Pictures from today’s CCFA Fundraiser -we had about 25 GI Care for Kids staff/family attending this year; this is not including Skittles (the dog)



Related blog post: Healthcare Hero: Dr. Benjamin Gold

Pictures from today’s CCFA Fundraiser -we had about 25 GI Care for Kids staff/family attending this year; this is not including Skittles (the dog)
Related blog post: Healthcare Hero: Dr. Benjamin Gold
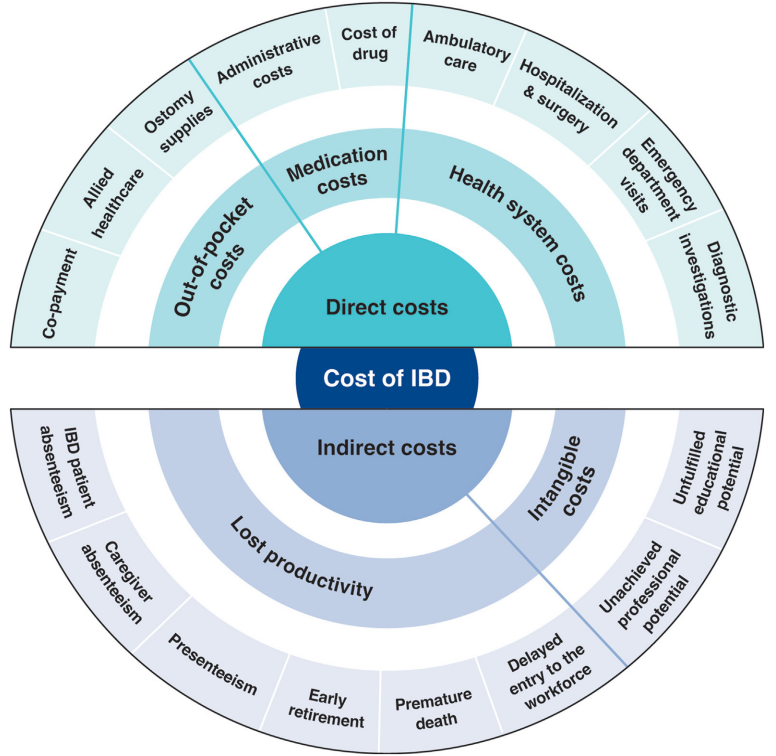
J Burisch et al. Clin Gastroenterol Hepatol 2025; 23: 386-395. Open Access! The Cost of Inflammatory Bowel Disease Care: How to Make it Sustainable
This article is a terrific review of care cost drivers in inflammatory bowel disease (IBD) but it does not actually have useful information on how to make the costs of care sustainable.
Key points:
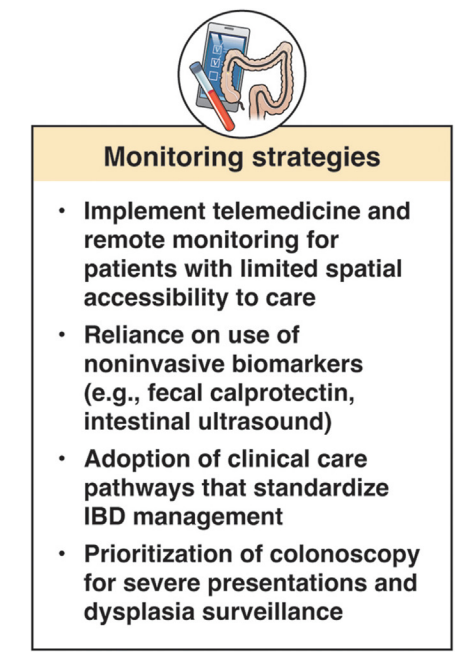
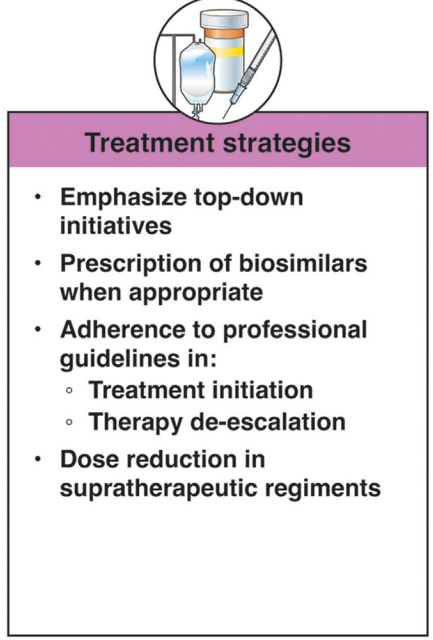
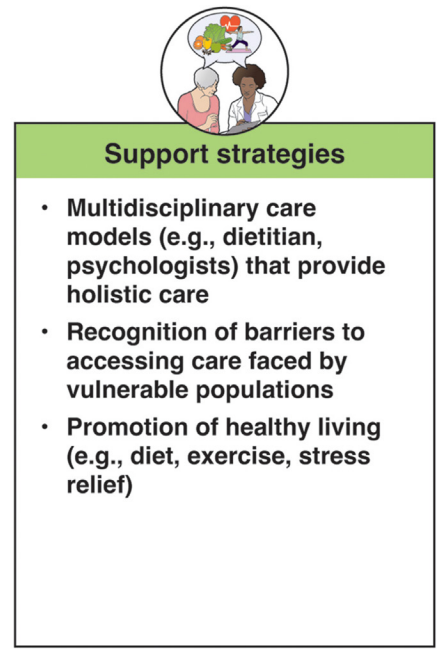
In terms of improving cost sustainability, here is what the authors propose “Strategies for cost reduction in the clinical treatment of IBD”:
My take: This article highlights the cost drivers in IBD but does not identify a path that appears to help address affordability.
