I am a pediatric gastroenterologist at GI Care for Kids (previously called CCDHC) in Atlanta, Georgia. The goal of my blog is to share some of my reading in my field more broadly. In addition, I wanted to provide my voice to a wide range of topics that often have inaccurate or incomplete information.
Before starting this blog in 2011, I would tear out articles from journals and/or keep notes in a palm pilot. This blog helps provide an updated source of information that is easy to access and search, along with links to useful multimedia sources.
I was born and raised in Chattanooga. After graduating from the University of Virginia, I attended Baylor College of Medicine. I completed residency and fellowship training at the University of Cincinnati at the Children’s Hospital Medical Center. I received funding from the National Institutes of Health for molecular biology research of the gastrointestinal tract.
During my fellowship, I had the opportunity to work with some of the most amazing pediatric gastroenterologists and mentors. Some of these individuals included Mitchell Cohen, William Balistreri, James Heubi, Jorge Bezerra, Colin Rudolph, John Bucuvalas, and Michael Farrell. I am grateful for their teaching and their friendship. During my training with their help, I received a nationwide award for the best research by a GI fellow.
I have authored numerous publications/presentations including original research, case reports, review articles, and textbook chapters on various pediatric gastrointestinal problems. In addition, I have been recognized by Atlanta Magazine as a "Top Doctor" in my field multiple times.
Currently, I am the vice chair of the section of nutrition for the Georgia Chapter of the American Academy of Pediatrics. In addition, I am an adjunct Associate Clinical Professor of Pediatrics at Emory University School of Medicine. Other society memberships have included the North American Society for Pediatric Gastroenterology Hepatology and Nutrition (NASPGHAN), American Academy of Pediatrics, the Food Allergy Network, the American Gastroenterology Association, the American Association for the Study of Liver Diseases, and the Crohn’s and Colitis Foundation.
As part of a national pediatric GI organization called NASPGHAN (and its affiliated website GIKids), I have helped develop educational materials on a wide-range of gastrointestinal and liver diseases which are used across the country. Also, I have been an invited speaker for national campaigns to improve the evaluation and treatment of gastroesophageal reflux disease, celiac disease, eosinophilic esophagitis, hepatitis C, and inflammatory bowel disease (IBD). Some information on these topics has been posted at my work website, www.gicareforkids.com, which has links to multiple other useful resources.
I am fortunate to work at GI Care For Kids. Our group has 17 terrific physicians with a wide range of subspecialization, including liver diseases, feeding disorders, eosinophilic diseases, inflammatory bowel disease, cystic fibrosis, DiGeorge/22q, celiac disease, and motility disorders. Many of our physicians are recognized nationally for their achievements. Our group of physicians have worked closely together for many years. None of the physicians in our group have ever left to join other groups. I have also worked with the same nurse (Bernadette) since I moved to Atlanta in 1997.
For many families, more practical matters about our office include the following:
– 14 office/satellite locations
– physicians who speak Spanish
– cutting edge research
– on-site nutritionists
– on-site psychology support for abdominal pain and feeding disorders
– participation in ImproveCareNow to better the outcomes for children with inflammatory bowel disease
– office endoscopy suite (lower costs and easier scheduling)
– office infusion center (lower costs and easier for families)
– easy access to nursing advice (each physician has at least one nurse)
I am married and have two sons (both adults). I like to read, walk/hike, bike, swim, and play tennis with my free time.
I do not have any financial relationships with pharmaceutical companies or other financial relationships to disclose. I have helped enroll patients in industry-sponsored research studies.
Methods: A retrospective cohort study was performed on patients (n=518) ages 0 to 21 hospitalized at Johns Hopkins Hospital between 1983 and 2010 with an ICD-9 discharge diagnosis of ascites
Key findings:
Among the 3 age groups (0–5, 6–12, and 13–21), the 0 to 5 age group experienced significantly increased length of stay (LOS) (P < 0.001) and mortality (P = 0.027).
Ascites etiology of veno-occlusive disease (VOD) and the presence of hydrothorax or thrombocytopenia was also significantly associated with increased LOS.
