Using the ImproveCareNow prospective registry, the authors analyzed a total of 285,913 visits from 32,497 patients aged ≤ 21 years.
Key findings:
The occurrence of erythema nodousm (EN) was 1.57% and the occurrence of pyoderma gangrenosum (PG) was 0.90%. Co-occurrence of EN and PG was reported in 0.30% patients.
Both EN and PG were associated (p < 0.0001) with worse intestinal disease, lower remission, higher inflammatory markers, and extraintestinal manifestations (EIMs) arthritis and uveitis.
Limitations: “imperfect and incomplete data entry that may introduce bias. However, due to the extensive longitudinal data, we expect any bias to be minimal.”
My take: This study clarifies how common these dermatologic findings occur in pediatric patients with IBD. Prompt recognition of these disorders is important. Recently, our group cared for a 20 yo patient with inadequately-treated PG by multiple internal medicine physicians; this led to prolonged hospitalization.
Yesterday’s pumpkin -please no snide remarks about how I can now retire and become a sculptor:
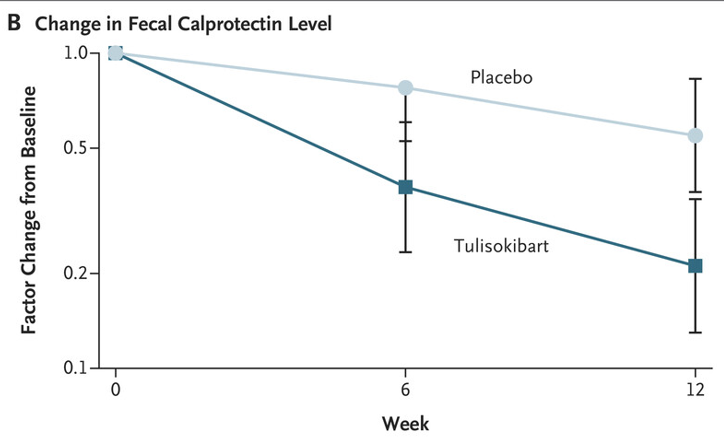
BE Sands et al. N Engl J Med 2024;391:1119-1129. Phase 2 Trial of Anti-TL1A Monoclonal Antibody Tulisokibart for Ulcerative Colitis
Background: “Several studies have implicated human tumor necrosis factor–like cytokine 1A (TL1A) in the pathogenesis of inflammatory bowel disease…Tulisokibart (formerly PRA023) is a humanized IgG1 kappa monoclonal antibody that binds to the membrane-bound and soluble forms of TL1A with high affinity and specificity. Tulisokibart prevents the interaction of TL1A and DR3, thereby suppressing type 1 and type 17 helper T-cell responses, increasing regulatory T-cell activity, and decreasing profibrotic pathways.”
Methods: (ARTEMIS-UC trial) The authors “randomly assigned patients with glucocorticoid dependence or failure of conventional or advanced therapies for ulcerative colitis to receive intravenous tulisokibart (1000 mg on day 1 and 500 mg at weeks 2, 6, and 10) or placebo. Cohort 1 included patients regardless of status with respect to the test for likelihood of response. Cohort 2 included only patients with a positive test for likelihood of response.”
“The inclusion of an integrated assessment of a panel of genetic markers as a diagnostic assay was based on the notion that patients with a propensity to overexpress TL1A might be more likely to have a response to tulisokibart than an unselected population.”
Key findings:
In the first cohort, a significantly higher percentage of patients who received tulisokibart had clinical remission than those who received placebo (26% vs. 1%), endoscopic healing (31% vs. 4%), endoscopic improvement (37% vs 6%) and clinical response (66% vs 22%)
“Among patients with a positive test for likelihood of response (cohorts 1 and 2 combined), clinical remission occurred in a higher percentage of patients who received tulisokibart than in those who received placebo (32% vs. 11%).”
Improvement in CRP and Calprotectin were noted as early as 2 weeks and 6 weeks respectively
The incidence of adverse events was similar in the tulisokibart and placebo groups
My take: Tulisokibart was effective in a group of patients with moderately to severely active ulcerative colitis who were refractory to advanced therapies.
