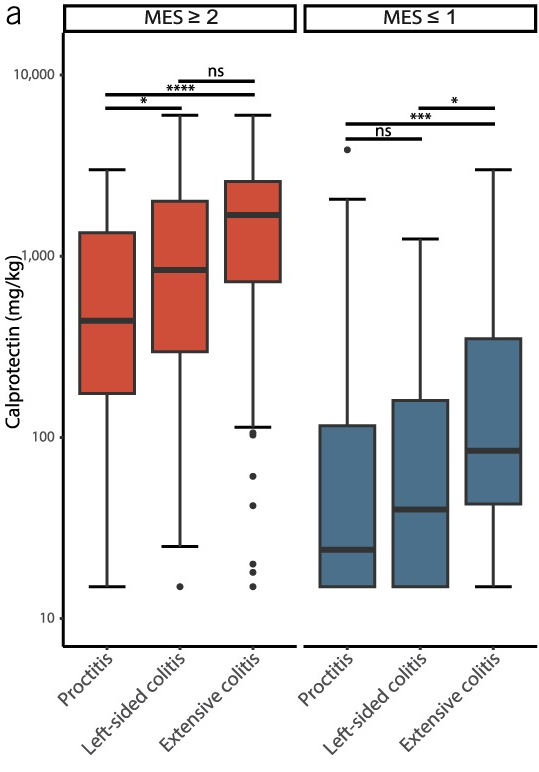
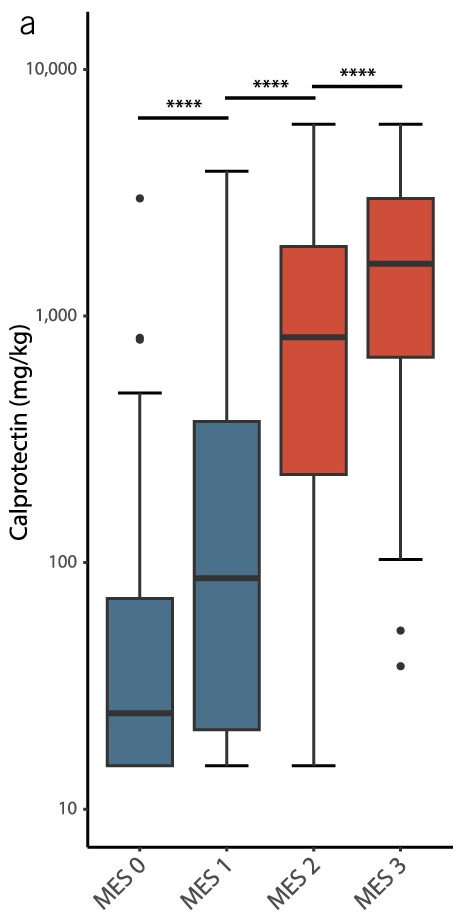
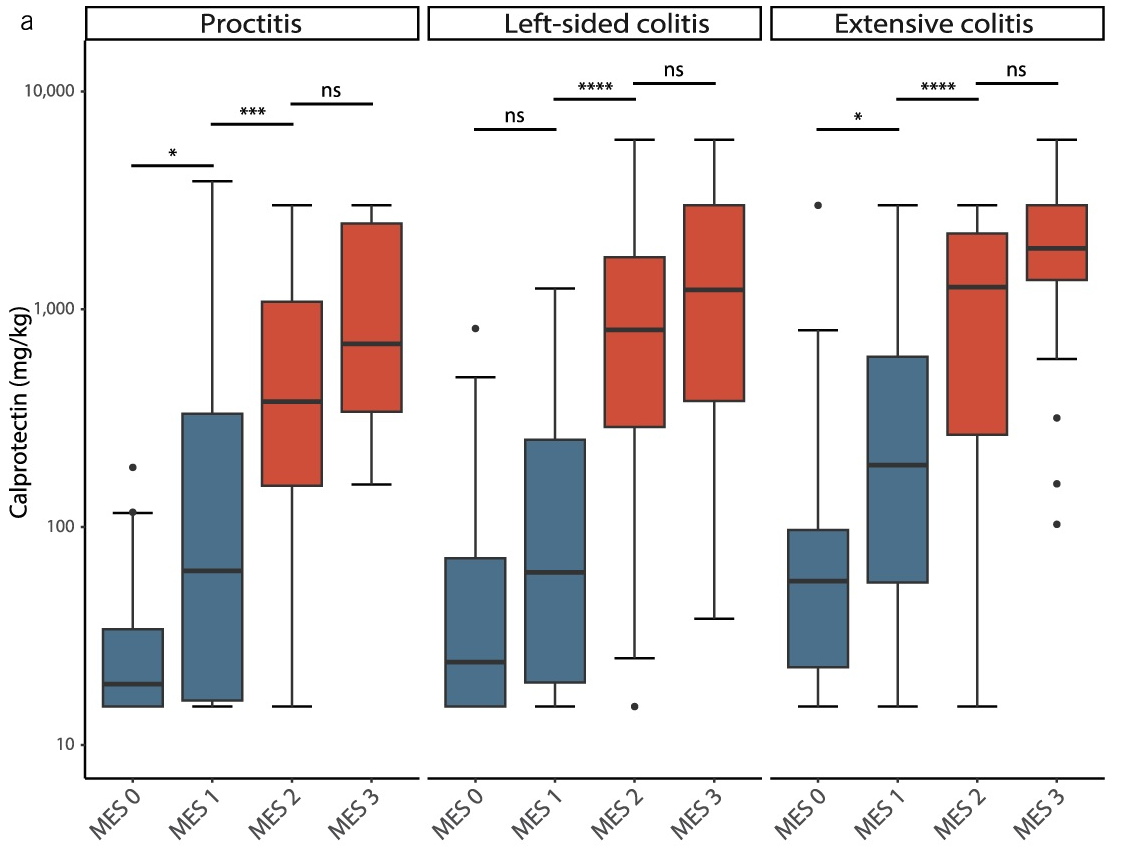
This single-center observational study (n=254) examined the correlation between fecal calprotectin (FC) levels with both disease extent and mucosal healing in ulcerative colitis. Mucosal healing was rated by the Mayo Endoscopic Score (MES).
