GI and Hepatology News, Open Access: Watershed Moment’: Semaglutide Shown to Be Effective in MASH (November 2024): “At 72 weeks, a 2.4-mg once-weekly subcutaneous dose of semaglutide demonstrated superiority, compared with placebo, for the two primary endpoints: Resolution of steatohepatitis with no worsening of fibrosis and improvement in liver fibrosis with no worsening of steatohepatitis.”
“ESSENCE (NCT04822181) is an ongoing multicenter, phase 3 randomized, double-blind, placebo-controlled outcome trial studying semaglutide for the potential treatment of MASH.” Cohort: N=1200, biopsy-defined MASH and fibrosis, stages F2 and F3…”After initiation, the semaglutide dosage was increased every 4 weeks up to 16 weeks when the full dose (2.4 mg) was reached.”
Key findings:
62.9% of those in the semaglutide group and 34.1% of those in the placebo group reached resolution of steatohepatitis with no worsening of fibrosis.
37% of those in the semaglutide group and 22.5% of those in the placebo group had improvement in liver fibrosis with no worsening of steatohepatitis
Weight loss was also significant, with a 10.5% reduction in the semaglutide group compared with a 2% reduction in the placebo group
No new safety signals were identified
Cardiometabolic risk factors improved as well, with changes in blood pressure measurements, hemoglobin A1c scores, and cholesterol values.
20%-40% improvements in liver enzymes and noninvasive fibrosis markers, such as ELF and vibration-controlled transient elastography liver stiffness.
My take: This expected finding indicates that more GLP-1 agents are likely to be approved for MASH treatment. Survodutide received “U.S. FDA Breakthrough Therapy” in October 2024.
The researchers found a 25.6% drop in people undergoing bariatric surgery in the final six months of 2023 compared with the number of surgeries people had during the same period the year before. During the latter half of 2023, the number of patients who took a glucagon-like peptide 1, or GLP-1 medication for weight loss, surged by more than 130%, according to a study published Friday in JAMA Network Open…Another popular weight loss drug, Eli Lilly’s Zepbound, was not included because the Food and Drug Administration did not approve it until November 2023…[And there are] anecdotal reports of hospitals that shut down bariatric surgery programs as the number of patients seeking operations slumped…
In 2022, nearly 280,000 metabolic and bariatric procedures were performed in the United States, according to the American Society for Metabolic and Bariatric Surgery. That represented about 1% of all U.S. residents eligible for weight loss operations…The CDC estimates that about 40% of U.S. residents have obesity and 1 in 10 have severe obesity.
Reference: Lin, K., et al. (2024). Metabolic Bariatric Surgery in the Era of GLP-1 Receptor Agonists for Obesity Management. JAMA Network Open. doi.org/10.1001/jamanetworkopen.2024.41380.
Methods: This cross-sectional study, we used 2022 to 2023 deidentified claims from 17 million unique deidentified adult patients with medical and pharmaceutical coverage through commercial and Medicare Advantage insurance in the OptumLabs Data Warehouse. We included only patients without diabetes and with obesity.
**Only 6% of patients with obesity in the study population received either GLP-1 drugs or surgery, suggesting that many more patients could be receiving treatment.
My take: The GLP-1 drugs have established a medical therapy with a good probability of effectiveness. This was lacking from prior medical treatments. It certainly is logical that their availability could reduce the use of bariatric surgery. The AAP may need to revise their bariatric surgery recommendations from 2020.
“The 17,604-patient trial tested Wegovy not for weight loss but for its heart protective benefits for overweight and obese patients who had preexisting heart disease but not diabetes. Participants were not required to track diet and exercise because it was not an obesity study…”
“Patients in the trial, called Select, lost an average of nearly 10% of their total body weight after 65 weeks on Wegovy. That percentage weight-loss was roughly sustained year-on-year until the end of about four years, where weight loss stood at 10.2%…”
“A third new analysis on Select published by Novo on Tuesday showed that the heart protective benefits of Wegovy to patients in the trial occurred regardless of their weight before starting on the drug and regardless of how much weight they lose on it.”
“The weight loss in the heart trial was less than the average of 15% weight loss in earlier Wegovy obesity studies”
“GLP-1 RAs (eg, semaglutide, tirzepatide, exenatide, liraglutide, albiglutide, dulaglutide, and lixisneatide) mimic incretins, which are hormones released after eating that prompt glucose-dependent insulin release from the pancreatic islets, stimulate satiety centers, inhibit glucagon release, and result in diminished gastric emptying.”