A Simard et al. J Pediatr Gastroenterol Nutr. 2024;79:800–806. Role of ileal diversion in pediatric inflammatory bowel disease
Indications:
Severe, medically refractory colitis
Complex and medically refractory perianal disease
In combination with bowel resection for irreversible bowel damage (e.g., fistulae, abscesses, or strictures)
Diversion “provides the opportunity to reduce steroid use, improve growth and observe the natural history of the disease in a more controlled manner. It may also enhance quality of life”
My take: This is a handy article when considering ileal diversion in a patient with medically-refractory inflammatory bowel disease.
In June, risankizumab (Skyrizi) received FDA approval as a treatment for moderate to severe ulcerative colitis in adults. FDA approval relied on the data from these two randomized trials.
Methods: For the induction trial, patients were randomized 2:1 to receive 1200 mg of risankizumab or placebo administered intravenously at weeks 0, 4, and 8. For the maintenance trial, patients with a clinical response (determined using the adapted Mayo score) after intravenous treatment with risankizumab were randomized 1:1:1 to receive subcutaneous treatment with 180 mg or 360 mg of risankizumab or placebo (no longer receiving risankizumab) every 8 weeks for 52 weeks.
Key findings:
In the 12-week induction INSPIRE study with 975 patients, the clinical remission rates at week 12 were 132/650 (20.3%) for 1200 mg of risankizumab and 20/325 (6.2%) for placebo (P < .001)
In the induction trial, a greater proportion of treated patients achieved endoscopic improvement (36.5% vs. 12.1%; P < 0.00001) and endoscopic histologic mucosal improvement (24.5% vs. 7.7%; P < 0.00001) after 12 weeks
In the induction trial, a clinical response at 12 weeks was noted in 418/650 (64.3%) of risankizumab-treated patients and 116/325 (35.7%) of the placebo-treated patients
In the COMMAND maintenance trial with 548 patients, the clinical remission rates at week 52 were 72/179 (40.2%) for 180 mg of risankizumab, 70/186 (37.6%) for 360 mg of risankizumab, and 46/183 (25.1%) for placebo. Both doses were statistically-significant compared to placebo, P < .001 and P = .002, respectively
After 1 year of treatment with either maintenance dose of risankizumab, more than 40% of patients had histologic and endoscopic improvement
More than 75% of patients in the maintenance trial had a history of inadequate response to advanced therapies
My take: The published results of risankizumab for Crohn’s disease are much more impressive than the results in this study.
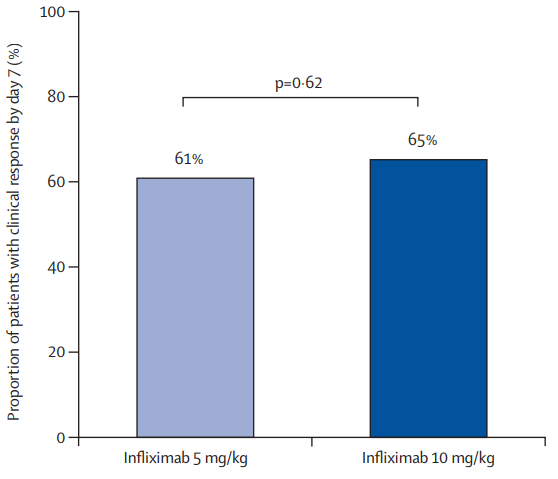
Methods: In this open-label, multicenter, randomized controlled trial, patients aged 18 years or older from 13 Australian tertiary hospitals with intravenous steroid-refractory ASUC were randomly assigned (1:2) to receive a first dose of 10 mg/kg infliximab or 5 mg/kg infliximab (randomization 1). Block randomization was used and stratified by history of thiopurine exposure and study site, with allocation concealment maintained via computer-generated randomization. Patients in the 10 mg/kg group (intensified induction strategy [IIS]) received a second dose at day 7 or earlier at the time of non-response; all patients in the 5 mg/kg group were re-randomized between day 3 and day 7 (1:1; randomization 2) to a standard induction strategy (SIS) or accelerated induction strategy (AIS), resulting in three induction groups. Patients in the SIS group received 5 mg/kg infliximab at weeks 0, 2, and 6, with an extra 5 mg/kg dose between day 3 and day 7 if no response. Patients in the AIS group received 5 mg/kg infliximab at weeks 0, 1, and 3, with the week 1 dose increased to 10 mg/kg and given between day 3 and day 7 if no response.
Thus, this was the first RCT comparing an intensified induction strategy (IIS; 10 mg/kg infliximab at weeks 0 and 1, with the second dose given earlier if no clinical response), an accelerated induction strategy (AIS; 5 mg/kg infliximab at weeks 0, 1, and 3, with the second dose increased to 10 mg/kg and given earlier if no response), and a standard induction strategy (SIS; 5 mg/kg at weeks 0, 2 and 6; with an extra 5 mg/kg dose before day 7 if no response) in steroid-refractory patients with ASUC.
Key findings:
There was no significant difference in the proportion of patients who had a clinical response by day 7 between the 10 mg/kg and 5 mg/kg groups: 65% vs 61%
In patients with a baseline albumin of less than 25 g/L, a day 7 response occurred in nine (64%) of 14 patients in the 10 mg/kg group versus 14 (45%) of 31 in the 5 mg/kg group (RR 1·43, p=0·17)
In patients with a baseline CRP of 50 mg/L or higher, a day 7 response occurred in six (60%) of ten patients in the 10 mg/kg group versus eight (42%) of 19 in the 5 mg/kg group (RR 1·39, p=0·34)
The proportions of patients with clinical response at day 14: 74% in the IIS group, 73% in the AIS group, and 68% of 44 in the SIS group.
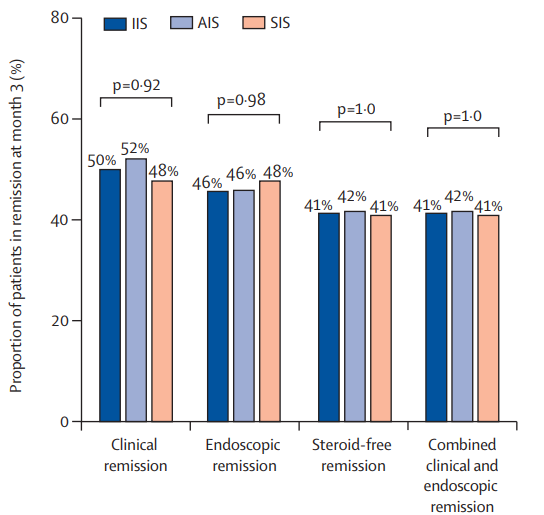
The clinical remission at month 3: 50% in the IIS group, 52% in the AIS group, and 48% in the SIS group
The steroid-free remission at month 3: 41% in the IIS group, 42% in the AIS group, and 41% in the SIS group
The endoscopic remission at month 3: 46% in the IIS group, 46% in the AIS group, and 48% in the SIS group
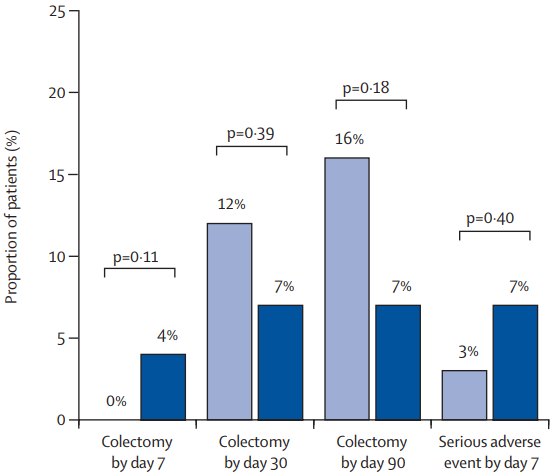
The colectomy rate at month 3: 7% in the IIS group, 19% in the AIS group, and 12% in the SIS group colectomy at month 3 were not significantly different between group (P=0.20)
The colectomy rate at month 12: 7% in the IIS group, 22% in the AIS group, and 15% in the SIS group colectomy at month 3 were not significantly different between group (p=0.13)
In post-hoc analysis of second-dose salvage strategies (among the group who had not responded at day7), a clinical response was observed in 19 (59%) of 32 patients who received a 10 mg/kg salvage dose versus nine (64%) of 14 who received a 5 mg/kg salvage dose (RR 0·92). Endoscopic remission at month 3 was observed in 11 (34%) who received 10 mg/kg salvage versus six (43%) who received 5 mg/kg salvage (RR 0·80). Colectomy by 3 months occurred in ten (31%) who received 10 mg/kg salvage compared with three (21%) who received 5 mg/kg salvage (HR 1·46)
Higher proportions of patients with clinical and biochemical remission between weeks 2 and 6 were apparent in the IIS and AIS groups versus the SIS group, but by 3 months, these differences were lost
My take: Intensified, accelerated, and standard induction regimens in the PREDICT-UC study did not result in a statistically-significant difference in clinical response by day 14 or in remission or colectomy rates by month 3. However, there are some important caveats:
There appeared to be a trend towards a lower colectomy rate in the IIS group.