This article is one of 11 articles in special issue discussing the future of IBD care.
Related blog posts:
JD Lewis et al. Clinical Gastroenterology and Hepatology. 2024; Volume 22, Issue 12, 2475 – 2486.e14. Open Access ! Provider Specialization in Inflammatory Bowel Diseases: Quality of Care and Outcomes
Methods: This was a retrospective cohort of newly diagnosed patients with IBD using data from Optum’s deidentified Clinformatics Data Mart Database (2000–2020). The study included 772 children treated by 493 providers and 2864 adults treated by 2076 providers.
Key findings:
My take: This study indicates significant treatment disparities between IBD-focused care providers and providers without an IBD focus in the care for adults, but not in the care of children. This could be related to improved collaboration among pediatric care providers, better training, and parental involvement.
In addition, this study focused on patients with newly-diagnosed disease. Treatment is more complicated in patients who have not responded to initial treatments; as such, IBD-focused providers may be more important in this population.
Related blog posts:
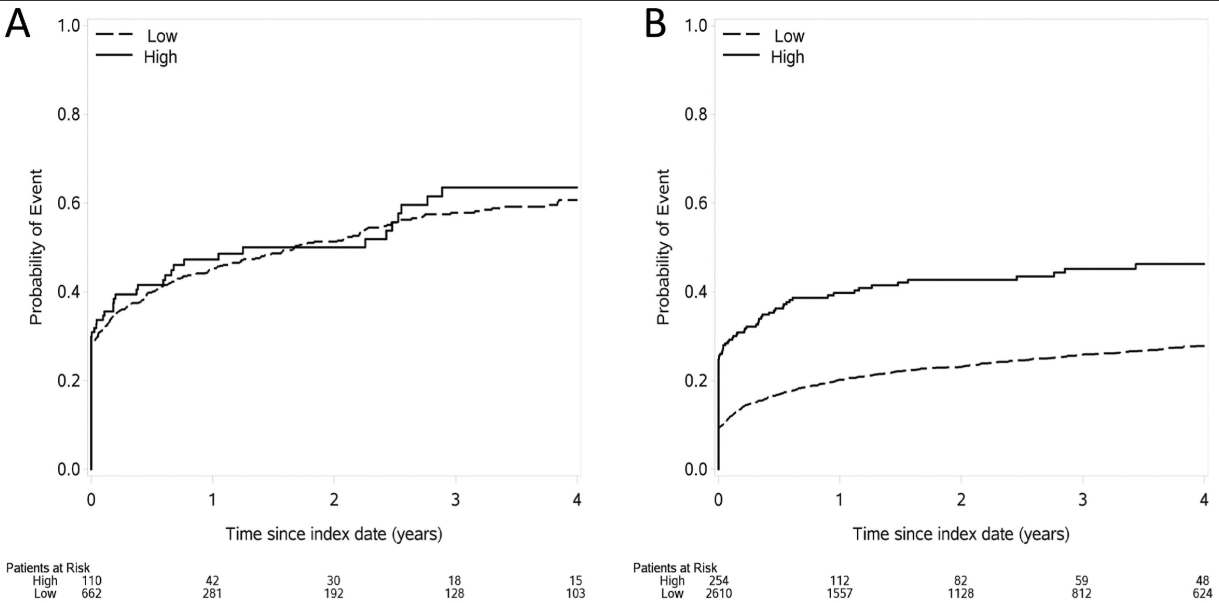