Key findings:
Disease extent: FC levels were significantly lower in proctitis (440 mg/kg) as compared with left-sided colitis (840 mg/kg) or pancolitis (1,690 mg/kg)
Mucosal healing: In MES ≤1, FC levels were significantly lower in proctitis (24) compared to left-sided colitis (40) or pancolitis (85)
My take: Fecal calprotectin levels are clearly affected by the extent of disease involvement. However, the increase in calprotectin values associated with disease activity was significantly larger than the differences attributed to disease extent.
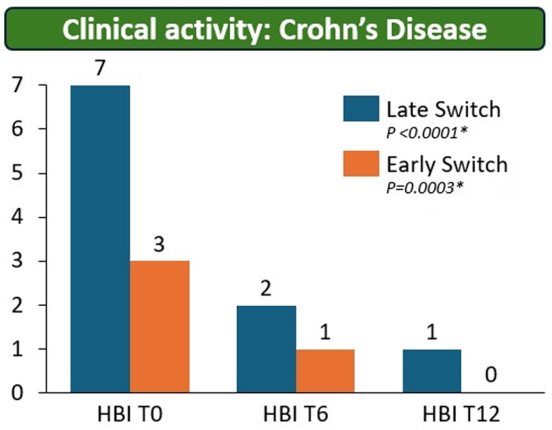
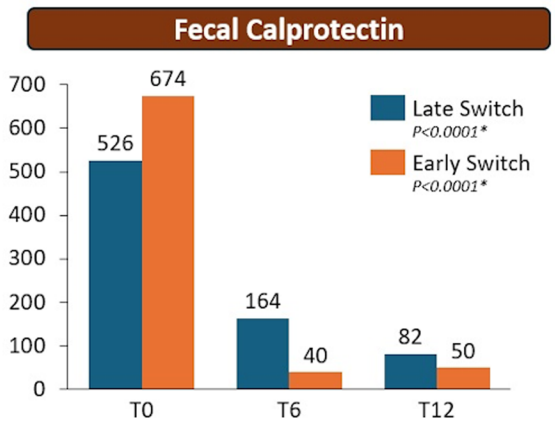
Methods: The RE-WATCH study was an observational, multicenter, retrospective study performed in four IBD referral centers. Inclusion criteria meant that only patients receiving on label SC-IFX at a dosage of 120 mg every other week were included in the study. The initiation of IFX therapy as the baseline timepoint.
Key findings:
There were no statistical differences between the two groups, early vs. late switch, after one year in terms of the respective endoscopic response (71.4% vs 70.8%, P = .95), steroid-free clinical remission (62.5% vs 68.7%, P = .51), or IFX retention rate (75.0% vs 66.7%, P = .35).
There was higher endoscopic remission rates in early switch patients as compared to late switch patients; however, this trend was not significant (69.6% vs 52.1%, P = .07).
A return to IV-IFX was required in 1 of 43 early switch patients and in 3 of 44 late switch patients (2.3% vs 6.8%, P = .31)
While the early switch group appears to fare a little better, there is likely a selection bias. For example, the early group had a much lower rate of severe endoscopic score at baseline (20% vs. 54%) and lower rate of Crohn’s fistulizing disease (8% vs 33%).
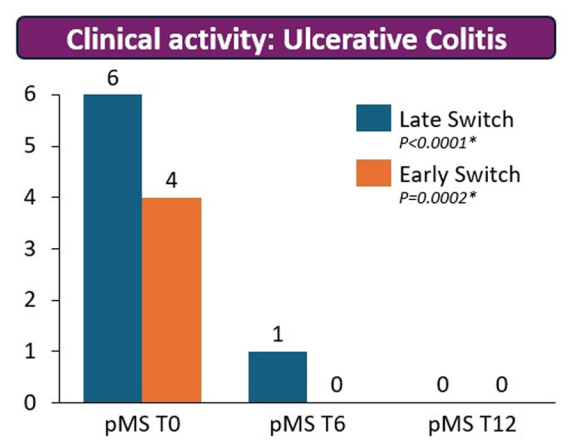
partial Mayo score (pMS)Harvey–Bradshaw index (HBI)
My take: These results indicate that outcomes are similar between patients switching from to IFX SC at both early (after induction) and late (after 6 months).
It is worth noting that prior studies have shown that home-based therapies (eg. home infusion), compared to office-based therapies, have been “associated with suboptimal outcomes including higher rates of nonadherence and discontinuation of infliximab.” This is a concern for SC biologics as well.