Because GLP-1 RAs diminish gastric emptying, they can increase the risk of residual gastric contents prior to surgery and endoscopy.
AGA Recommendations:
“If patients taking GLP-1 RAs solely for weight loss can be identified beforehand, a dose of the medication could be withheld before endoscopy with likely little harm, although this should not be considered mandatory or evidence-based. Nevertheless, it is unclear if withholding the medication for only one dose would be reliably adequate for an individual’s gastric motility to return to normal. ..there is insufficient evidence to suggest this practice be performed for patients taking these medications to treat diabetes”
“Generally, in patients on GLP-1 RAs who have followed standard perioperative procedures (typically an 8-hour solid-food fast and a 2-hour liquid fast) and who do not have symptoms of nausea, vomiting, dyspepsia, or abdominal distention, we advise proceeding with upper and/or lower endoscopy.”
“When possible, placing patients on a liquid diet the day before sedated procedures may be a more acceptable strategy, in lieu of stopping GLP-1 RAs.”
My take: This guidance provides useful advice given the increasing use of GLP-1 RAs. If these medications are being used for obesity, holding a dose prior to endoscopy is a good idea.
Related article: S Sen et al. JAMA Surgery 2024; doi:10.1001/jamasurg.2024.0111.Glucagon-Like Peptide-1 Receptor Agonist Use and Residual Gastric Content Before AnesthesiaKey finding: Use of a GLP-1 