O Atia et al. Infammatory Bowel Diseases, 2025, 31, 617–624. Durability of the First Biologic in Children and Adults With Ulcerative Colitis: A Nationwide Study from the epi-IIRN
This was a nationwide Israeli study with 15,111 patients with UC, of whom 2322 (15%) received biologics, with a median follow-up of 7.0 years. The dataset includes ~98% of the Israeli population; “the accuracy of medication data is high, as the Israeli health care system provides medications almost free of charge through the HMOs, and the electronic dispensing of drugs contributes to reliable and precise data.”
Key findings:
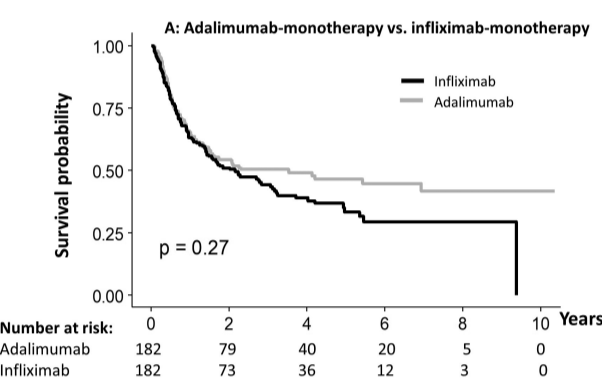
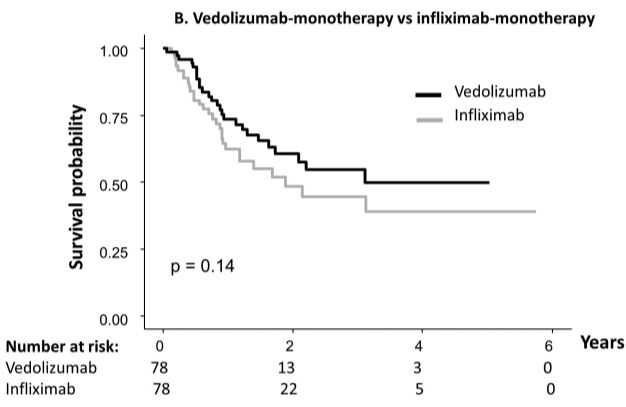
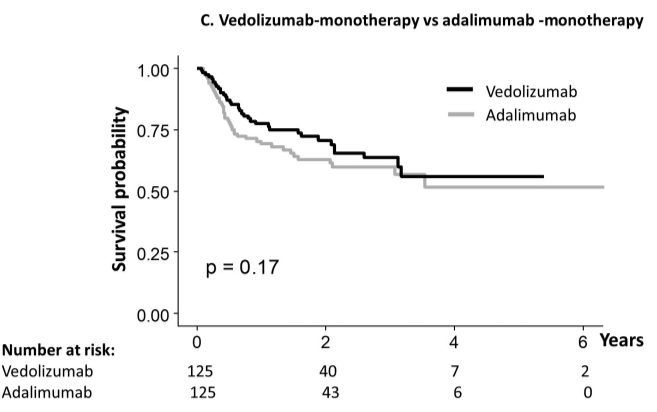
My take: When looking at the durability plots, the three main biologics in this study, infliximab, adalimumab and vedolizumab, performed similarly. Whether therapeutic drug monitoring would influence theses results is not clear. It is interesting that a recent study in the pediatric population found that combination therapy was important for adalimumab and not infliximab (see: Why Do Children Taking Adalimumab Benefit from Methotrexate Dual Therapy?)