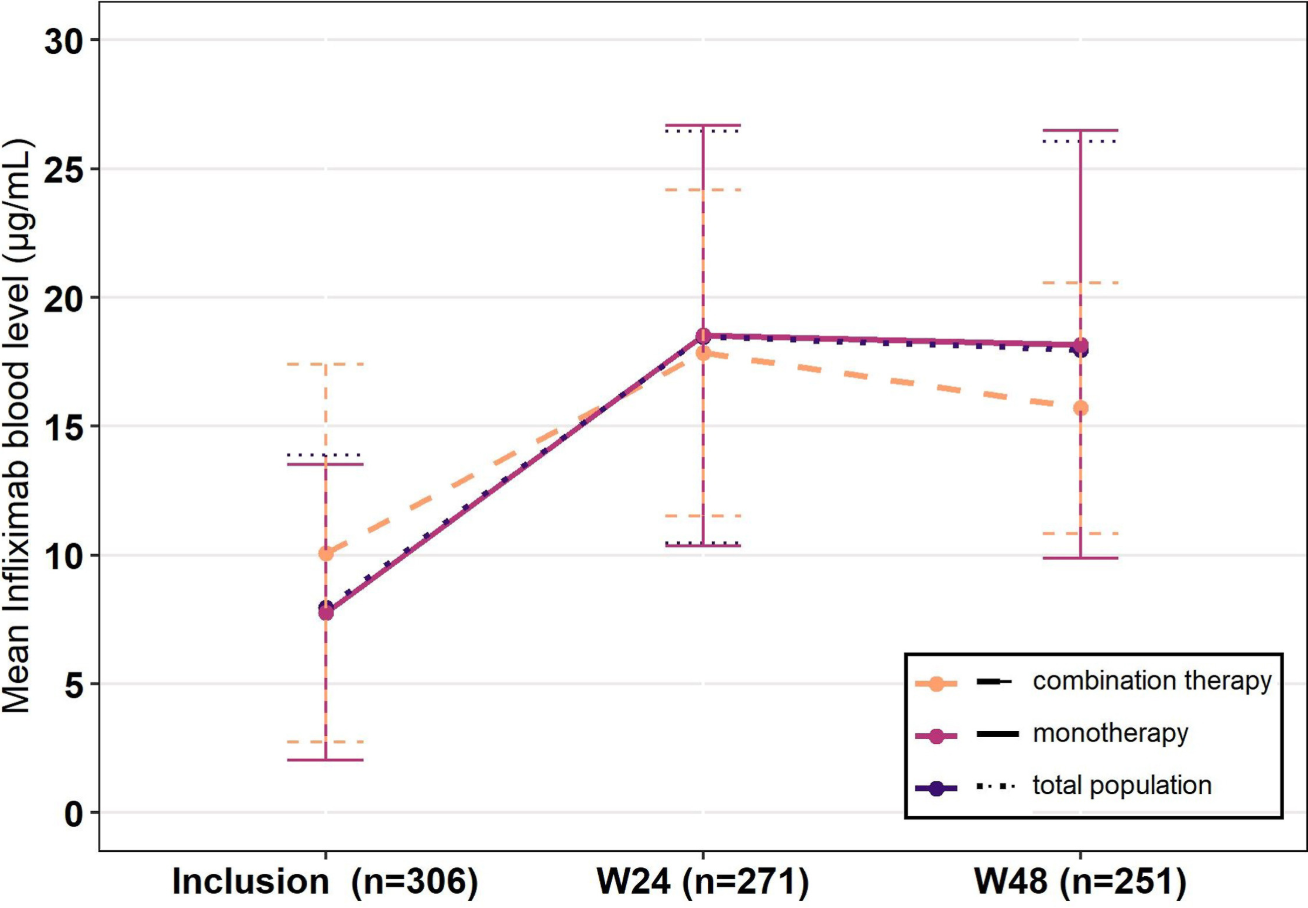
Methods: The PEREM (PErsistence, effectiveness and safety of subcutaneous infliximab after switch from intravenous infliximab in IBD patients in REMission) study, a prospective national French cohort trial, enrolled 426 patients with IBD. Participants were in steroid-free clinical remission for at least 6 months on IV-IFX when they switched to SC-IFX. 56% were on IV-IFX standard dosing (5 mg/kg 8-weekly) and 16% received combination therapy with an immunomodulator drug at baseline. All patients were switched to SC-IFX standard dosing (ie, 120 mg every other week). The treatment could be intensified during follow-up, either to 120 mg every week or 240 mg every other week.
Key Findings:
At week 48, SC-IFX persistence was 95.4%
86.9% of patients were in steroid-free clinical remission
Mean infliximab levels were 8.0 μg/mL at inclusion and 18.0 μg/mL at week 48 (P < .0001)
Among the 19 (4.5%) patients who stopped SC-IFX, 6 (1.4%) switched back to IV-IFX
Dosing at 10 mg/kg/Q4W had 100% SC IFX persistence compared to 95% for 5 mg/kg/Q8W; however, at the 48 week followup, there were only 6 patients in the higher dose compared to 149 in the lower dose
Ongoing use of combination therapy was not associated with better persistence. Though, only 7 patients were receiving combination therapy at the 48 week followup
From the discussion:
“The high persistence observed in the PEREM study is partly explained by the long-term control of the disease by the time of switch, the median time since last flare being over 5 years before inclusion. Henceforth, the persistence observed here is in accordance with results on long term maintenance of IV-IFX, the yearly persistence of IV-IFX without intervention being 87%.”
SC-IFX was associated with higher levels. However, this was expected and higher levels are needed with SC administration. The “different bioavailability of SC-IFX compared with IV-IFX is responsible for different goals of infliximab blood levels depending on its route. In particular, a level above 20 μg/mL has been associated with higher rates of remission20” with SC-IFX.
My take: This study shows that SC-IFX is a good option for patients in long-term remission. With SC-IFX therapy, more effort is needed to make sure patients are adherent with therapy and monitoring in order to achieve optimal outcomes.
This was a multicenter, retrospective, case-control study of patients hospitalized with ASUC who underwent colectomy, comparing patients treated with tofacitinib (n=41) prior to colectomy with infliximab-treated controls (n=68).
Key findings:
Compared with tofacitinib-treated patients, infliximab-treated patients had higher overall rates of overall (44 [64.7%] vs 13 [31.7%]; P = .002) and serious (19 [27.9%] vs 3 [12%]; P = .019) postoperative complications
My take: This study supports the safety of JAK inhibitor therapy for ASUC. It showed a significantly lower rate of overall postoperative complications in ASUC patients treated with tofacitinib compared with infliximab; the authors note that “these findings can likely be extrapolated to upadacitinib, a selective JAK inhibitor, given its similar mechanism of action.”
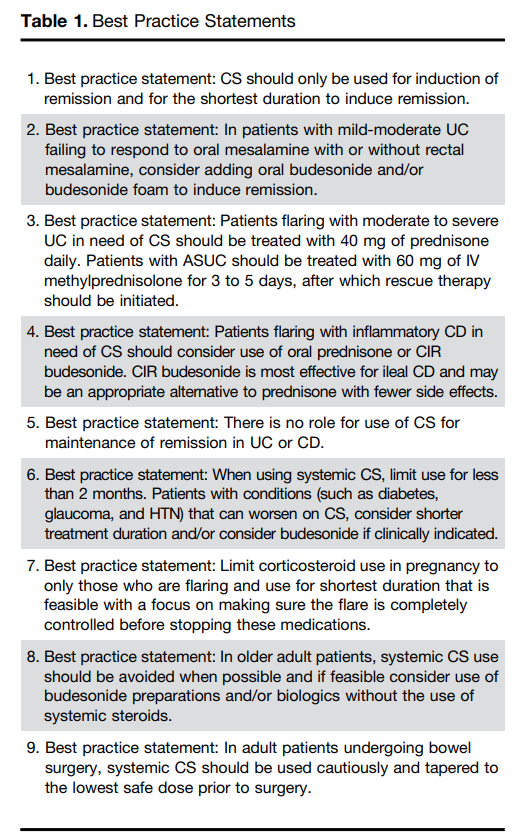
Steroids are commonly used and misused for inflammatory bowel disease. This article reviews best practices, steroid formulations/dosing, and potential complications.