Ascites with the etiology of congestive hepatopathy and the presence of grade 3 ascites, hepatic encephalopathy, hepatorenal syndrome, hydrothorax, hyponatremia, and thrombocytopenia were associated with increased mortality.
Black pediatric patients with ascites have an increased risk of mortality
Zack Cooper, an economist at Yale School of Public Health, and his colleague, Martin Gaynor, have crunched the numbers on hospitals using the government’s preferred way of measuring market concentration, and they’ve found that about 80% of America’s hospital markets are now “highly concentrated.”…
The research clearly shows, Cooper says, that growing monopolization has raised prices for patients. Less competition means hospitals can charge higher prices and get away with it. They can pay lower wages and get away with it. And they can provide worse care and get away with it. “We want firms to compete and be incentivized to raise their quality to attract more consumers, and the more that hospitals merge, the less sharp those incentives become,” Cooper says. “We have evidence that death rates are literally higher in markets where hospitals face less competition.”…
The bizarre part of all this is that many of these monopolizing hospitals are technically considered “nonprofits.” … instead of making profits that are distributed to shareholders, nonprofit hospitals take the extra money they make and use it for executive compensation and buying shiny stuff.
Using a selected sample from a database with >62 million patients, this retrospective cohort study determined the rates of colorectal cancer among patients with IBD. Key finding:
Among the IBD cohort, patients treated with anti-TNF agents were less likely to develop CRC; patients with Crohn’s disease: odds ratio, 0.69; 95% confidence interval, 0.66-0.73; P < 0.0001 vs patients with ulcerative colitis: odds ratio, 0.78; 95% confidence interval, 0.73-0.83; P < 0.0001.
My take: This study found an association between anti-TNF therapy and a reduced risk of CRC in patients with IBD.
Using the National Health Interview survey (2015), the authors identified individuals with self-reported IBD and assessed national estimates of financial toxicity. Key findings:
23% reported financial hardships due to medical bills, 16% of patients reported cost-related medication nonadherence, and 31% reported cost-reducing behaviors
Approximately 62% of patients reported personal and/or health-related financial distress, and 10% of patients deemed health care unaffordable
Inflammatory bowel disease was associated with 1.6 to 2.6 times higher odds of financial toxicity across domains compared with patients without IBD
My take: In addition to the physical and emotional toll of having IBD, there is also significant financial hardships for many.
Methods: Data from 6 ustekinumab phase 2/3 CD and UC studies were pooled, and safety was evaluated through 1 year; this included 2574 patients (1733 patient-years of follow-up)
Key Safety findings –Events per 100 patient years -placebo vs ustekinumab respectively:
Major cardiovascular events were rare with 2 in placebo group 0.34 and 2 in the ustekinumab group 0.12
Morekey findings:
No cases of progressive multifocal leukoencephalopathy or reversible posterior leukoencephalopathy
Antibodies to ustekinumab were identified in 3.6% of patients
My take: This study showed similar safety between ustekinumab and placebo, but is limited by short followup. The authors note that 5-year data from ustekinumab’s use with psoriasis has found no safety signals for malignancy.
This cross-sectional study with 229 patients examined the relationship between inflammatory bowel disease (IBD) activity and resilience based on the Connor-Davidson Resilience Scale questionnaire (high resilience score ≥ 35).
Key findings:
High resilience was noted in 27% of patients with UC and 21.5% of patients with CD.
Among patients with UC, those with high resilience had a mean Mayo score of 1.54, and those with low resilience had a mean Mayo score of 4.31, P < 0.001.
Among patients with CD, those with high resilience had a mean HBI of 2.31, and those with low resilience had a mean HBI of 3.95, P = 0.035.
In multivariable analysis, high resilience was independently associated with lower disease activity in both UC (P < 0.001) and CD (P = 0.037) and with higher QoL (P = 0.016).
High resilience was also associated with fewer surgeries (P = 0.001) among patients with CD.
Reading this study, made me think of Galen’s assertion about a different treatment, circa 100 AD: “All who drink of this remedy recover in a short time except those whom it does not help, who all die. It is obvious, therefore, that it fails only in incurable cases.” In the case of this study, the remedy is resiliency.
This study is intriguing and adds to the literature that mental health and IBD may be a two-way street: mental health may affect IBD and IBD activity may affect mental health. However, it is difficult to prove causation in a cross-sectional study. Reverse causation is possible; that is higher disease burden may result in lower resilience.
Also, it is not clear to me that resilience is a particularly modifiable factor. Some may interpret this study in a ‘blame the victim’ mode. I think a lot of individuals would think they are resilient but most do not know until they face a difficult situation. Perhaps, Mike Tyson’s assertion is more apt: “Everyone has a plan until they get punched in the mouth.”
My take: This study does not prove that resilience helps prevent IBD activity, though being resilient is nice if you have it.
Plus one: JR Rosh et al. J Crohns Colitis. 2021 May 26; jjab089. doi: 10.1093/ecco-jcc/jjab089. (EPUB). Ustekinumab in Pediatric Patients with Moderately to Severely Active Crohn’s Disease Pharmacokinetics, Safety, and Efficacy Results from UniStar, a Phase 1 Study This was a “multicentre, 16-week, double-blind induction dose-ranging study (NCT02968108), patients aged 2-<18 years; patients were randomized (1:1) to one of 2 weight range-based intravenous induction doses: 130mg vs 390mg in patients ≥40kg and 3mg/kg vs 9mg/kg in patients <40kg. At week 8, all patients received a single subcutaneous ustekinumab maintenance dose of 90mg in patients ≥40kg or 2mg/kg in patients <40kg..” (Kudos to my partner, Stanley Cohen, one of the authors)
Key finding: Pharmacokinetics were similar to those in adults with Crohn’s disease. However, serum ustekinumab concentrations were lower among those with body weight <40kg…These results suggest a different dosing regimen may be required for patients <40kg
A long time ago I heard a joke from a mentor about how can you tell if a person is an optimist. An optimist is a person who finds a pile of manure under the tree on Christmas morning and declares: ‘Oh boy, I’m getting a pony.’
Researchers who are trying to identify oral treatments for celiac disease are probably true optimists. Yet, despite my skepticism, a recent study (D Schuppan et al. NEJM 2021; 385: 35-45. A Randomized Trial of a Transglutaminase 2 Inhibitor for Celiac Disease) provides the best proof yet that an oral treatment may be helpful.
In this 6-week randomized, double-blind, placebo-controlled study with 159 participants, treatment with ZED1227, a selective oral transglutaminiase 2 inhibitor reduced histologic injury compared to placebo; all patients were receiving a diet with 3 grams of daily gluten. Key findings:
Treatment with ZED1227 at all three dose levels attenuated gluten-induced duodenal mucosal injury. The estimated difference from placebo in the change in the mean ratio of villus height to crypt depth from baseline to week 6 was 0.44 (95% confidence interval [CI], 0.15 to 0.73) in the 10-mg group (P=0.001), 0.49 (95% CI, 0.20 to 0.77) in the 50-mg group (P<0.001), and 0.48 (95% CI, 0.20 to 0.77) in the 100-mg group (P<0.001)
The estimated differences from placebo in the change in intraepithelial lymphocyte density were −2.7 cells per 100 epithelial cells (95% CI, −7.6 to 2.2) in the 10-mg group, −4.2 cells per 100 epithelial cells (95% CI, −8.9 to 0.6) in the 50-mg group, and −9.6 cells per 100 epithelial cells (95% CI, −14.4 to −4.8) in the 100-mg group
Adverse events were similar to placebo; 3 (8%) patients in the 100 mg group developed a rash
The need for a treatment besides a gluten-free diet is significant; among adults, 40-50% do not achieve mucosal healing/recovery despite GFD institution; in addition, the diet is difficult and costly.
My take: I think it is still a long journey to find an effective & safe oral treatment for celiac disease.
F Wang et al JPGN 2021; 73: 17-22. Glucocorticoids Improve Enteral Feeding Tolerance in Pediatric Short Bowel Syndrome With Chronic Intestinal Inflammation In this retrospective study with 15 patients who had histologically-confirmed chronic intestinal inflammation, glucocorticoids (budesonide or prednisone) were associated with clinical improvement. Key findings: 7 of the 15 patients gained enteral autonomy. 6 of 7 of those had eosinophilic infiltrates as part of their histologic findings. 11 of 15 had a reduction in parenteral calories.
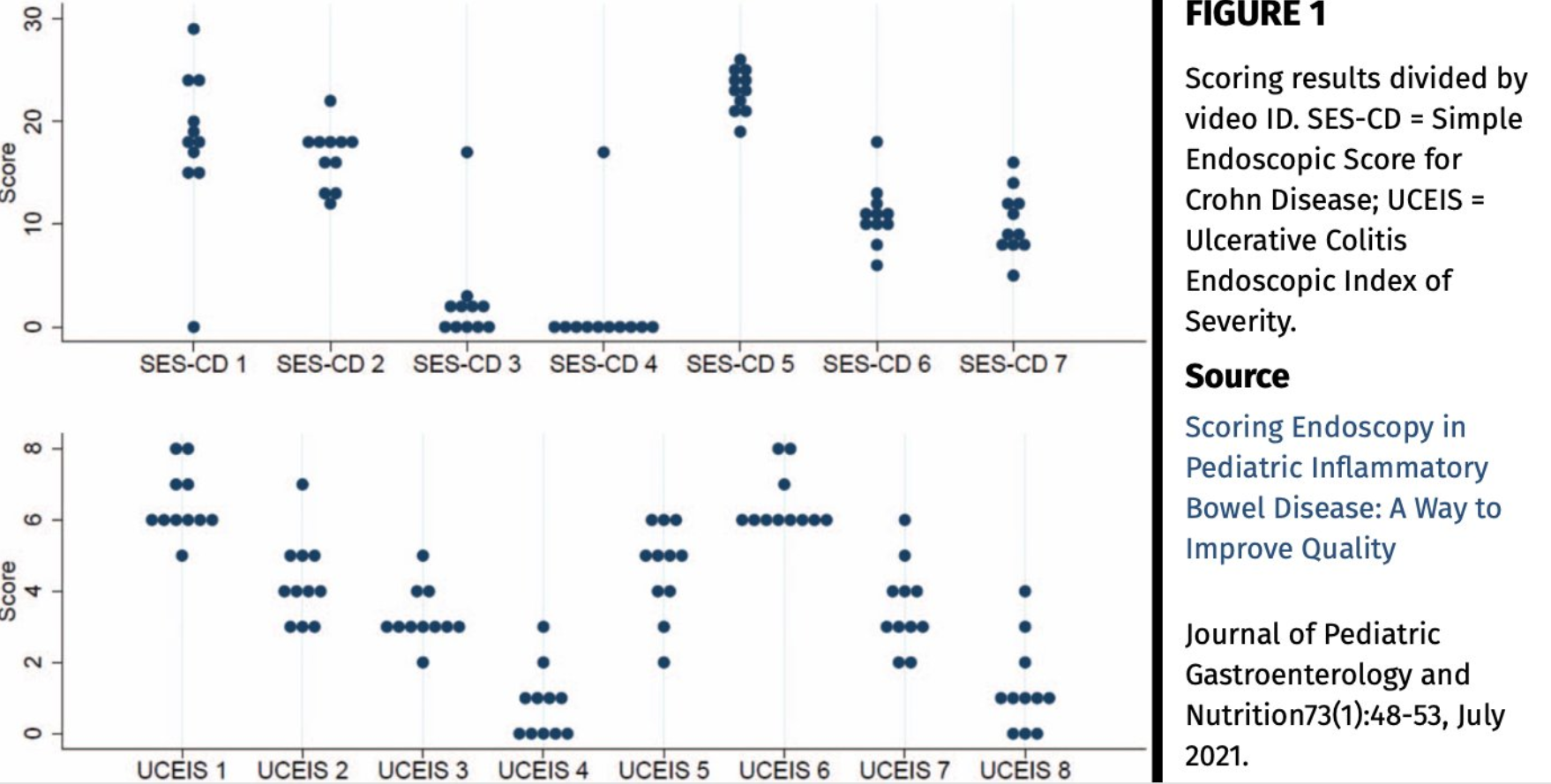
L Norsa et al JPGN 2021; 73: 48-53. Scoring Endoscopy in Pediatric Inflammatory Bowel Disease: A Way to Improve Quality This study showed very poor agreement between 11 pediatric GIs in evaluating videos of 15 endoscopies (see below). Key finding: Intraclass correlation was 0.298 (95% confidence interval [CI]: 0.13–0.55) for ulcerative colitis (UC) and 0.266 (0.11–0.52) for Crohn disease (CD). My take: This study indicates either a need for rigorous training of endoscopists and/or need for AI review of endoscopy.