RA was independently associated with increased residual gastric content (1.5 mL/kg of clear liquids on gastric ultrasonography) on preprocedural gastric ultrasonography: 56% (35 of 62) in patients with GLP-1 RA use (exposure group) compared with 19% (12 of 62) in patients who were not taking a GLP-1 RA drug (control group).
This is at the entrance to the Westside Reservoir Park. I had the chance to go there as part of a Westside Beltline Tour in Atlanta.This reservoir is as deep as the Statue of Liberty is tall and can hold 2.4 billion gallons of water for the city of Atlanta
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
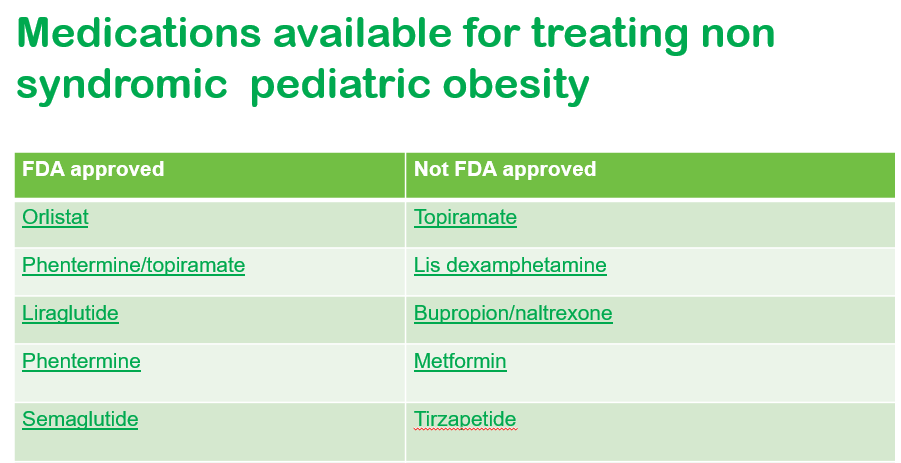
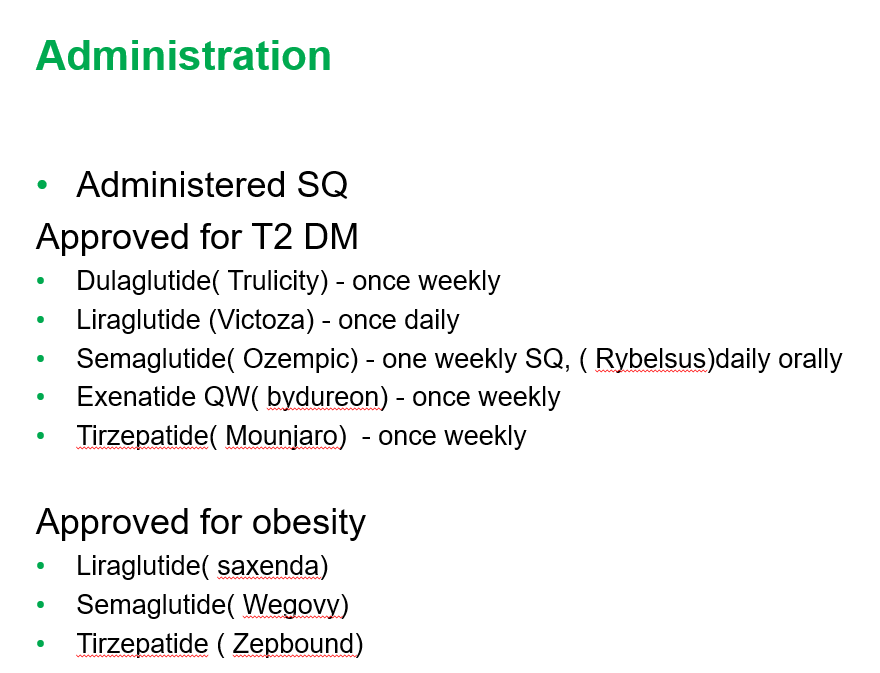
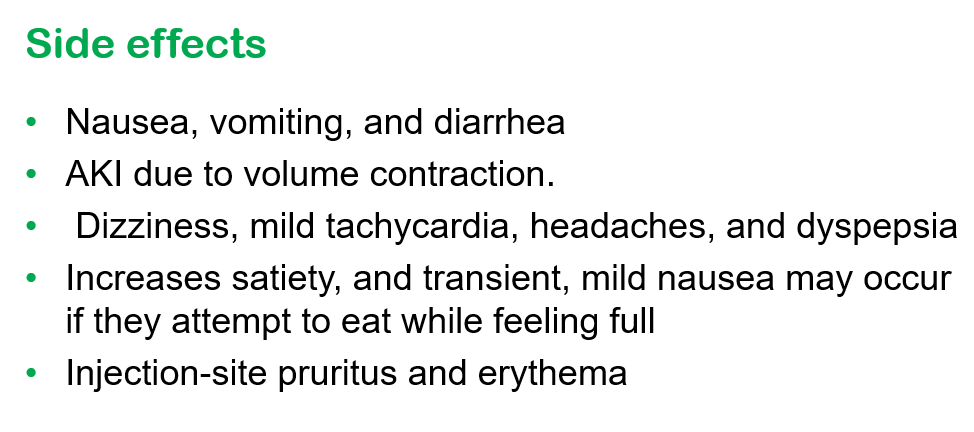