For moderate to severe ulcerative colitis (in adults), the authors recommend treatment with 40 mg of prednisone daily. Patients with ASUC (acute severe ulcerative colitis) should be treated with 60 mg of IV methylprednisolone for 3 to 5 days, after which rescue therapy should be initiated
Use of budesonide is recommended as an option for many clinical situations to minimize steroid adverse effects. These situations include mild-moderate UC failing to respond to mesalamine, ileal CD and older patients
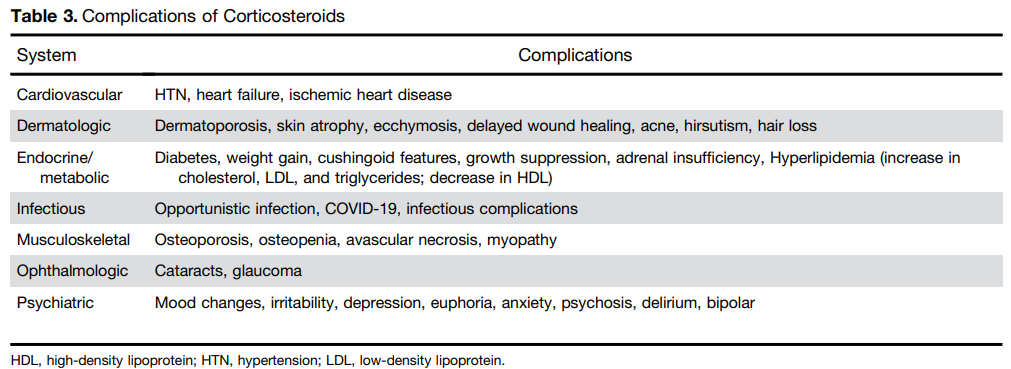
Postoperative complications: “In the postoperative period, patients treated with CS had a higher risk of both infectious complications (aOR, 3.69; 95% CI, 1.24–10.97) and major infectious complications (aOR, 5.54; 95% CI, 1.12–27.26) [Abrerra et al].135 Subramanian pooled data from 7 studies showing that preoperative CS use is associated with increased postoperative complications (OR, 1.41; 95% CI, 1.07–1.87) as well as infectious complications.
The authors note that corticosteroids “remain widely available and are an effective short-term option for induction of remission in patients with active UC or inflammatory CD. However, their well-described and significant safety profile warrants proactive strategies to limit their use through non-systemic formulations, short-term exposures, steroid-sparing maintenance options, and most recently, complete steroid avoidance strategies.”
My take: Continuing steroids when they are not effective prior to potential surgery (eg. ASUC) remains a frequent problem. Sometimes, it is difficult to know it they are helping some.
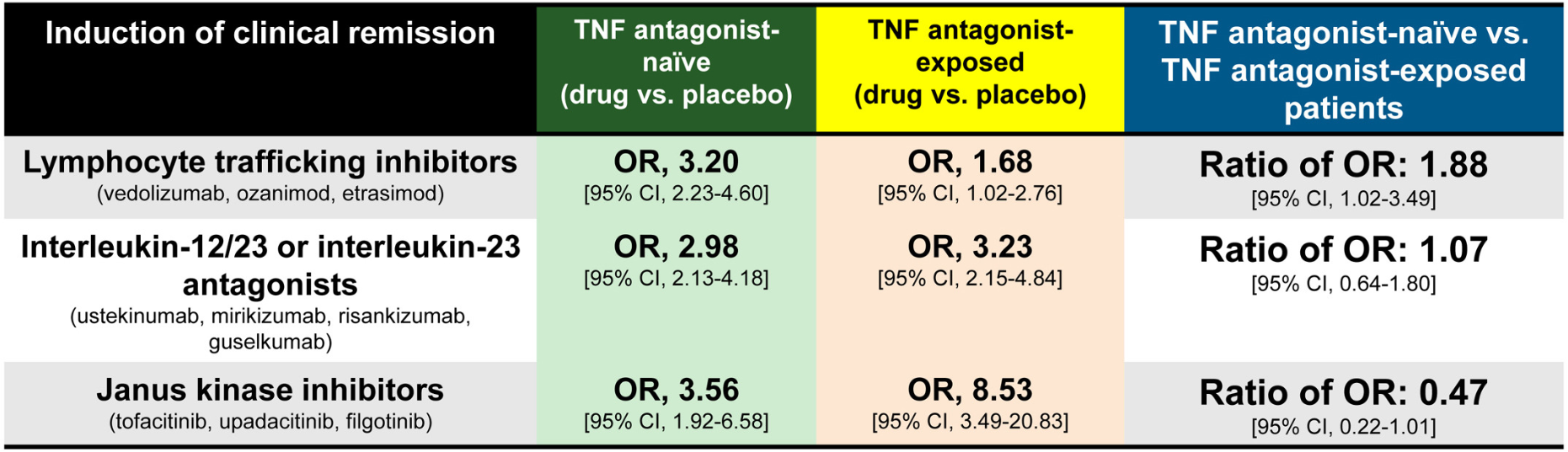
Methods: Meta-analysis of 17 randomized controlled trials in 8871 adults with moderate-severe UC. The authors calculatedthe ratio of odds ratio of achieving remission with active drug vs placebo, in TNF antagonist–naïve vs TNF antagonist–exposed patients.
Key findings:
JAK inhibitors: Less efficacious in TNF antagonist–naïve vs exposed patients (6 trials; ratio of OR, 0.47)
IL-23 antagonists: No significant difference was observed in efficacy of selective interleukin-23 antagonists vs placebo in TNF antagonist–naïve vs exposed patients (6 trials; ratio of OR, 1.07)
Lymphocyte trafficking inhibitors: More efficacious in TNF antagonist–naïve vs exposed patients (5 trials; odds ratio [OR], 1.88)
Discussion:
This study “confirmed prior observations that exposure to TNF antagonists significantly reduces the efficacy of lymphocyte trafficking inhibitors in inducing remission, including both vedolizumab and S1P receptor modulators, by approximately 50%.In contrast, prior exposure to TNF antagonists was associated with a significant increase in the efficacy of JAK inhibitors in inducing remission, with 2-fold higher efficacy in TNF antagonist–exposed vs TNF antagonist–naïve patients”
In the SELECT-COMPARE trial in patients with rheumatoid arthritis, there was also an improved response to upadacitinib in patients with prior adalimumab.
“The current findings raise the intriguing possibility that exposure to TNF antagonists could result in lasting effects on the immune system that differentially alter responsiveness to therapies with distinct mechanisms of action”
My take: This study suggests that JAK inhibitors are a good choice for secondary therapy after anti-TNF agents. Other factors, besides efficacy, including safety, extraintestinal manifestations, and cost, have to be considered as well.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Today and tomorrow I am highlighting two adult clinical guidelines both of which are equivalent to up-to-date textbook chapters with specific recommendations; both are open access. In addition, the articles have accompanying author podcasts. Thanks to Ben Gold for these references.
Table 2 in the UC guideline makes 54 recommendations and Table 3 provides 57 key concepts.
Selected Management Recommendations:
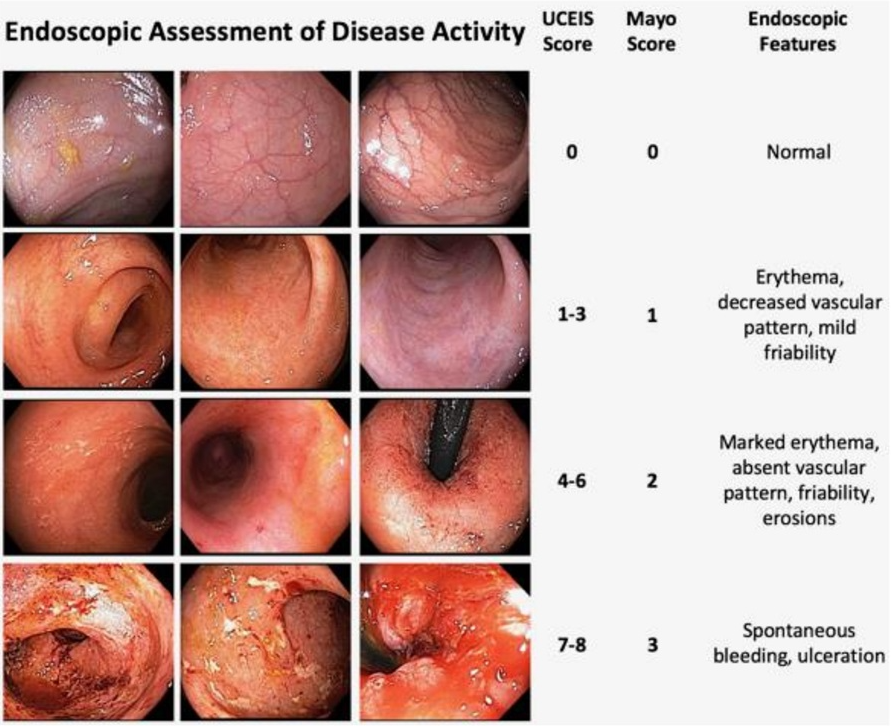
Table 2, #4: We recommend treating patients with UC to achieve endoscopic improvement (Mayo score 0 or 1) to increase the likelihood of sustained steroid-free remission and to prevent hospitalization and surgery
Table 2, #5: We recommend the use of FC (fecal calprotectin) in UC to assess response to therapy, to evaluate suspected relapse, and during maintenance
Table 2, #33: When infliximab is used as induction therapy for patients with moderately to severely active UC, we recommend combination therapy with a thiopurine
Table 2, #43: Recommend continuing tofacitinib or upadacitinib as compared with no treatment for maintenance of remission in patients with prior moderately to severely active UC now in remission after induction with tofacitinib or upadacitinib. **The authors recommend continuing each biologic that achieved remission with induction therapy (#38-#43)
Table 2, #51: In patients with ASUC failing to adequately respond to intravenous corticosteroids (IVCS) by 3 days, we recommend medical rescue therapy with infliximab or cyclosporine (Strong recommendation, moderate quality of evidence).
Key concepts:
Table 3, #29: Patients who are primary nonresponders to an anti-TNF (defined as lack of therapeutic benefit after induction and despite sufficient serum drug concentrations) should be evaluated and considered for alternative mechanisms of disease control (e.g., in a different class of therapy) rather than cycling to another drug within the anti-TNF class.
Table 3, #31: Subcutaneous infliximab and vedolizumab are considered equivalent to the standard intravenous maintenance dosing of these agents. The equivalence of the subcutaneous formulations for induction or as substitution for escalated doses of these therapies has not been robustly established.
Table 3, #41: Patients with UC should have available all medical options as recommended by their doctor and healthcare team. Third-party payers and requirements for step therapy should not come between the patient and their healthcare team in making decisions about treatment for UC.
Table 3, #48: All patients with ASUC should undergo a flexible sigmoidoscopy within 72 hours and preferably within 24 hours of admission. This should be used to assess endoscopic severity of inflammation and to obtain biopsies to evaluate for cytomegalovirus (CMV) colitis.
Table 3, #51: Nonsteroidal anti-inflammatory drugs (NSAIDs), narcotics, and medications with anticholinergic side effects should be avoided in ASUC.
Table 3, #57: In patients with ASUC initiating infliximab, dose intensification should be considered for those patients with low serum albumin (<2.5 g/dL).
My take: This article does an excellent job of summarizing current available evidence and good practice. Many of the recommendations may be helpful in garnering approval from third party payers.
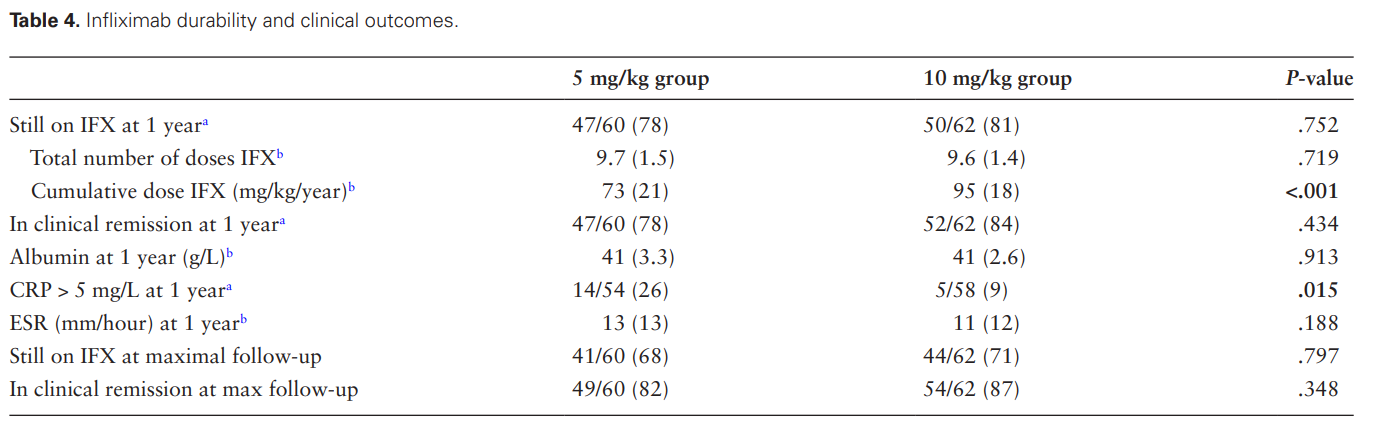
In this single center retrospective study from Ireland, the authors examined 122 patients (93 with Crohn’s disease [CD], 18 with ulcerative colitis [UC], 1 with IBDU) who received infliximab and had prospectively-collected data. The earlier cohort 2018-2019 received 5 mg/kg/dose and the later group 10 mg/kg/dose. Both groups had proactive therapeutic drug monitoring (pTDM).
Key findings:
The 5 mg/kg group, compared to the 10 mg/kg group, was less likely to have target pre-third TLs (6% vs 80%, P < .001) with the stated goal of >/= 15 microgm/mL
Fewer patients in the 5 mg/kg than 10 mg/kg group had pre-fourth TLs ≥5 µg/mL (6/48 [12.5%] vs 28/50 [56%], P < .001; mean [SD] TL 3.5 [6.3] vs 10.0 [9.9], P < .001)
Concurrent immunomodulator therapy was more common in the 5 mg/kg group (43% compared to 24%)
80% of patients were still receiving infliximab at 1 year including 87% of patients with CD and 54% with UC
The higher dose group had a lower CRP at 1 year followup. 26% of patients receiving the lower dose had a CRP > 5 mg/L compared with 9% in the higher dose group.
Some other measures of long term outcome (eg. IFX durability, clinical remission) were slightly better but did not reach statistical significance (see below)
Discussion Points:
“Our data show higher rates of below-target infliximab levels during and after induction in the 5 mg/kg group. Higher rates of dose escalation in this group during the first year resulted in similar dosing regimens…Thus, the similar infliximab durability and clinical outcomes at 1-year follow-up reflect early-dose optimization leading to dose equalization between the 2 groups, rather than a lack of benefit to higher dosing regimens”
“Our data affirm that proactive TDM with pre-emptive dose escalation restores below-target infliximab TLs and sustains clinical response…Indeed, in our cohort, some patients with low IFX levels pre-third dose were given their fourth dose 6 weeks later, rather than the standard 8 weeks. Without proactive TDM results, our rate of suboptimal TLs pre-fourth and during maintenance therapy would have been higher in both groups”
“Rates of immunomodulator use in the 10 mg/kg group were lower than in the earlier cohort of 5 mg/kg, reflecting changes in clinical practice over time”
My take:
This study shows that 94% of pediatric patients did NOT achieve adequate levels of infliximab at the pre-third dose with “standard” therapy. This was true even with 43% of the lower dose cohort receiving combination therapy (which often helps improve pharmacokinetics)
Proactive therapeutic drug monitoring helped mitigate the clinical outcomes, especially in the lower dosed cohort
“Children with IBD treated with the historic standard dose of 5 mg/kg induction are at increased risk of pharmacokinetic treatment failure related to high rates of suboptimal TLs”
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
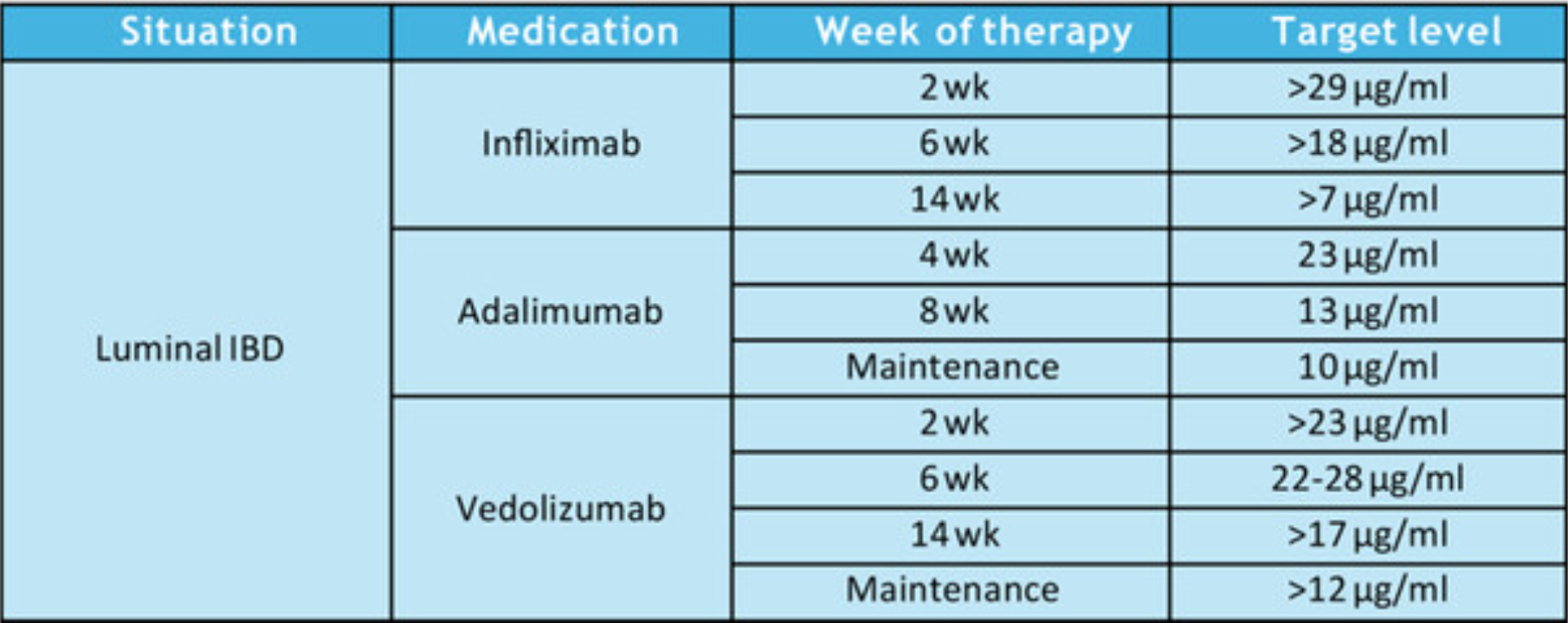
Therapeutic Drug Targets Based on Condition, Medication and Time of Therapy:
Discussion Points:
Pediatric Dosing is Different: “Pediatric studies have also determined adult infliximab targets are insufficient…In a prospective pediatric study, Clarkston et al. found that a trough level of 29 μg/mL at 2 weeks is required to achieve both clinical and biologic response. Patients with lower trough levels had 13-fold greater odds of clinical nonresponse. Additionally, a trough of 18 μg/mL at 6 weeks was associated with improved response. Patients with lower trough levels had sixfold greater odds of clinical nonresponse. They also observed that patients who did not achieve a trough >5–7 μg/mL by 14 weeks of therapy had a 21-fold increase in the odds of clinical nonresponse.62“