Related blog posts:
Also, from AGA Today (3/20/25): FDA Approves Guselkumab To Treat Patients With Crohn’s Disease
HCPlive (3/20, Campbell) reports the FDA on Thursday announced the approval of “guselkumab (Tremfya) for the treatment of adults with moderately to severely active Crohn disease.” The announcement from Johnson and Johnson claims the “approval is based on data from multiple phase 3 trials, including the GALAXI trials, which found guselkumab outperformed ustekinumab (Stelara) for multiple endoscopic endpoints. The agent now boasts indications for moderately to severely active Crohn disease and moderately to severely active ulcerative colitis (UC).” This is the fourth indication for guselkumab in the US
Related blog posts:
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Congratulations to Dr. Benjamin Gold who is one of the honored heros at this year’s CCFA Take Steps. Also, congratulations to Clara Cann and Lauren Leonard who are being recognized as well.
Link: Register for Take Steps 2025 (4/26/25)
MV Vestergaard et al. . JAMA. Published online October 15, 2024. doi:10.1001/jama.2024.20429. HLA-DRB1*01:03 and Severe Ulcerative
Colitis
Background: This study aimed to identify biomarkers by conducting a Danish nationwide genome-wide association study (GWAS) on severe vs less severe ulcerative colitis.
Methods: Severe ulcerative colitis: Patients with severe ulcerative colitis were defined as having at least 1 major ulcerative colitis–related operation, at least 2 ulcerative colitis–related hospitalizations exceeding 2 days, and/or use of at least 5000 mg of systemic corticosteroids within 3 years of diagnosis
The authors utilized two source populations
The combined cohort included 4491 patients (4153 from NBS and 338 from NorDIBD) with a mean (SD) age at diagnosis of 23.3 (8.4) years; 53% of patients were female and 27% had severe disease.
Key findings:

My take: HLA-DRB1*01:03 is a low-frequency allele, carriers have a significantly higher risk of severe ulcerative colitis.
Related blog posts:
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
R Duan et al. Clin Gastroenterol Hepatol 2025; 23: 45-58. Open Access! Antibiotic Exposure and Risk of New-Onset Inflammatory Bowel Disease: A Systematic Review and Dose-Response Meta-Analysis
Twenty-eight studies involving 153,027 patients with IBD were included.
Key findings:
Some of the limitations:
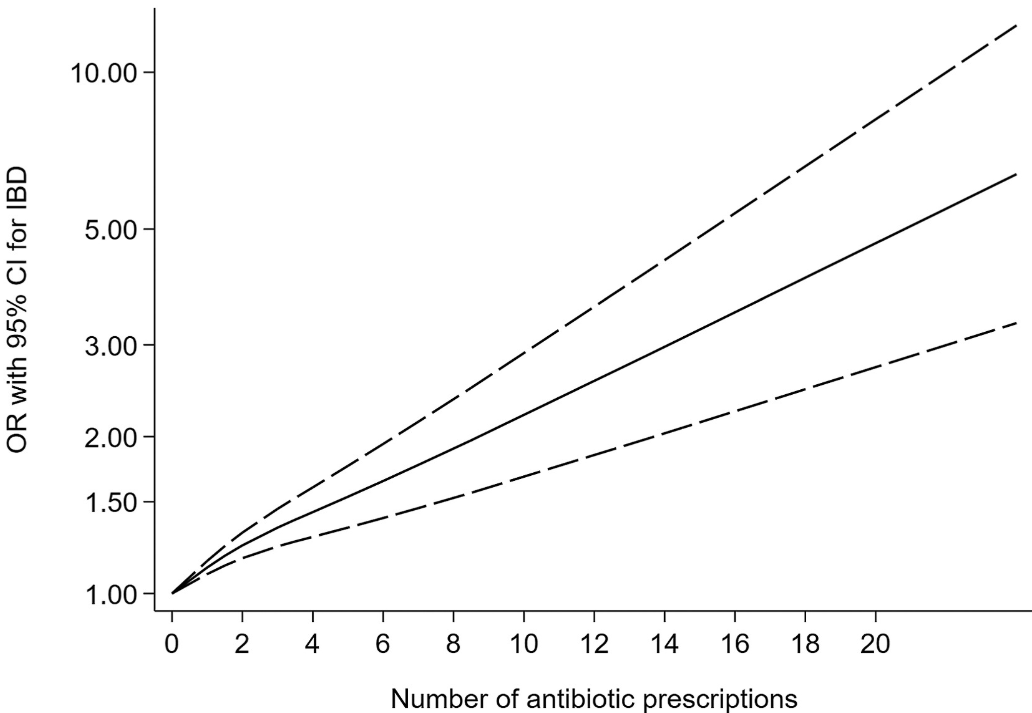
My take: This is another study showing an association between antibiotic use and new-onset IBD. While this study does not prove causation, it is another reason for good antibiotic stewardship.
