 weeks was 60.8% with risankizumab and 40.8%% with ustekinumab (P<0.001); there were similar rates of glucocorticoid-free clinical remission, 60.8% vs 40.4% respectively. Endoscopic response at 48 weeks was 45.1% and 21.9% respectively.
My take: These head-to-head results showed the superiority of risankizumab over ustekinumab across numerous clinical and endoscopic end points, including glucocorticoid-free clinical remission and endoscopic remission. However, it is still concerning to me that endoscopic remission rates were only 32% at 1 year and that less than half had an endoscopic response.