Undetectable/very low anti-TNF levels: “If the serum level is extremely low or undetectable, then full re-induction is warranted in addition to dose escalation.”
Timing of TDM: “As a practice point, TDM is routinely recommended at the end of induction for most patients. We recommend obtaining TDM earlier during induction in at-risk populations, including younger age children, those with hypoalbuminemia, and those with increased inflammatory burden.”
Maintenance proactive TDM: “Based on prospective randomized trial evidence, we recommend proactive TDM during maintenance every 6–12 months…yearly proactive TDM was associated with 55% reduced risk of developing antidrug antibodies.26“
Increased Antidrug Antibodies with Lower Infliximab Dosing: “In the pivotal REFINE study on immunogenicity in pediatric IBD, Coleman et al. found that antibodies to infliximab were detected in 68% of patients in the cohort, and starting dose under 7.5 mg/kg was one of the strongest predictors of developing antidrug antibodies.4“
Higher Doses Prevent Antidrug Antibodies: “The best available evidence for preventing immunogenicity supports initiating therapy with infliximab doses greater than 8 mg/kg, and in the case of hypoalbuminemia, doses greater than 10 mg/kg. For children <40 kg, doses of 200 mg/m2 are more appropriate.”
Perianal fistulas: “Overall, there is less evidence to support adalimumab use over infliximab for treatment of perianal fistulas. It is possible that adalimumab may have lower efficacy for perianal fistula.105 However, it is unclear if this is inherent to adalimumab, or if it relates to less frequent TDM or less frequent dose escalation in practice.”
Vedolizumab: “In general, as with other biologic therapies, a higher serum vedolizumab concentration is associated with higher likelihood of treatment response…Multiple studies identified that in patients with IBD (either UC or CD) early trough levels at Week 2132 with a cut off of >23.2 μg/mL or Week 6133, 134 with a cut off of above 22–28 μg/mL or at Week 14135) above 16.55 μg/mL predicted a higher likelihood of sustained response over the first year. In regard to clinical remission one study identified that corticosteroid free, clinical and biochemical remission was correlated to higher trough vedolizumab concentration.136“
Vedolizumab in younger patients: “Children under 30 kg require vedolizumab doses of 200 mg/m2 or 10 mg/kg.”
My take: “This NASPGHAN position paper should also serve to document that high-dose therapy, especially guided by TDM, is evidence-based standard of care.” This article clearly establishes three key points:
“Intensive anti-TNF⍺ dosing strategies are not experimental. The initial doses of infliximab and adalimumab approved by the United States Food and Drug Administration (FDA) routinely lead to under-treatment, poor outcomes, and treatment discontinuation.60, 117 There is a rich, corroborated, and verified evidence-base to support the safety and efficacy of high-dose therapy anti-TNF⍺ therapy when clinically indicated, especially as supported by TDM.50, 62, 65, 100, 101, 103, 118“
Therapeutic drug monitoring is essential in the pediatric population to optimize drug levels, allow many patients to do well with monotherapy, and to help avoid development of antidrug antibodies.
The best available evidence supports TDM during induction of vedolizumab as well.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
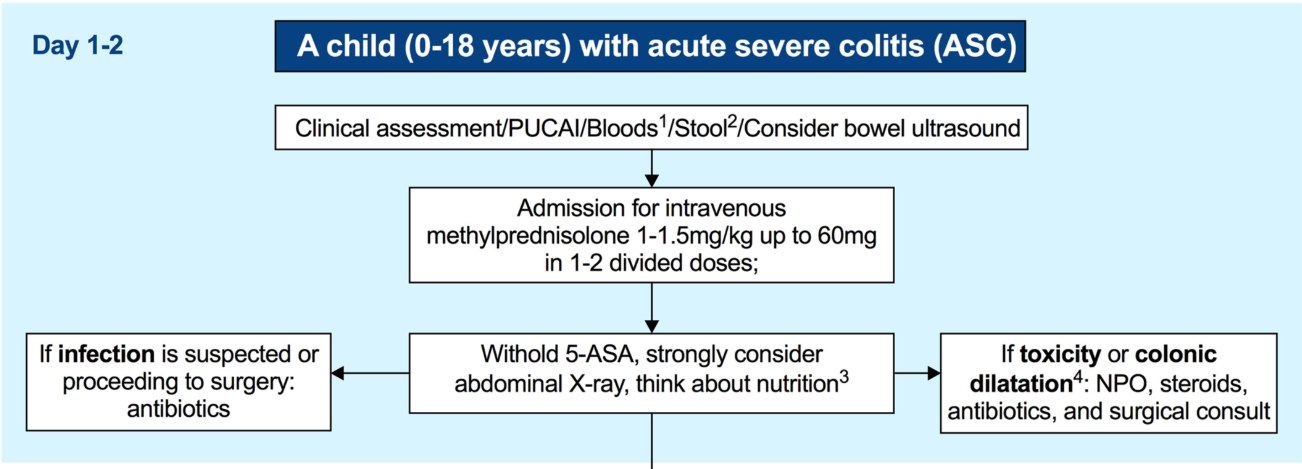
Comprehensive review (69 pages!) of all the topics related to acute severe colitis are covered. Topics include associated enteric infections (C diff, CMV), toxic megacolon, antibiotics, pain management, VTE, surgery, and pouchitis.
Some of the recommendations:
All mesalamine preparations (oral and rectal) should be discontinued upon admission to exclude mesalamine intolerance, especially when mesalamine has been commenced during the preceding few weeks; (re-) introduction should be considered after significant improvement in the clinical condition [EL5, adults EL5] (*100% agreement).
Regular diet should be continued in most ASC cases [not in toxic megacolon]. Enteral nutrition may be used if oral feeding is not tolerated or in malnourished children [EL4, adults EL1] (*100% agreement).
Pharmacological thromboprophylaxis for reducing the risk of VTE should be considered in all inpatient children with ASC (Figure 1) [EL5, adults EL2] (*100% agreement).
Intravenous methylprednisolone 1 mg/kg/day (up to 40 mg/day) once daily is the first-line treatment in ASC and should be promptly started [EL2, adults EL1]. A higher dose of 1.5 mg/kg/day (up to 60 mg/day) can be used at the clinician’s discretion (e.g., in patients on oral corticosteroids at admission and/or with a more severe spectrum of ASC) [EL4, adults EL4] (*100% agreement).
Intravenous methylprednisolone should not be extended beyond 7–10 days of total course, since it carries no additional benefit and increases toxicity. In corticosteroid-refractory patients in whom second-line therapy is initiated, there is no need for corticosteroid tapering if corticosteroids are given as an isolated short course (up to 10 days) (*100% agreement).
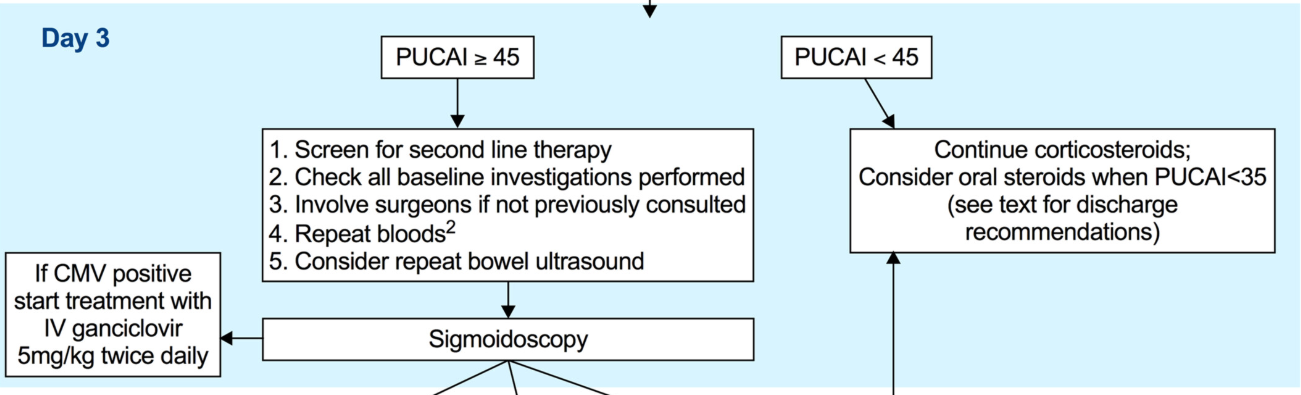
A PUCAI > 45 on the 3rd day of IVCS treatment should dictate planning for second-line therapy between Days 3–5 [EL2, adults EL2] (*100% agreement).
Second-line therapy should be initiated on the 5th day of IVCS treatment in children with a PUCAI ≥ 65 [EL2, adults EL2] (*100% agreement).
Infliximab is recommended as the preferred second-line medical therapy for anti-TNF naive children failing IVCS [EL3, adults EL1] (*100% agreement).
To reduce unnecessary immunosuppression, corticosteroids (when ineffective) should be rapidly weaned following introduction of second-line therapy or decision to proceed to colectomy (stopped if in use ≤10 days and reduced to prednisone ≤0.2 mg/kg or equivalent to 10 mg adult dose with gradual tapering thereafter if >10 days) [EL5, adults EL5] (*100% agreement).
Third-line sequential rescue therapies (CNIs after infliximab, infliximab after CNI or a JAK inhibitor after either) may be considered in stable patients, in specialised centres and in those whose corticosteroids were weaned off or nearly weaned off as stated above [EL5, adults EL2] (*100% agreement).
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.