A Mathur. Liver Transplantation 2023; 29: 465-466. Open Access! Salvaging the fatty liver for transplant: is short duration NMP enough? (ed)
“As of 2020, the Center for Disease Control (CDC) notes that 40% of the ~258 million US adults suffer from obesity. This represents just more than a 100 million people suffering from obesity. In addition, about 23 million people suffer from severe obesity with a body mass index >40 kg/m2.” Fatty liver disease (aka NAFLD), driven primarily by obesity, is a leading cause of liver transplantation. In addition, fatty liver disease is impacting the ability to treat liver failure.
“The end result of this epidemic is that we are identifying a greater proportion of organ donors with varying degrees of liver steatosis. Transplantation of steatotic livers is associated with an increased degree of ischemia-reperfusion injury (IRI) and release of inflammatory cytokines from the graft. The consequences of this can range from severe reperfusion syndromes with immediate vasoplegia and circulatory collapse to distant organ dysfunction with acute kidney injury, liver allograft dysfunction, and primary nonfunction (PNF).”
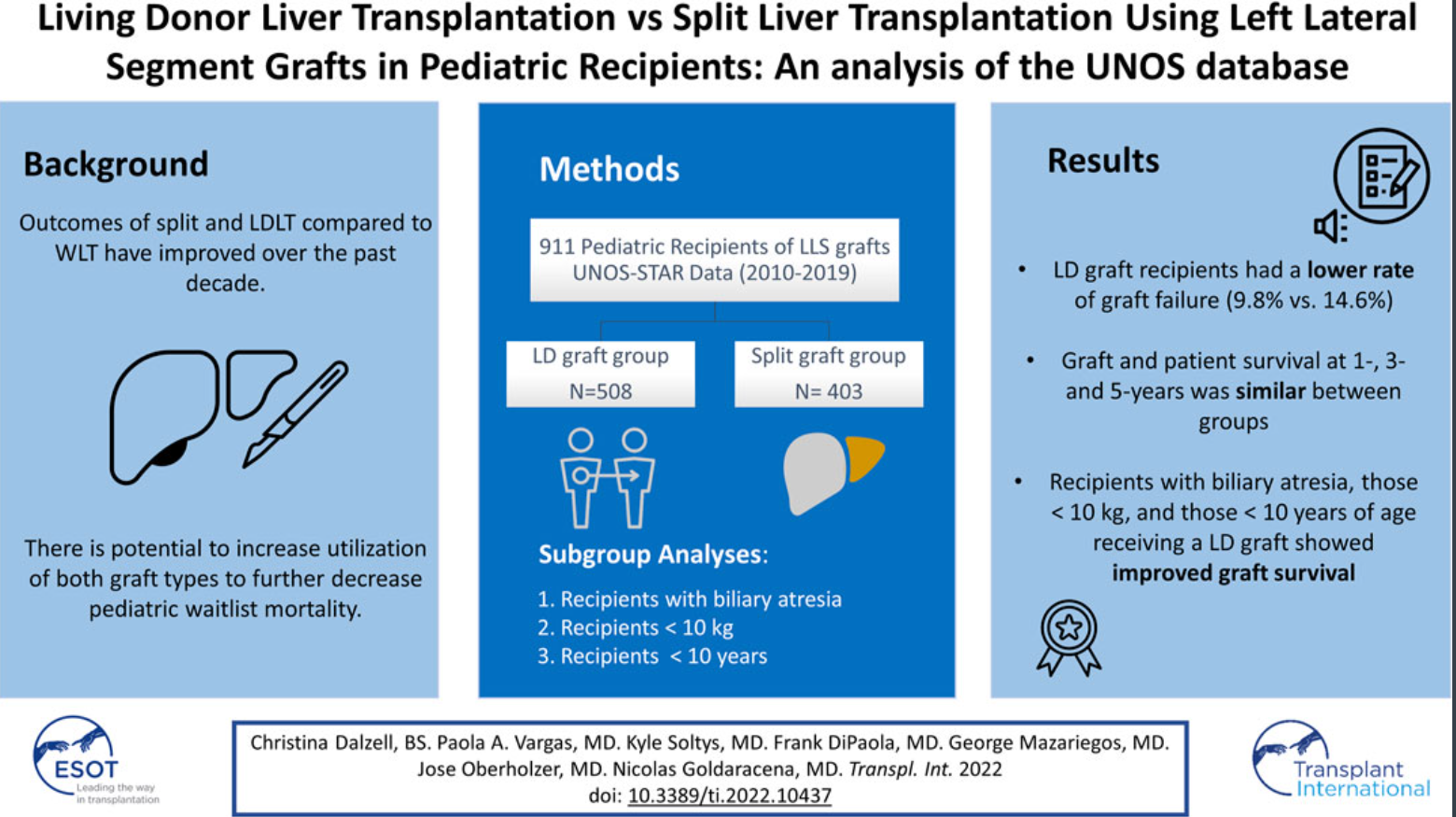
In order to try to identify suitable liver organs for transplantation, researchers are trying to identify strategies to utilize steatotic grafts safely. Patrono et al (Liver Transplantation 2023; 29: 508-502) examined the feasibility of using normothermic machine perfusion (NMP) in the setting of macrovesicular steatosis (MaS) ≥30%. They identified 10 patients who had liver transplants using NMP in patients with MaS ≥30%; 4 additional organs were not used despite NMP. 8 of 10 patients showed good liver function, representing 57% (8 of 14) of NMP fatty organs.
Another study in the same issue (NB Ha et al. Liver Transplantation 2023; 29: 476-484) showed that patients with sarcopenic obesity (=low muscle mass obesity) had high waitlist mortality of 40% compared to 21% and 12% for those with sarcopenia without obesity and for those with obesity without sarcopenia, respectively.
My take: Obesity increases the risk of fatty liver associated cirrhosis/liver failure, and is impacting the availability of suitable organs for those in need. Furthermore, in those with obesity, the presence of sarcopenia increases the risk of death on transplant waitlist.
- Related blog posts:
How Successful is Liver Transplantation for Fatty Liver Disease? - Online Aspen Webinar (Part 6) -NAFLD and NASH
- NAFLD Guidance from American Association for the Study of Liver Diseases
- Trends in Liver Diseases: Autoimmune Liver Diseases and Fatty Liver
- Liver Shorts July 2020
- Sarcopenia, fatigue, and nutrition in chronic liver disease
- “More to It Than Meets the BMI”

Tucson Botanical Gardens