While issues with nutrition are ubiquitous, among the three areas of expertise for pediatric gastroenterologists (gastroenterology, hepatology, and nutrition), it does seem that nutrition expertise receives the least interest overall. One effort to work on this is Nutrition University (N2U) sponsored by NASPGHAN/NASPGHAN foundation.
This is the first year in which the program has been opened up to physicians who have been in practice for more than 10 years and I am looking forward to a great review. Prior to attending, the participants were asked to review previous N2U modules which are available at NASPGHAN website: 2012 N2U Course ( a good source for CME as well).
This year’s syllabus: 2015 N2U Syllabus & Presentations (posted with permission from course organizers).
Last night the meeting started off with some comments by Praveen Goday (Praveen’s training in Cincinnati overlapped with mine) who has spearheaded this effort; subsequently the faculty addressed previously submitted attendee questions.
Here’s a sampling:
Should we be recommending a low FODMAPs diet for IBS? Rob Shulman indicated that about ~70% of adults responded in one study and that a similar study in children at Baylor College of Medicine produced similar results. However, the diet is difficult and help from a dietician/nutritionist is needed. If there is not a response in 7-10 days, then it is likely to be ineffective.
What should be the first formula for Cow’s Milk allergy/intolerance in infancy? The recommendation for most infants (not the very sickest) was to start with a hydrolysate formula which should be effective in more than 90%. It was suggested that amino acid based formulas be reserved for hospitalized infants and those who do not respond to hydrolysates.
What about fish oil enterally or parenterally? James Heubi(*) noted that a lot more data is needed but fish oil either enterally or parenterally may be beneficial. Rob Shulman commented that recent work indicates that vitamin E may be an important reason why fish oil could be better than soy-based lipid emulsions.
How practical are blenderized diets for gastrostomy fed children? Catherine Karls noted that the general goal is to provide nutrients which mimic the commercial formulas but there are many important caveats for DIY (do-it-yourself formula).
- An RD needs to supervise to assure all micronutrient needs are being met. Using computer programs, this facilitates calculating dietary reference intakes (DRIs).
- Many parents prefer as homebrews are perceived as more natural or holistic
- Some children have better tolerance (eg. volume-sensitive, patients with retching)
- Drawbacks: time commitment, additional costs (though may be cheaper for some), and concerns regarding food safety
- Homebrews are not recommended for jejunostomy feeds (gastrostomy only) or for those with small-caliber feeding tubes (needs to be at least 14 Fr)
- Don’t use without the assistance of an RD!
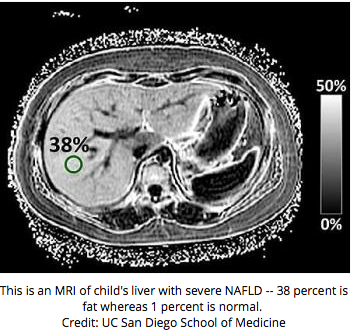
Which is better for NAFLD -low carb or low fat? Ann Scheimann stated that this question is misleading –it is a lot more complicated. It depends on the carbs and it depends on the fat. Fructose clearly worsens NAFLD but so does a diet high in animal fat.
What are the nutritional management recommendations for acute pancreatitis? Justine Turner indicated that too many centers continue to rely on parenteral nutrition. Yet, guidelines recommend the use of enteral nutrition due to lower risk of poor outcomes (eg. infections when NPO and on parenteral nutrition). ‘Resting pancreas is not helpful.’ With acute pancreatitis, enzyme secretion is reduced. Her approach is to start nasogastric (NG) feedings at about 24 hours after presentation, as long as hemodynamically stable. She indicated that nasojejunal (NJ) feedings can be done if NG is not well-tolerated. NJ feedings are effective at reducing enzyme secretion. However, Praveen Goday stated that his practice was often starting with NJ feeds. “Sometimes there is only one shot” before the ICU team starts HAL. Both physicians indicated that polymeric formulas were probably acceptable; however, starting with semi-elemental or elemental feedings are often done, again as a practical matter to minimize the likelihood of reverting to parenteral nutrition.
What is the advice regarding children who need far less than typical calories for weight (eg. wheelchair-bound inactive child)? Generally all nutrients are being met if a child less than 10 years is receiving 4 cans of commercial formula. For children 10 and older, receiving 6 cans per day should ensure adequate nutrients. For those who fall below this threshold, several options:
- Reduced calorie formula (eg. Pediasure Sidekicks, Compleat Reduced) are approximately 0.6 cal/mL but have all the other nutrients
- Supplementation: multivitamin, calcium, phosphorus, protein
- Need to meet at least 80% of typical fluid needs, thus not much rationale for 2 cal/mL formulas. As a practical matter, if the child is urinating well, they are receiving enough fluids.
*I was fortunate to have Jim as an attending during my fellowship at Cincinnati. In fact, even before then, Jim interviewed me when I was considering Cincinnati for my pediatric residency. He is a terrific person and amazing to work with.
Disclaimer: This blog entry has abbreviated/summarized this presentation. Though not intentional, some important material is likely to have been omitted; in addition, transcription errors are possible as well.
These blog posts are for educational purposes only. Specific dosing of medications/diets (along with potential adverse effects) should be confirmed by prescribing physician/nutritionist. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.