Related blog posts:
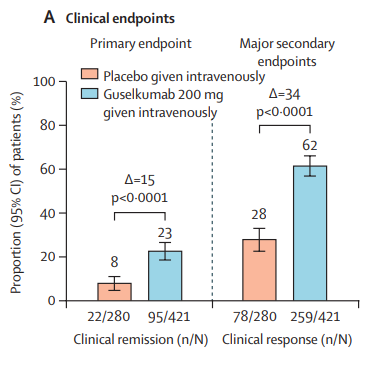
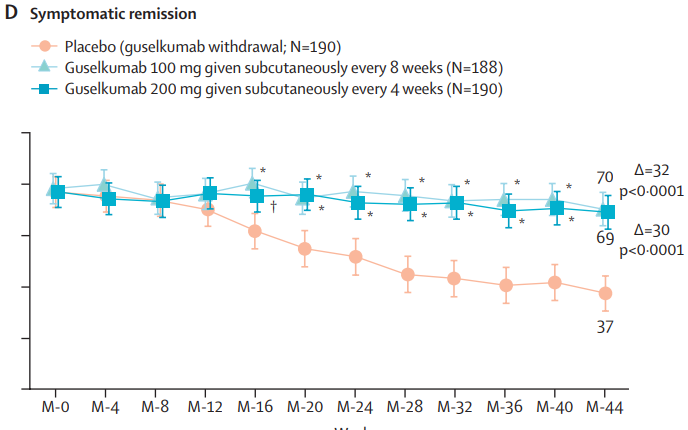
DT Rubin et al. Lancet 2024; 405: 33-49. Guselkumab in patients with moderately to severely active ulcerative colitis (QUASAR): phase 3 double-blind, randomised, placebo-controlled induction and maintenance studies
Background: “Guselkumab is a dual-acting, human IgG1, interleukin-23p19 subunit inhibitor that potently neutralises interleukin-23 and can bind to CD64.”
Methods: “Two phase 3, randomised, double-blind, placebo-controlled studies (QUASAR phase 3 induction and maintenance) included randomised and treated adults with moderately to severely active ulcerative colitis (induction baseline modified Mayo score from 5 to 9) with inadequate response or intolerance to conventional or advanced ulcerative colitis therapy.”