There appeared to be a favorable trend towards an improved response to IIS group in those with low albumin (<25 g/L) and high CRP (>5 mg/L). The smaller numbers in these subgroups could have precluded statistical significance
Also, even the SIS group were able to receive a 4th induction 5 mg/kg dose between days 3-7 if they had not responded to treatment
In patients who had not responded to either 10 mg/kg or 5 mg/kg, a salvage dose at day 7 resulted in a >60% response rate
It is possible that a sustained strategy of more aggressive dosing (not done in this study) aided with therapeutic drug monitoring could result in better outcomes following IIS
A recent case reminded me of the quote by Helena Ravenclaw in Harry Potter: “”If you have to ask, you’ll never know. If you know, you need only ask.”
One of my colleagues recently diagnosed a teenage boy with ulcerative colitis. His past medical history was notable for ADHD. At the time of his evaluation, he was noted to have an elevated AST.
Labs:
June: AST 143, ALT 8, Hepatitis B immune
August: AST 190, ALT 10, Albumin 4.7, T protein 7.3, T bili 0.4, D bili 0.1, Alk phos 168; GGT 10, CPK 93
The concern at the time was whether his elevated AST should preclude using his ADHD medicine and whether there was an underlying liver disease. Based on the pattern of liver enzyme abnormalities, it was suspected that the patient had macro AST. A blood test was sent to the Mayo clinic and confirmed this diagnosis:
“”The sample was investigated for the presence of macro AST by polyethylene glycol (PEG) precipitation. Serum AST activity = 316 U/L. The AST result post-PEG precipitation = 22 U/L. The results obtained are positive for the presence of macro AST (93% of activity precipitated with PEG). Based on validation studies performed at the Mayo Clinic, a cut-off of >80% AST activity precipitated by PEG indicates the presence of macro AST.” This test is rarely ordered at the Mayo Clinic and is ordered as a miscellaneous test; it is not on the Mayo Clinic’s regular test menu.
Internet description of macro AST: Macro-aspartate aminotransferase (macro AST) is a rare, benign condition that causes a persistent elevation of aspartate aminotransferase (AST) levels in the blood. It’s caused by the binding of AST to immunoglobulins, which results in a high molecular weight macroenzyme that’s excreted from the serum more slowly than normal.
My take: Macro AST diagnosis is useful –it helps eliminate the concern for other conditions. Since it is quite uncommon, it is easier to think of this problem once you have seen it before.
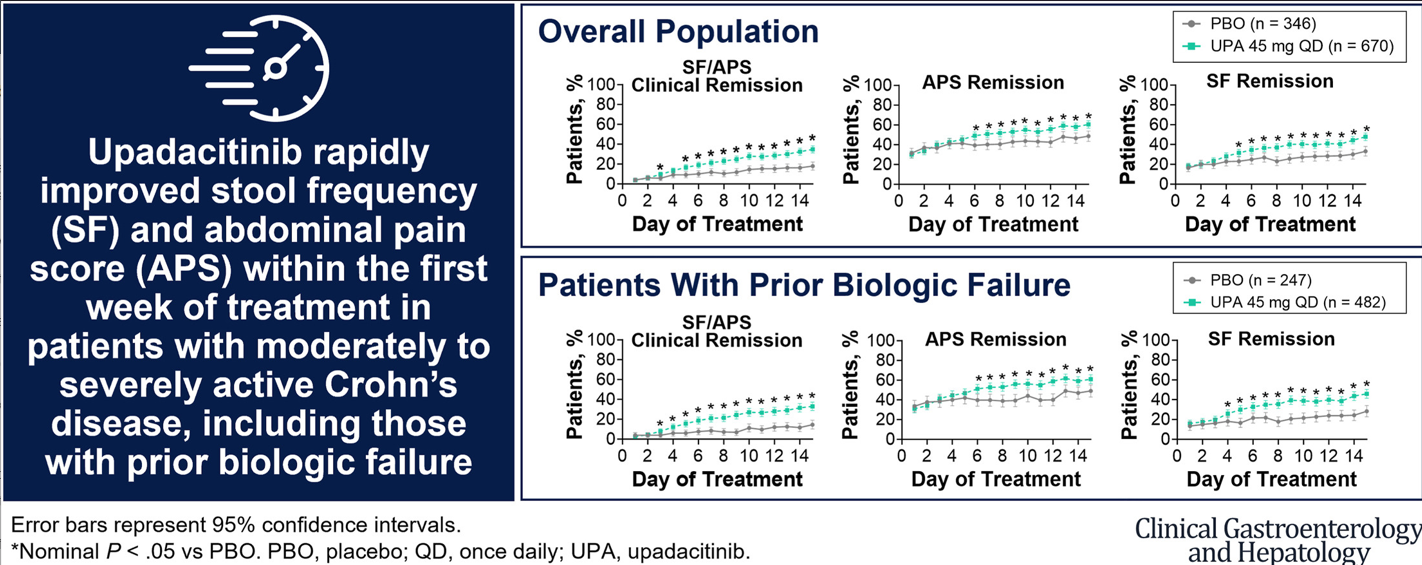
This study was a post hoc analysis included pooled data from 2 phase 3, multicenter, double-blind, 12-week induction trials (U-EXCEL and U-EXCEED) and 1 maintenance trial (U-ENDURE). The study included 1021 patients with Crohn’s disease (CD) (n = 674 UPA45; n = 347 PBO).
Key findings:
Upadacitinib 45 mg taken once daily resulted in rapid relief from CD symptoms within 5 to 6 days of treatment initiation and improved clinical outcomes starting at week 2.
The present analysis demonstrates symptomatic relief as early as day 5 to 6 for patients receiving UPA, with 16.7% of patients experiencing daily SF/APS clinical remission by day 5.
The first achievement of daily stool frequency/abdominal pain score (SF/APS) clinical remission occurred earlier with UPA45 (median, 13 d) vs PBO (median, 32 d)
Patients treated with UPA45 showed improved rates of SF/APS clinical remission (21.1% UPA45 vs 8.9% PBO) and clinical response (58.8% UPA45 vs 37.9% PBO) starting at week 2 (both P ≤ .01).
In their discussion, the authors note that time to response to treatment with upadacitinib compares favorably to other advanced therapies:
“Vedolizumab resulted in symptomatic improvement within 2 to 4 weeks of treatment initiation16; ustekinumab led to clinical response and remission at week 3 or 6, depending on the dose.17 Similarly, of the time points analyzed, clinical response and/or clinical remission was observed as early as week 2 for risankizumab, 5 infliximab,18 and certolizumab pegol,19 and as early as week 1 for adalimumab.20,21“
My take: The rapid response seen in many patients indicate that upadacitinib can be a steroid-sparing therapy in patients with Crohn’s disease.
Key findings: Among the 975 patients with moderate to severe ulcerative colitis, analyzed in the induction trial, 1200 mg of risankizumab significantly increased the rates of clinical remission at 12-week follow-up compared with placebo (20.3% vs 6.2%, respectively). Among 548 patients included in the primary efficacy analysis for the maintenance trial, 180 mg of risankizumab and 360 mg of risankizumab significantly increased the rates of clinical remission (40.2% and 37.6%, respectively) compared with placebo (25.1%).
KA Hommel et al. JPGN 2024; 78:1273–1278. Pilot and feasibility of the SMART IBD mobile app to improve self-management in pediatric inflammatory bowel disease
The Self‐Management Assistance with Recommended Treatment (SMART) IBD app –Key findings:
Patients rated the app quality as good and accessed the app adequately overall, with some pages being used often.
Medication adherence increased over the course of the study and was associated with sleep duration, mood, and stool consistency and blood content.
My take: IBD Management apps could be quite helpful, especially for teens and young adults.
S Hsiang et al. Inflammatory Bowel Diseases, Volume 30, Issue 8, August 2024, Pages 1284–1294, https://doi.org/10.1093/ibd/izad166. Safety, Effectiveness, and Treatment Persistence of Subcutaneous Vedolizumab in IBD: A Multicenter Study From the United Kingdom
Methods: IBD patients (n=563) on IV vedolizumab across 11 UK sites agreed to transition to SC injections or otherwise continued IV treatment
Key findings:
Data from 563 patients, demonstrated no differences in disease activity, remission rates, and quality of life between the SC and IV groups at all time points
Drug persistence at week 52 was similar (81.1% vs 81.2%; P = .98)
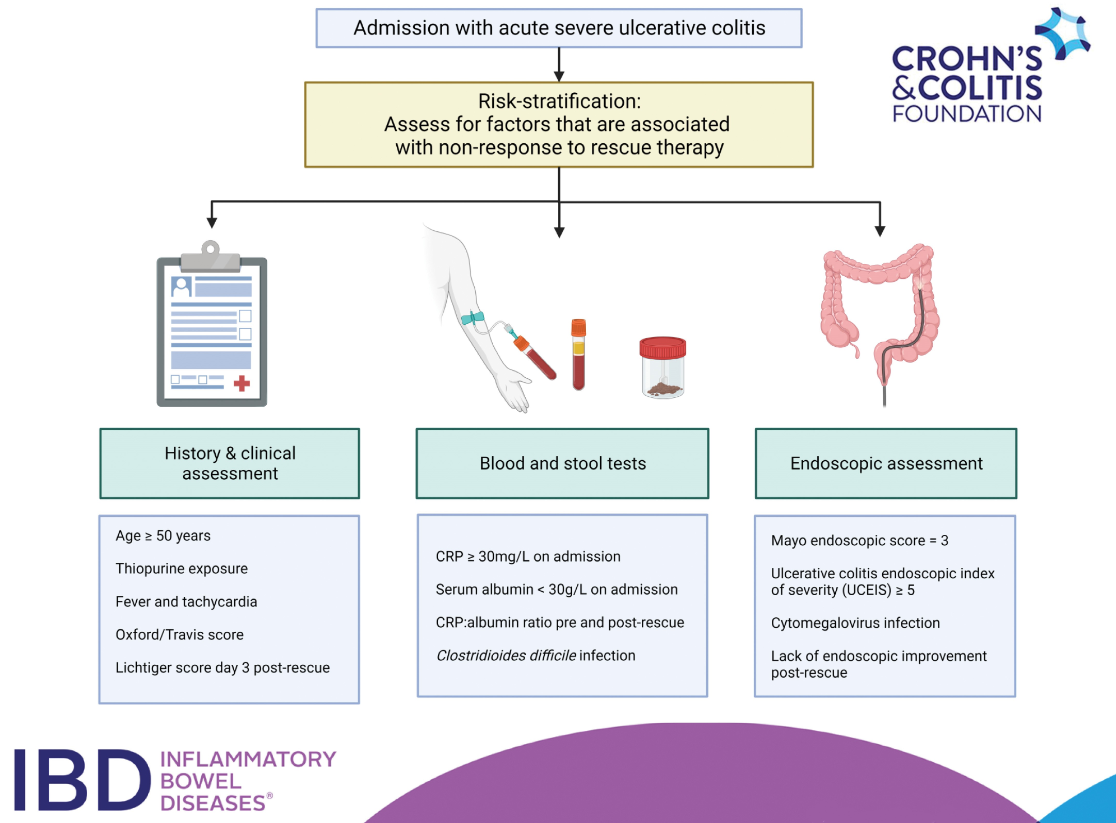
CFD Li Wai Suen, et al. Inflammatory Bowel Diseases, Volume 30, Issue 8, August 2024, Pages 1389–1405, https://doi.org/10.1093/ibd/izad183. Factors Associated With Response to Rescue Therapy in Acute Severe Ulcerative Colitis
This systematic review identified 101 completed studies were eligible for inclusion.
