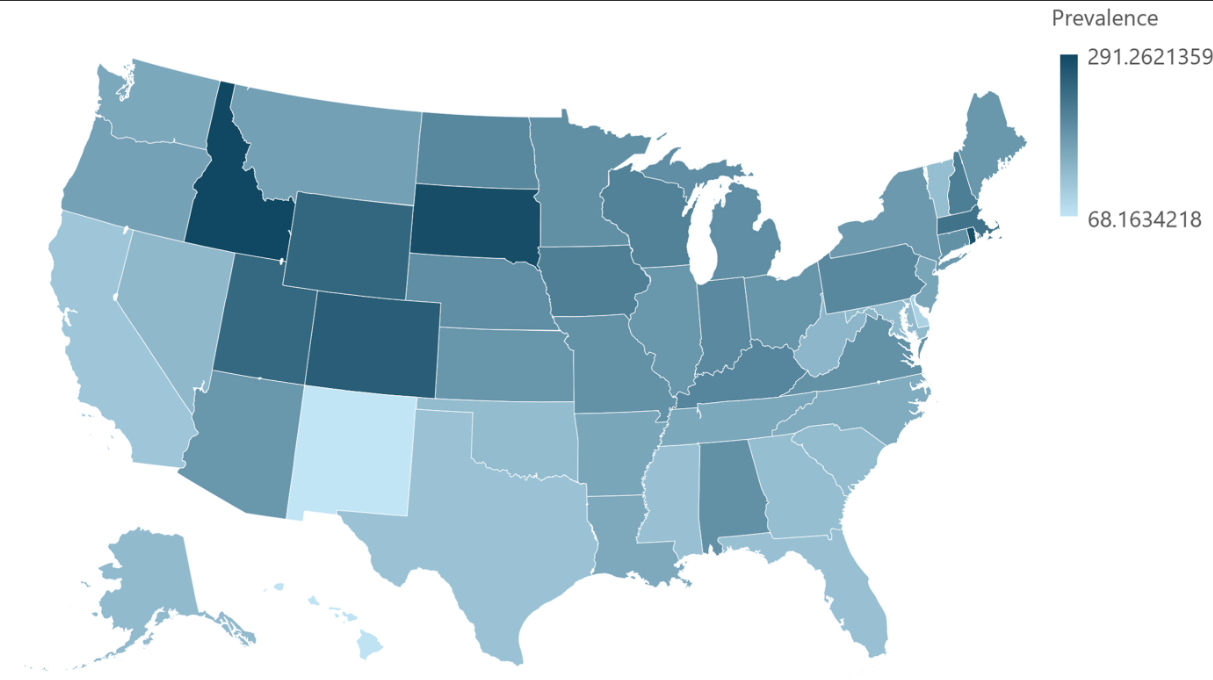
P Visaggi, ES Dellon. Gastroenterology 2026;170:476–494. Open Access! Epidemiology, Natural History, and Treatment of Eosinophilic Gastrointestinal Diseases
Diagnosis:
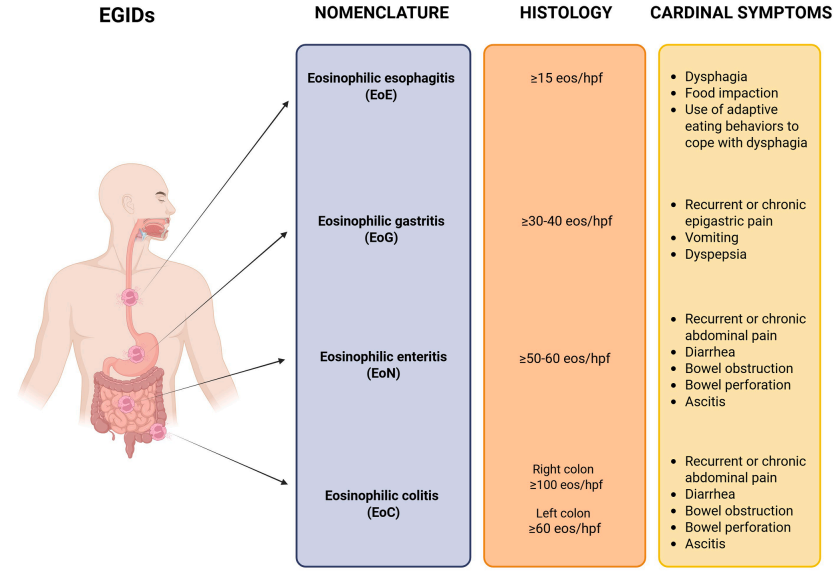
- EoE is diagnosed in the setting of symptoms of esophageal dysfunction, demonstration of at
least 15 eosinophils per high-power field (eos/hpf) on esophageal biopsy, and exclusion of competing causes of esophageal eosinophilia. At the time of diagnosis, disease severity can be assessed with the Index of Severity for EoE (I-SEE) - Non-EoE EGIDs: the diagnostic process is more challenging and pediatric diagnostic guidelines were only published in 2024…biopsy specimen shows pathologically elevated
levels of GI tract eosinophils, and other conditions that cause GI eosinophilia are excluded…Symptoms are nonspecific, multiple conditions could explain extraesophageal eosinophilia, inflammation can involve muscular and serosal layers rather than mucosal,
Treatment:
- EoE: PPIs, Swallowed topical corticosteroids, Monoclonal antibodies and food elimination dets
- Non-EoE EGIDs: “The management of non-EoE EGIDs is challenging due to lack of established end points, validated outcomes, and of successful RCTs leading to approved treatments. Accordingly, management of non-EoE EGIDs is currently based on low-quality evidence.” Main treatments: corticosteroids (prednisone or budesonide), food elimination diets, and monoclonal antibodies (eg. dupilumab). “The use of PPIs, mast cell stabilizers, leukotriene inhibitors, and immunomodulators for non-EoE EGIDs has been reported,
with variable results.”
My take: This is a useful review with a number of pointers for epidemiology, natural history, evaluation and management of EoE and Non-EoE EGIDs.
Related blog posts:
- Updated Nomenclature for Eosinophilic Gastrointestinal Diseases
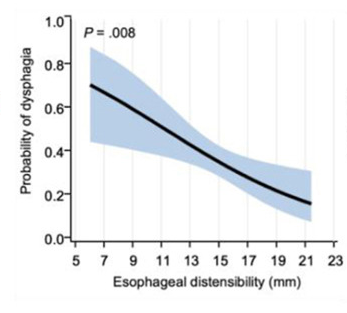
- The Esophagus Works Better After Responding to Treatment for Eosinophilic Esophagitis
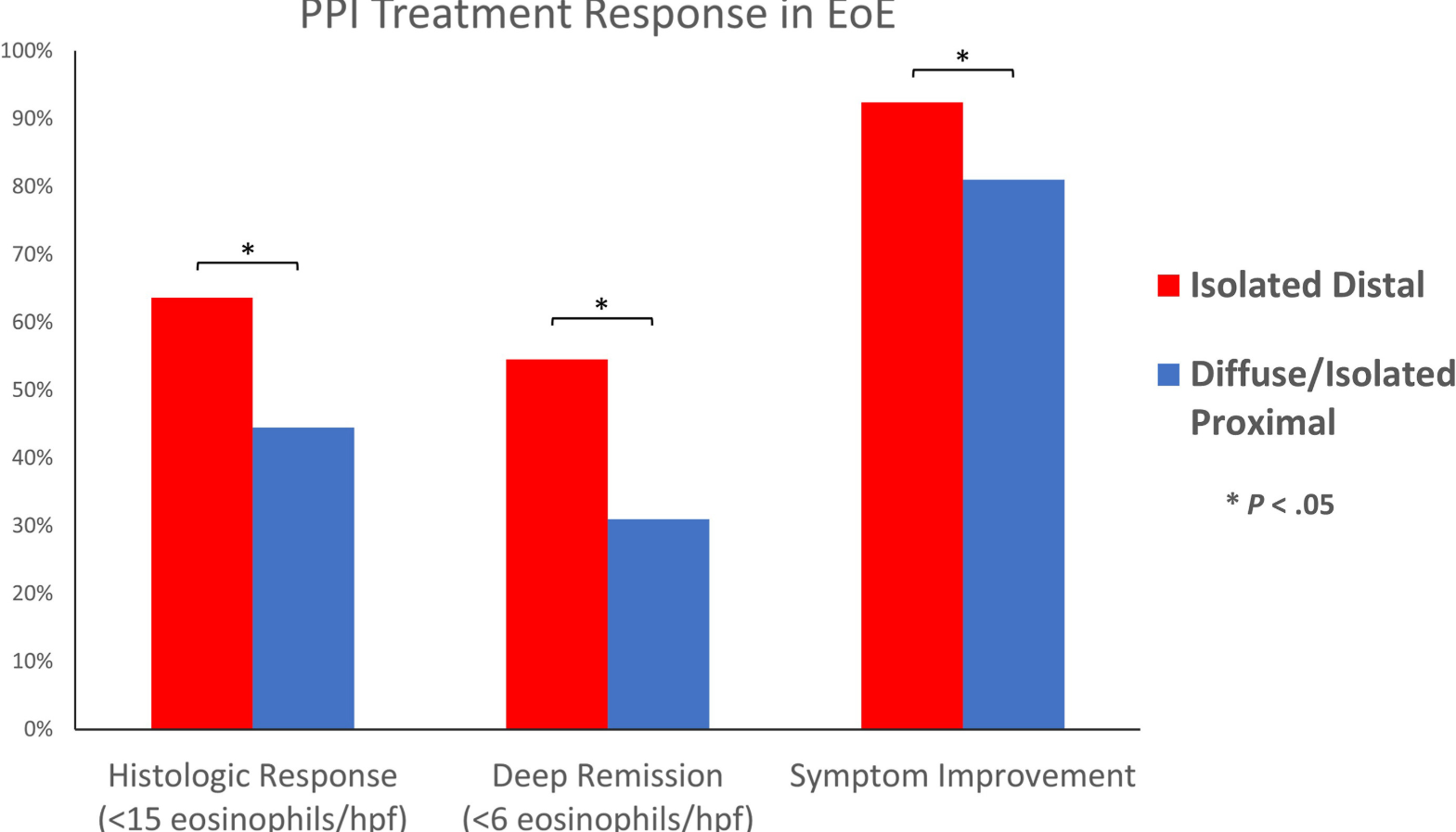
- Updated Data on PPI Effectiveness For Eosinophilic Esophagitis
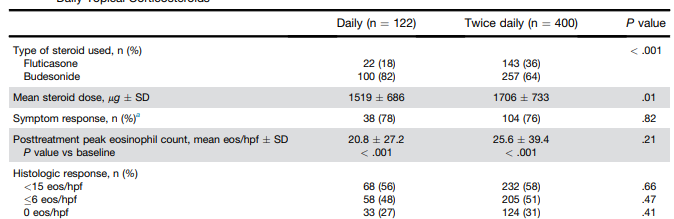
- Eosinophilic Esophagitis: Once vs Twice Daily Steroid Treatment
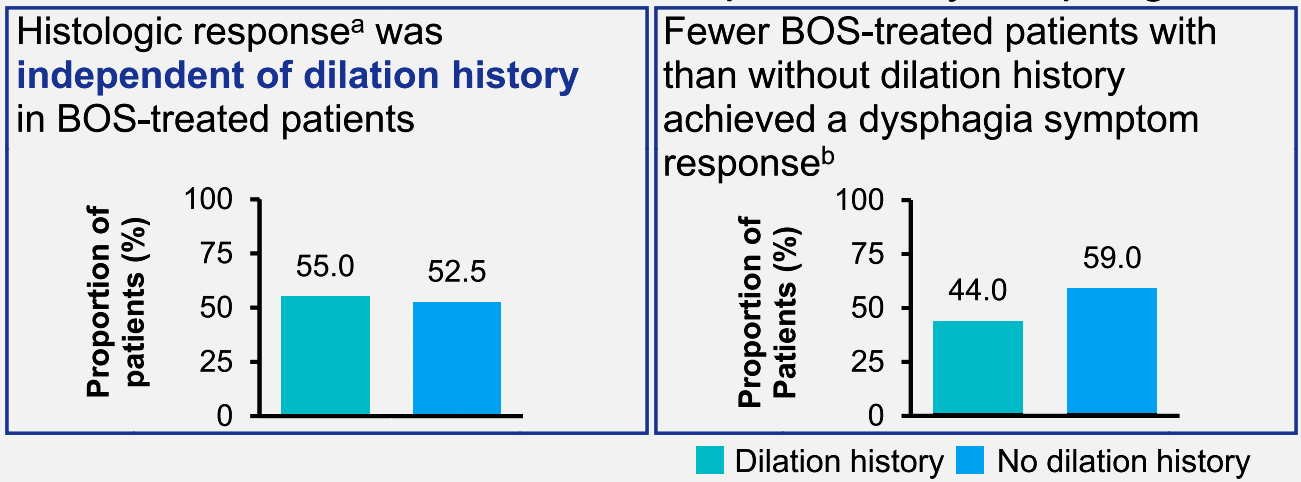
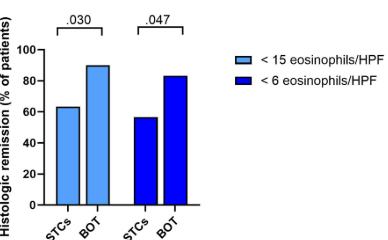
- Is Topical Budesonide Less Effective in Patients With Eosinophilic Esophagitis With Strictures?
- Eosinophilic Colitis Is Not a Typical EGID or IBD
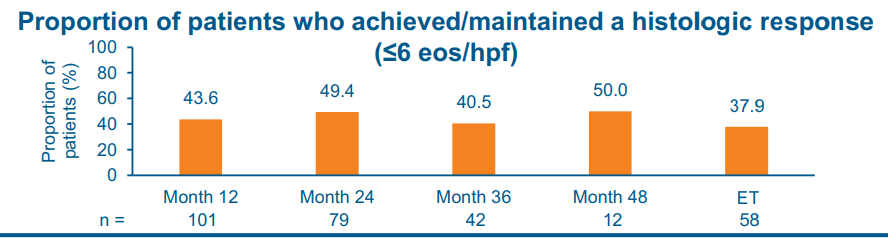
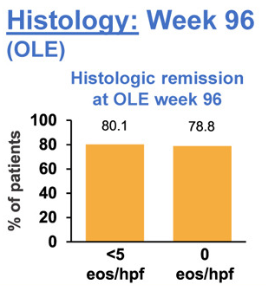
- Long-Term Treatment of Eosinophilic Esophagitis with Budesonide
- ESPGHAN Eosinophilic Esophagitis Guidelines
- How Closely Related Are Eosinophilic Gastrointestinal Disorders To Isolated Eosinophilic Esophagitis