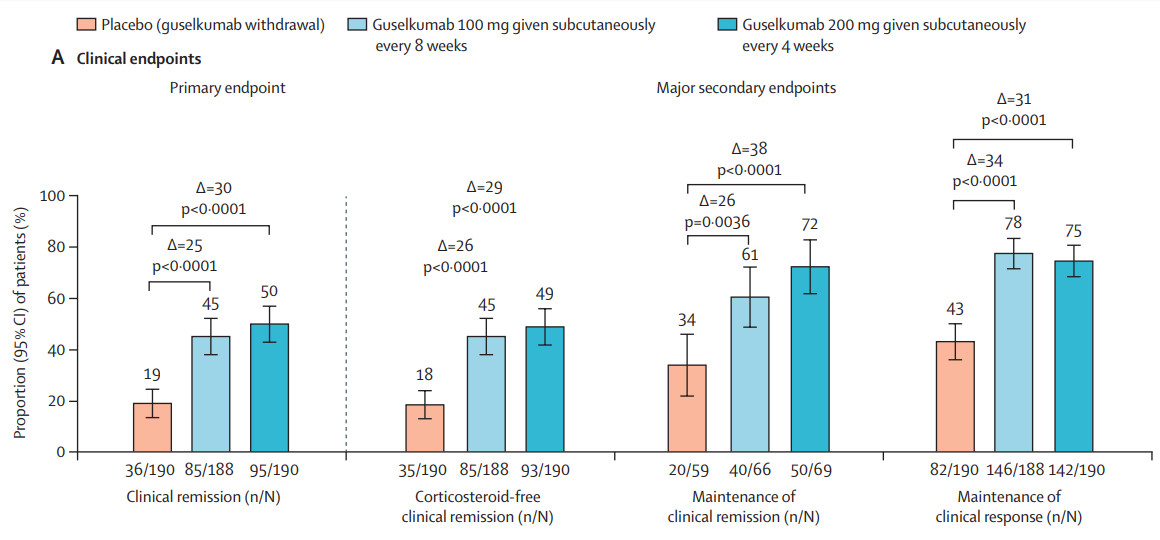
“The induction study primary population included 701 patients (guselkumab 200 mg given intravenously 60% [421 patients]; placebo 40% [280 patients]). The maintenance study primary population included 568 guselkumab induction responders randomly assigned to receive guselkumab 200 mg given subcutaneously every 4 weeks (190 [33%] patients) or 100 mg every 8 weeks (188 [33%] patients) or placebo (guselkumab withdrawal 190 [33%] patients).”
Key findings:


MAINTENANCE DATA AT 44 WEEKS
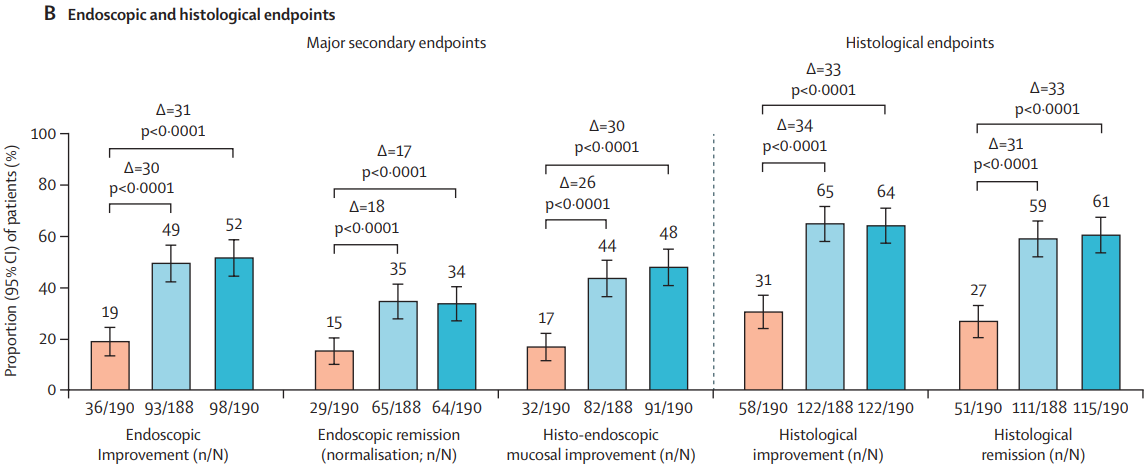
Results and Discussion points:
My take: Overall, this is a pivotal study showing that guselkumab is an effective agent for moderately to severely active ulcerative colitis in those with and without prior treatments. More head-to-head studies are needed to determine the optimal positioning of therapies for UC. Currently, AGA guidelines (AGA Living Guideline for Moderate-to-Severe Ulcerative Colitis –The Good and The Bad) suggest that guselkumab should be considered in the top tier of medications used in patients naive to biologics/advanced therapies and in the second tier for those with prior biologic treatments.
Related blog posts:
L Beidermann et al. Nutrients. 2024;16(23):4197. Open Access! Efficacy and Safety of Anthocyanin-Rich Extract in Patients with Ulcerative Colitis: A Randomized Controlled Trial
First of all: Bilberries are similar to blueberries, but have red inner flesh rather than white flesh.