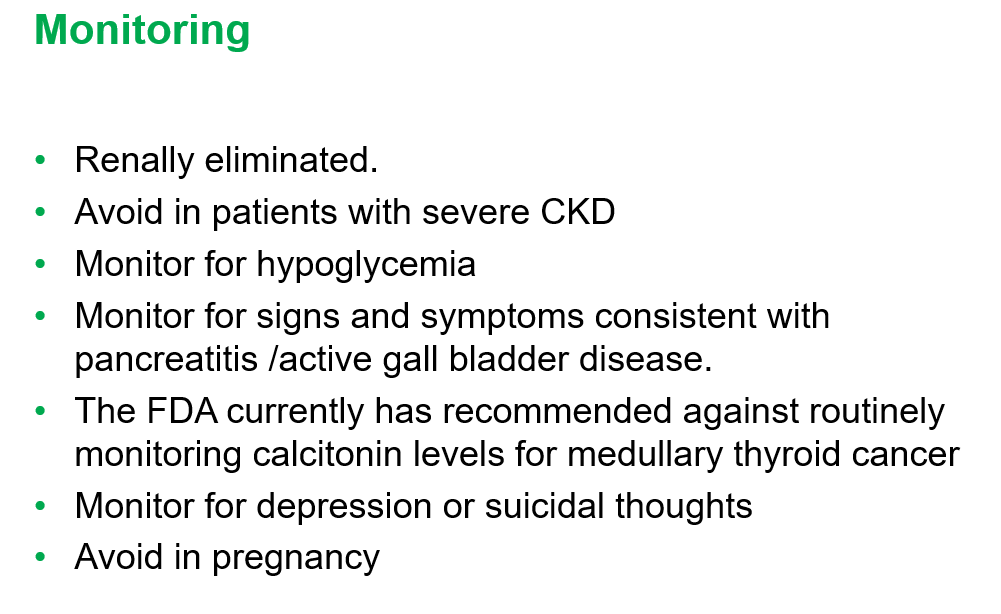
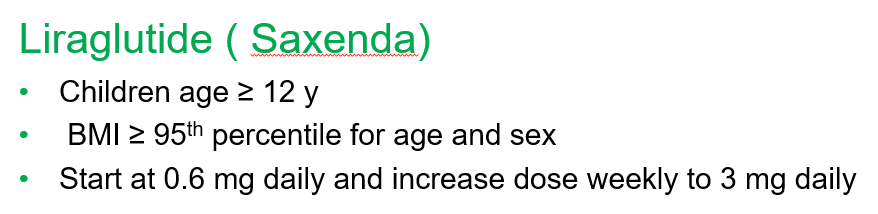
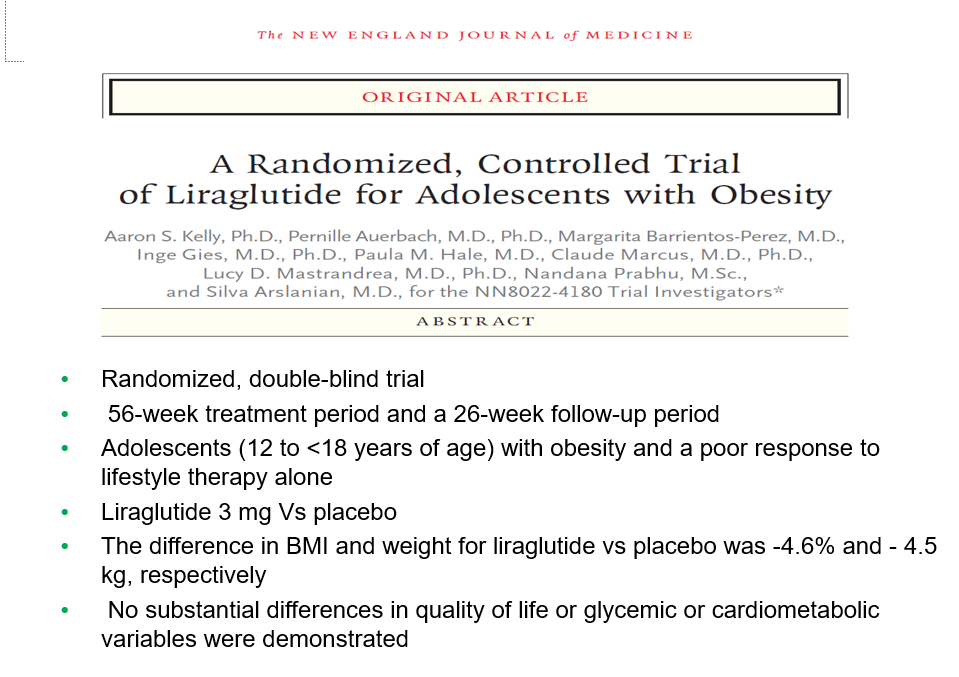
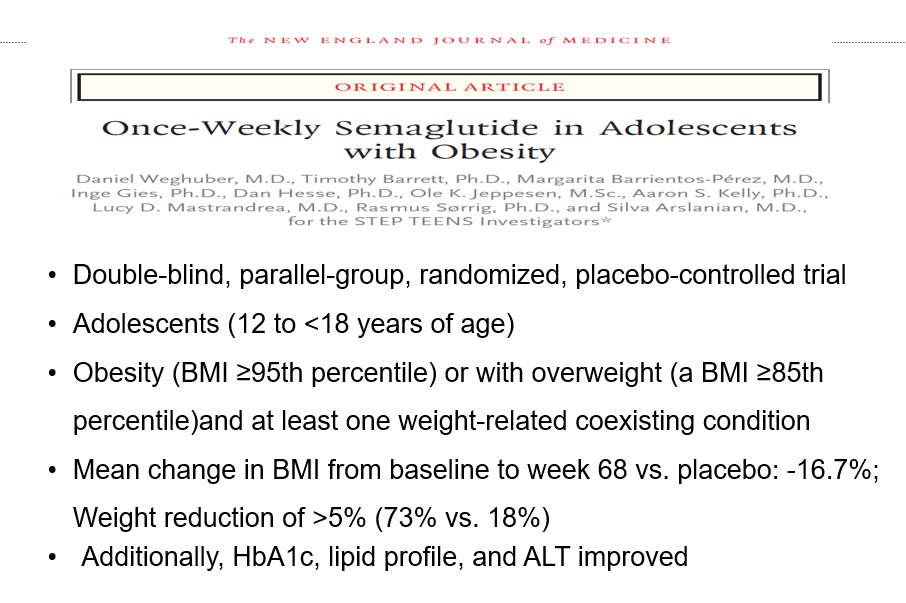
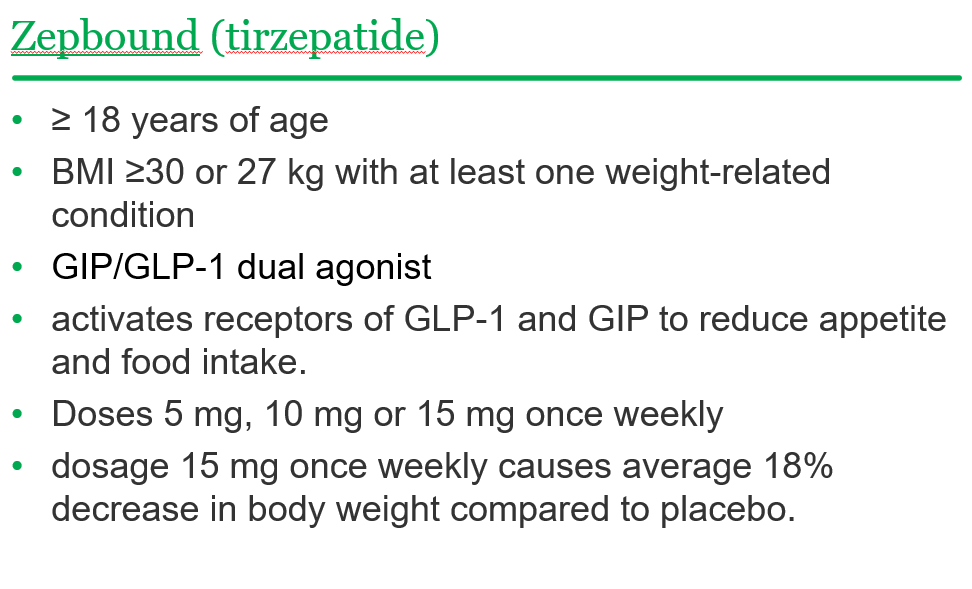
Recently, Dr. Shruthi Arora, an Emory Pediatric Endocrinologist and part of CHOA’s Strong4Life team, provided a terrific review of pediatric obesity pharmacology for our group.
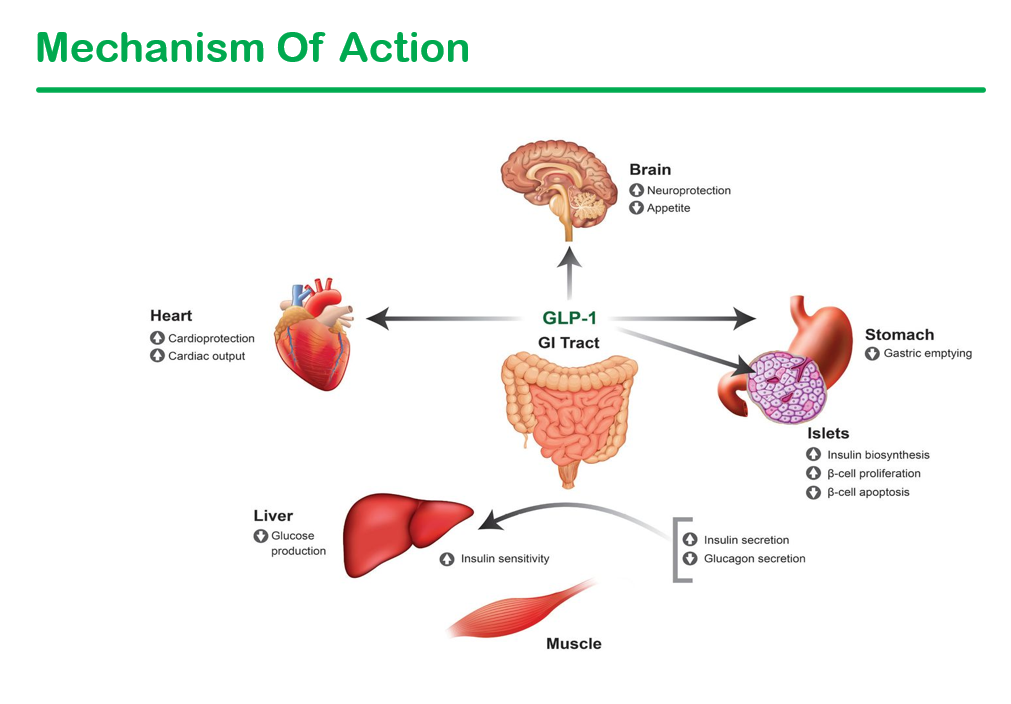
Here are a few slides from Dr. Arora’s lecture:
General points from this lecture:
GLP-1 agents are a huge advance but currently limited by affordability (frequently there is a lack of insurance coverage if there is not T2DM) and availability. In addition, most individuals will regain weight loss when these agents are stopped.
GLP-1 agents are not recommended in the following: patients with gastroparesis, and patients with a personal or family history significant for MEN 2 A /MEN 2 B/ Medullary thyroid cancer
Long-term data is still needed. These agents have been associated with muscle and bone loss; thus, working to assure a good diet is still very important
——————————————————————————
NASPGHAN has a good review/webinar on this topic as well: Pediatric MASLD in the Current Era of Pharmacological and Surgical Obesity Treatment Options. For members, after sign in, you can register and login to this webinar (look under clinical practice tab). This webinar made a lot of useful points (many covered by Dr. Arora too).
For GLP-1 agents, due to effects on gastric emptying, they are generally held prior to anesthesia. If they are given weekly, then hold 1 week prior to anesthesia. If it is a daily medication, hold for 1 day prior to anesthesia.
Surgery definitely helps improve MASH -though variable responses in patients. SLEEVE gastrectomy is currently the most frequent bariatric surgery
There is trouble getting GLP-1 medications.
Limited knowledge regarding long-term effects of cycling of GLP-1 agents.
Obesity is a long-term disease –>anticipate long-term treatment
The Wall Street Journal recently published a personal account of using the newer obesity medications. Bradley Olson, 1/12/24: A Weight-Loss Drug Changed My Life. Will It Solve My Problem? (behind a paywall). This article discusses the dramatic improvement experienced by the writer along with his concerns about the cost of the medication and potential for rebound when he can no longer afford it. Two of the figures:
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
This is a terrific review of obesity and current management options, including surgery and medications. The review provides a thorough explanation of some of the reasons why we are having so many more children with obesity. The article personalizes the problems by focusing on one teen, Alexandra, who underwent sleeve gastrectomy.
Here are a few excerpts (from this lengthy article):
In response to so many grim facts, the A.A.P. in January released its first “clinical practice guideline” for those who care for children who have obesity. The academy now recommends that they immediately start “intensive health behavior and lifestyle treatment,” which it labels “the foundation” of obesity management; this approach supersedes the former strategy of “watchful waiting.” For older youth in certain circumstances — those with a higher B.M.I., say — drugs and, in cases of severe obesity, surgery should be made available as options...
The tenacity ofbody weight can be traced to our biology. Humans evolved to resist losing body fat so that we don’t become extinct, says Rudolph Leibel, chief of the pediatric molecular genetics division at Columbia University’s medical center…
A small number of children with severe obesity are born with leptin deficiency, a gene mutation identified by Sadaf Farooqi, a professor at the University of Cambridge’s Institute of Metabolic Science. Their appetites seem to be bottomless. Though it’s rare, Farooqi cites the extreme effect of this mutation as a clear illustration of the “very strong” impact that biology has upon appetite….Ghrelin, a hunger hormone, increases when food intake is restricted, making us eat more. Insulin, another important hormone, helps turn the food we eat into energy and controls things like blood sugar that influence how much we eat…“We don’t decide whether we’re going to be hungry or not, whether we’re going to have a craving or not….
Genetics may determine more than 70 percent of children’s body weight…But if our genes didn’t change significantly in the last century, why, then, are children getting bigger?No one knows for sure. One likely explanation, however, is the evolutionary mismatch between our genes and our surroundings…
The amount of readily accessible food has expanded immensely, making it easier than ever to eat — open a phone app, say, or go to a drive-through. Plenty of Americans can consume as much as they want, whenever they want.
Today nearly 70 percent of what children eat is ultraprocessed food… Ultraprocessed foods appeal to parents too: They’re cheap, last for years in pantries and freezers and require little preparation. “All food companies are trying to sell products,” Nestle says. “That’s the system, and if the system makes kids fat, well, too bad. Collateral damage.”..Over the past few decades, the variety of food items in some supermarkets has risen to more than 40,000 from 7,000…
Adolescents who have had bariatric surgery — most of them white and female — experienced weight loss similar to what adults lost: around 25 percent of their B.M.I. And while nearly 90 percent of these teenagers needed diabetes medications before the operation, none did afterward…Only a tiny fraction of the teenagers with severe obesity who qualify actually receive the operation…
The latest glucagon-like peptide-1 receptor agonists — as a group, commonly referred to as Ozempic — are the true game changers, a class of drugs that are making possible a degree of weight loss not seen before with medications. The pharmaceutical company Novo Nordisk manufactures GLP-1s for weight loss, one of which is semaglutide and sold under the brand name Wegovy. (Ozempic is the brand name for a lower-dose version of semaglutide that is prescribed to treat diabetes)…
The major studies of children and these drugs have enrolled many fewer adolescent subjects than adults, but no new safety concerns have emerged. In addition to semaglutide’s principal side effects of nausea, vomiting and diarrhea — reported by two-thirds of study participants — more serious ones include gallstones and pancreatitis. Wegovy comes with a caution about possible thyroid cancer, and the F.D.A. mandates that it include a warning about the possibility of suicidal ideation, because it acts on the brain…If patients discontinue the medicines, the weight returns…older drugs in its class have been used to treat diabetes for nearly two decades. But for any new medicine, the long-term risks remain uncertain…
For now, most adolescents who qualify for semaglutide probably won’t be able to get the drug at all [due to cost and drug shortages]….
[At the same time] a greater awareness of the drawbacks that can accompany the medicalizing of obesity, have fueled popular body-positivity movements like Health at Every Size, which seek to disentangle weight from health…
But despite the risks that can accompany obesity treatments — and despite the fact that the data doesn’t always present a clear picture — the prevailing attitude within the medical establishment is that, on balance, the potential negative consequences of obesity are too evident to ignore
Eric Topol: “The GLP-1 and now triple G-Agonists are exceeding expectations as weight loss drugs. Benefits for cardiovascular outcomes, possibly Type 1 diabetes, addiction, and more are reviewed in the latest Ground Truths.” His newsletter also describes the early results of these medications with MASH/NASH with improvement in ~90%.
To get the full review, go to Ground Truths: http://erictopol.substack.com (can sign up to get regular emails on many current medical topics)
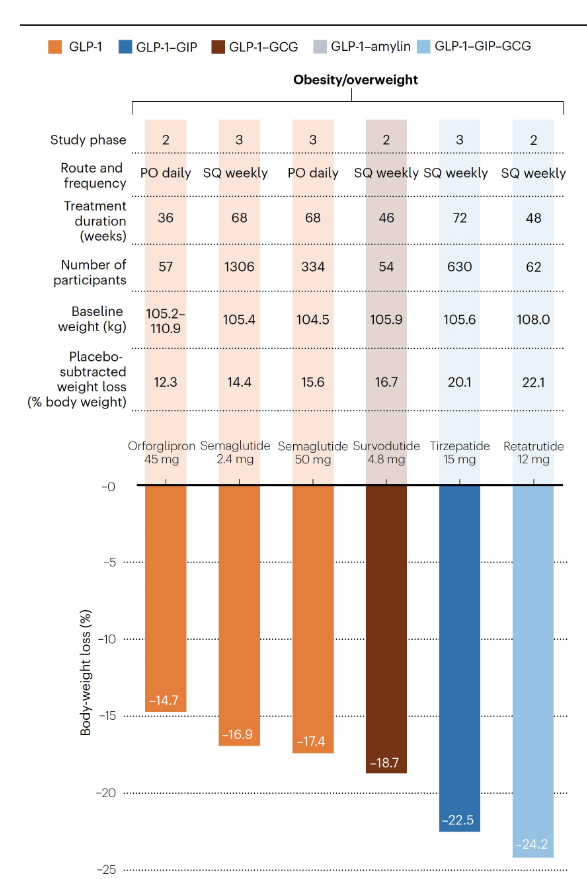
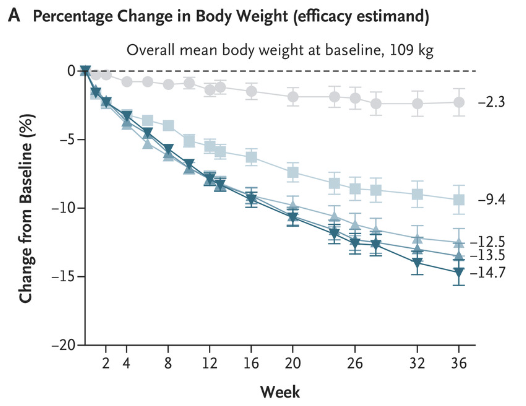
S Wharton et al. NEJM 2023; DOI: 10.1056/NEJMoa2302392. Daily Oral GLP-1 Receptor Agonist Orforglipron for Adults with Obesity
In this phase 2 randomized, double-blind trial with 272 adults with obesity (mean weight at baseline 108 kg), participants were randomly assigned to receive orforglipron at one of four doses (12, 24, 36, or 45 mg) or placebo once daily for 36 weeks. “The pharmacokinetic profile of orforglipron, with a half-life of 29 to 49 hours, supports once-daily oral administration.”
Key findings:
At week 36, the mean change ranged from −9.4% to −14.7% with orforglipron and was −2.3% with placebo.
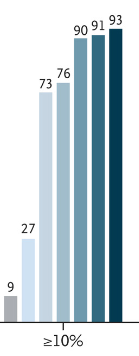
A weight reduction of at least 10% by week 36 occurred in 46 to 75% of the participants who received orforglipron, as compared with 9% who received placebo.
Adverse events reported with orforglipron were similar to those with injectable GLP-1 receptor agonists.
Weight reduction of at least 10% at week 36:
My take: This is an exciting time for drug development for obesity. Given the low success rates of traditional ‘lifestyle’ management approaches, these medications have the potential to reduce a great deal of morbidity. Oral agents, rather than injections, would hasten the use of these agents more broadly. Long term outcomes are still unclear.
AM Jastreboff et al. NEJM 2023; DOI: 10.1056/NEJMoa2301972. Triple–Hormone-Receptor Agonist Retatrutide for Obesity — A Phase 2 Trial.
Background: Retatrutide (LY3437943) is an agonist of the glucose-dependent insulinotropic polypeptide, glucagon-like peptide 1, and glucagon receptors.
Methods: This study enrolled 338 with BMI of at least 27 in a a phase 2, double-blind, randomized, placebo-controlled trial with once-weekly injections of retatrutide.
Key Findings:
The number who achieved at least a 10% weight loss:
“The safety profile of retatrutide was consistent with reported phase 1 findings in persons with type 2 diabetes13 and similar to those of therapies based on GLP-1 or GIP–GLP-1 for the treatment of type 2 diabetes or obesity”
My take: There are a number of effective agents for obesity that have been developed very recently. Long term efficacy and safety are still not well-understood.
This 38 page report has a ton of updated recommendations and useful advice –geared to adults with fatty liver disease. The last ~dozen pages are the 491 references.
Some of the useful points:
CVD and nonhepatic malignancies are the most common causes of mortality in patients with NAFLD without advanced fibrosis; death from liver disease predominates in patients with advanced fibrosis.
Initial lab evaluation in adults:
Statins are safe and recommended for CVD risk reduction in patients with NAFLD across the disease spectrum, including compensated cirrhosis.
Patients with NAFLD should be screened for the presence of T2DM. T2DM is the most impactful risk factor for the development of NAFLD, fibrosis progression, and HCC.108–111 Given the central pathogenic role that insulin resistance plays in the pathogenesis of both T2DM and NAFLD, it is not surprising that patients with T2DM have a higher prevalence of NAFLD (ranging from 30% to 75%)10,112,113 and a higher risk of developing NASH with fibrosis.93,114–117
Other important comorbidities: dyslipidemia, obstructive sleep apnea, cardiovascular disease, and chronic kidney disease
Lifestyle factors that can be beneficial:
Table 6 lists potential medications though there are no FDA approved treatments for fatty liver disease. Bariatric surgery is also a beneficial treatment option “in patients who meet criteria for metabolic weight loss surgery, as it effectively resolves NAFLD or NASH in the majority of patients without cirrhosis and reduces mortality from CVD and malignancy.”
Potentially useful medications include Vitamin E, Pioglitazone, Liraglutide, Semaglutide, Tirzepatide and SGLT-2i. “Semaglutide can be considered for its approved indications (T2DM/obesity) in patients with NASH, as it confers a cardiovascular benefit and improves NASH. Pioglitazone improves NASH and can be considered for patients with NASH in the context of patients with T2DM . Available data on semaglutide, pioglitazone, and vitamin E do not demonstrate an antifibrotic benefit, and none has been carefully studied in patients with cirrhosis.”
Treatments NOT Recommended: “Metformin, ursodeoxycholic acid, dipeptidyl peptidase-4, statins, and silymarin are well studied in NASH and should not be used as a treatment for NASH as they do not offer a meaningful histological benefit.”