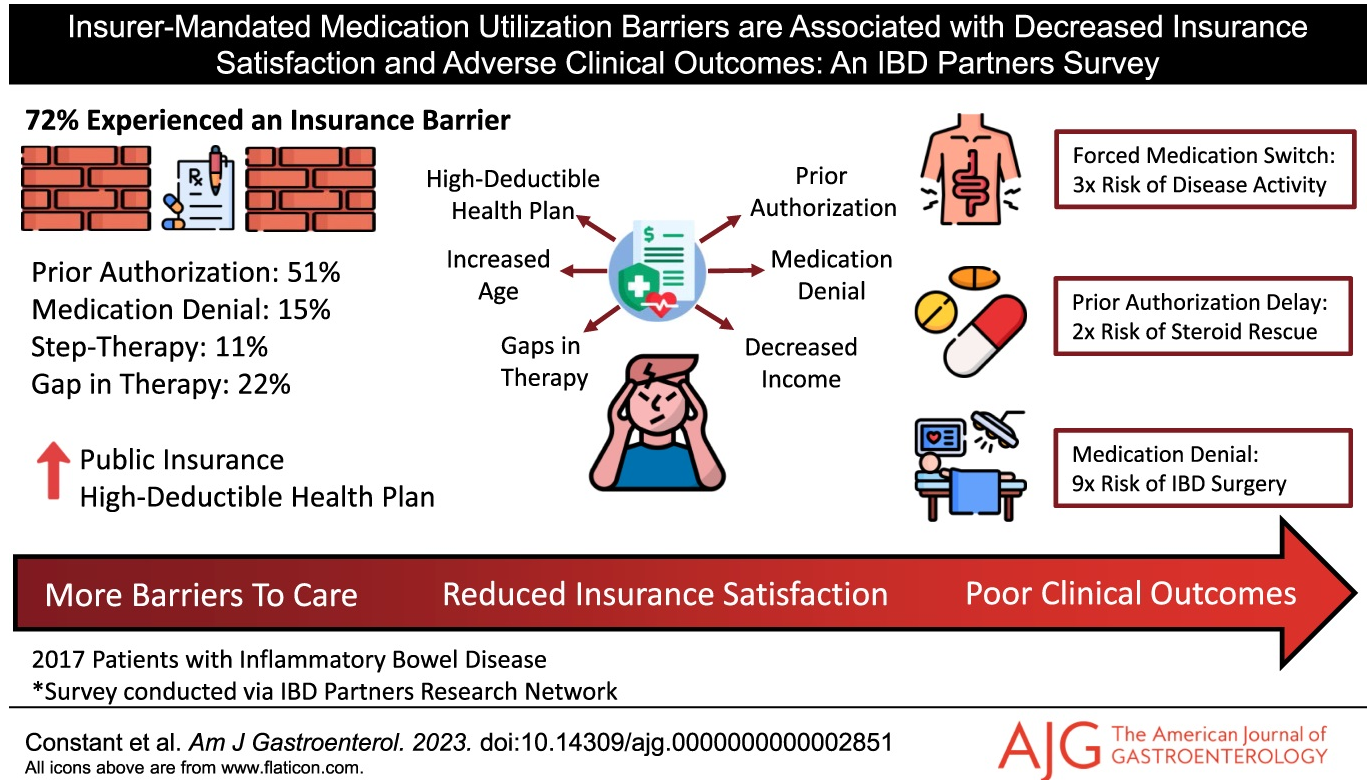
Key findings: In this longitudinal survey with 2017 patients, 72% experienced an insurer-mandated barrier, most commonly prior authorizations (51%). Fifteen percent were denied an IBD medication by their insurer, 22% experienced an insurance-related gap in therapy, and 8% were forced by their insurer to switch from an effective medication. Several insurance barriers were linked to negative downstream clinical outcomes, including prior authorizations associated with corticosteroid rescue (odds ratio [OR] 2.24]), forced medication switches associated with continued disease activity (OR 3.28), and medication denials associated with IBD-related surgery (OR 8.92).
FDA IBD Workshop -Take-Home PointsOff-label does not equate to experimentalFDA Statement: The FD&C Act does not, however, limit the manner in which a physician may use an approved drug. Once a product has been approved for marketing, a physician may prescribe it for uses or in treatment regimens or patient populations that are not included in approved labeling. Such “unapproved” or, more precisely, “unlabeled” uses may be appropriate and rational in certain circumstances, and may, in fact, reflect approaches to drug therapy that have been extensively reported in medical literature
In this phase 2 randomised, multicentre, double-blind trial with 309 adults, the authors report on the safety and efficacy of subcutaneous guselkumab maintenance regimens to week 48 in the GALAXI-1 study. Key findings:
“At week 48, the numbers of patients with CDAI clinical remission were 39 (64%) in the guselkumab 200→100 mg group, 46 (73%) in the guselkumab 600→200 mg group, 35 (57%) in the guselkumab 1200→200 mg group, and 37 (59%) in the ustekinumab group.”
“Eendoscopic remission was seen in 11 (18%), 11 (17%), 20 (33%), and four (6%) patients, respectively.”
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.