Background: The authors note that some small studies have shown that anthocyanin-rich extract (ACRE), the bioactive ingredient of bilberries, has been effective for ulcerative colitis (UC)
“ACs have been associated with many protective biological effects, including anti-oxidative, anti-carcinogenic, antimicrobial, and anti-inflammatory properties [17,20,21]. Due to their phenolic structure, ACs exhibit an anti-oxidative capacity in vivo as they scavenge reactive oxygen species (ROS) [20,22], also a classical effect of 5-ASA [23]. After ingestion, ACs largely bypass absorption in the upper gastrointestinal tract, reaching the colon intact, where they are metabolized by microbiota through deglycosylation and further degraded into vanillic, protocatechuic, p-coumaric, gallic, and syringic acids (i.e., phenolic acids) [24]. ACs interrupt the pro-inflammatory signaling and are inhibitors of 5-lipoxygenase, a key enzyme implicated in the arachidonic acid pathway for the biosynthesis of active leukotrienes.”
Methods: A multi-center, randomized, placebo-controlled, double-blind study with a parallel group was conducted. Due to COVID-19’s effect on study enrollment, only 34 patients were randomized and only Eighteen ACRE and eight placebo patients could be analyzed (per protocol set)
Key finding:
The authors state that the placebo group had an unusually high response and that improved FC with ACRE patients indicates efficacy in UC.


My take: This is a negative study (despite the secondary finding of improved FC at some timepoints). Importantly, the study did not demonstrate any harms in the ACRE group. It did help me understand more about bilberries!
Related blog posts:
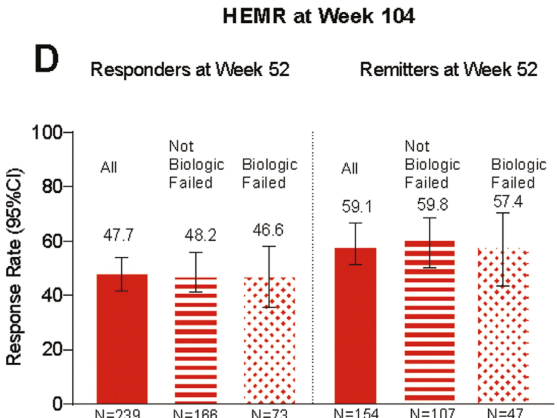
BESands, et al. Inflammatory Bowel Diseases, 2024. 30: 2024 2245–2258. Open Access! Two-Year Efficacy and Safety of Mirikizumab Following 104 Weeks of Continuous Treatment for Ulcerative Colitis: Results From the LUCENT-3 Open-Label Extension Study
In this LUCENT-3 study, the authors examined response at 2 years among patients who had response to treatment at 1 year; patients received 200 mg mirikizumab every 4 weeks. The authors stratified patients by induction response and by previous biologic exposure.
Key findings (from Figure 4):
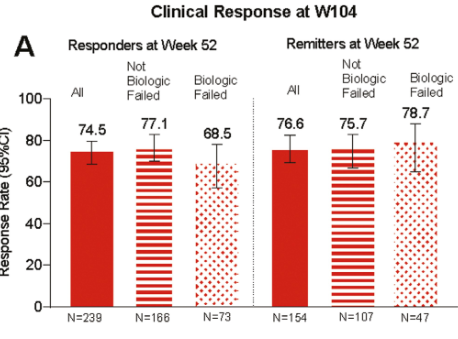

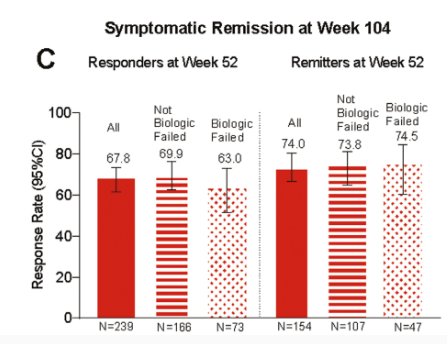
My take: It is good to see extended data for mirkizumab. Head-to-head trials, though, are needed to better determine which therapies are most effective.
Related blog posts:
