D Wendel et al. JPGN 2021; 72: 474-486. Free full text: Management of Central Venous Access in Children With Intestinal Failure: A Position Paper From the NASPGHAN Intestinal Rehabilitation Special Interest Group
This is a very useful article with recommendations for central venous access in children. The main recommendations are summarized in Table 3 & listed below; however, there is a lot of detailed information in the article on frequent issues like schools, travel (including dealing with TSA), sports, and even swimming. In addition, the article delineates recommendations for management and prevention of line complications.
1. Recommendations for venous access:
- Tunneled, single lumen, cuffed silicone catheters should be used for children with IF.
- Upper extremity access is the preferred location when available.
2. Recommendations pertaining to routine CVC care:
- Proper technique and hygiene surrounding CVC care are of paramount importance in preventing CVC-associated complications. Caregivers should receive directed education regarding CVC care before initial discharge, with subsequent reinforcement education as needed.
- CHG impregnated supplies (disk, sponge, or dressing) should be considered for central line dressing in pediatric IF patients.
- Routine surveillance of central venous access should be performed by US. MR, CT, or traditional venography should be reserved for when further delineation of access is required.
3. Recommendations regarding general considerations—sports, travel, and emergencies:
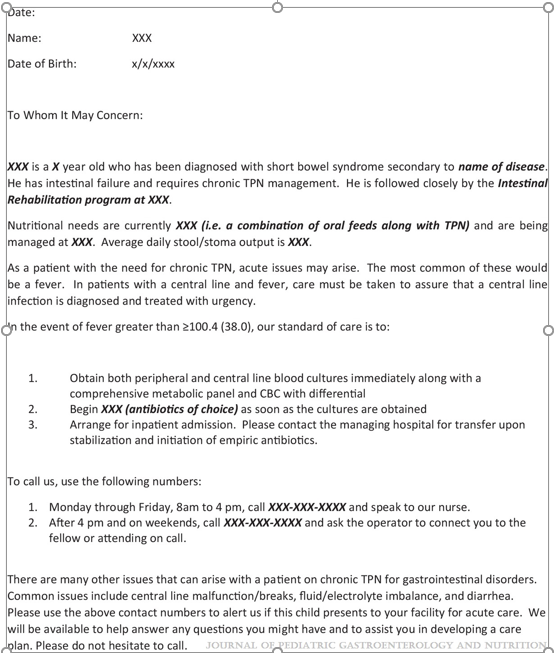
- All children with IF should be provided with an emergency letter that details the specific needs of the individual child in case of an emergency. (See at bottom for example -Figure 1)
- Discuss with families the risks of swimming and sports participation with strategies to protect the dressing and central line.
- All travel plans should be discussed with the intestinal rehabilitation team well in advance of travel to facilitate discussion of a plan of care in case of emergency.
4. Recommendations regarding central line-associated bloodstream infections:
- All children with IF and CVC who develop a fever (≥38.0°C) should be admitted to the hospital and assessed for bacteremia with central and peripheral blood cultures while receiving broad-spectrum empiric antibiotics through the CVC for at least 48 h, awaiting culture results regardless of other infectious sources.
- If clinically stable, discuss with the patient’s IRP before line removal for CLABSI.
- Prophylactic lock therapy with ethanol or other nonantibiotic locks should be strongly considered in all children with IF who have had at least one central line-associated bloodstream infection or are at high risk for infection.
5. Recommendations pertaining to central line mechanical complications:
- In children with IF, CVC should be repaired whenever possible to preserve central venous access.
- Children with IF and a newly identified CRT should be treated with low molecular weight heparin for at least 6 weeks with guidance from a hematologist.
- Children with IF who have persistence of at least one chronic thrombus should be maintained on prophylactic anticoagulation with low molecular weight heparin.
- Children who have lost multiple sites of central venous access should be considered for referral to an intestinal transplant center for evaluation and management
6. Recommendations for central venous access program management:
- All centers following children with IF should, at a minimum, track the number of outpatient CLABSI per 1000 catheter days.
With regard to swimming: “Swimming introduces an incompletely defined but potentially severe risk to those requiring chronic central venous access. Contamination of various chlorine-treated (swimming pools), stagnant (lakes and ponds), and flowing (oceans and rivers) bodies of water with human pathogens has been well documented, though proper maintenance may minimize outbreaks. The potentially fatal risk of such contaminants gaining access to central circulation via the CVC is unclear…Parents seeking guidance are confronted by mixed messaging from support programs, online resources and blogs, and even IRP. These conflicting recommendations and practices reflect the paucity of data to guide a safe and clear approach for swimming with a central line…[in one study of 16 home PN programs] swimming in low-risk situations [was permitted but] recommended immediate site cleaning and dressing change following water exposure and avoidance of submersion for 4–6 weeks after CVC placement. Ultimately, the decision to permit children with IF to swim lies with the parent or guardian.”

Related blog posts:
- Central Line Pointers
- Is It Safe To Exclude Central Line Infections at 24 hrs?
- Polyurethane vs Silcione with Ethanol Locks
- Antibiotic Selection for Suspected Central Line Infections
- #NASPGHAN19 Intestinal Failure Session Part 1
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.