NY Times 7/2/21: Full text: For Surprise Medical Bills, It’s the Beginning of the End Key issues for regulators: define a standard price for out-of-network care, determine what hospitals and doctors will need to do to notify patients they are not in their insurance network, and establish a complaint system for consumers who believe they were illegally billed.
This single-center retrospective study with 43 patients (over 11 year timeframe) identified etiology and outcomes for neonatal acute liver failure (NALF).
Key findings:
Etiologies included viral infection (23%), gestational alloimmune liver disease with neonatal hemochromatosis (GALD-NH) (21%), cardiac-associated ischemia (16%), other ischemia (14%), genetic etiologies (9%), Trisomy 21-associated myelodysplasia (TAM) (7%), hemophagocytic lymphohistiocytosis (HLH) (2%), and not identified (7%)
Infants with viral etiologies had the highest alanine aminotransferase (ALT) at presentation (1179 IU/L, interquartile range [IQR] 683–1585 IU/L) in contrast to low levels in GALD-NH (23 IU/L, IQR 18–64 IU/L)
Across all etiologies, only 33% were alive at 1 year
Among laboratory values at presentation, alpha-fetoprotein (AFP) was significantly higher in patients that survived with their native liver (P = 0.04)
Figure 4 provides a helpful management algorithm for NALF. Figure 4 is similar to the slide below (shared by lead author).
-Consider empiric acyclovir in those with INR >/= 2.0 in the first 30 days of life
-In those with normal to low elevation of aminotransferases, consider empiric IVIG while undergoing workup. Part of workup should include either MRI or lip biopsy for GALD
-In those with moderate to severe elevation of aminotransferases, workup should include assessment for viral, HLH and genetic etiologies. Fulminant viral hepatitis or HLH likely with Ferritin levels >10,000. Hypoglycemia and hyperammonemia is suggestive of metabolic/mitochondrial disorder
-Liver biopsy may be needed if etiologies not identified
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
65% of respondents (n=238 of 2300 responded to survey) perform repeat endoscopy to assess for endoscopic remission in pediatric IBD as part of routine clinical practice (usually 9 to 12 months later)
“Symptoms are not sufficient to follow IBD patients” was reported by 82% of those who repeat endoscopy
“I perform endoscopy based on clinical, biomarker, and/or imaging trends” was reported by 81% of those who do not repeat endoscopy
In those inclined to do repeat endoscopy (n=134 total), the authors state there was a significant difference based on years in practice but this is difficult to discern based on the data presented in Table 1; the numbers in both groups are much greater than the number of total patients in each group. They state in the repeat endoscopy group (n=134), the practitioner experience was n=58 (1-5 yrs), n=43 (6-10 yrs), n= 34 (11-15 yrs), and 70 (>15 yrs) and the “no repeat group” (n=67 total) was n=43 (1-5 yrs), n=33 (6-10 yrs), n=21 (11-15 yrs), and n=37 (>15 yrs). Apparently, according to the discussion, those in practice more than 15 years were less likely to recommend a ‘treat-to-target’ endoscopy.
There is also a discrepancy in the report with regard to ImproveCareNow participation, stated to be 63% in the abstract and 71% in the results section
Discussion: I would propose that the first part of a journal club start with these two lines from the discussion: “As the paradigm of clinical endpoints has evolved in the management of IBD, there has been a shift from using clinical symptoms to drive major therapeutic decisions to using endoscopic assessment. This lag time to adopt new practices in medicine has been highlighted in research demonstrating the slow adoption of new clinical practices by physicians, possibly related to the difficulty with “unlearning” common practices and shifting to new ones.” As an aside, 77% of the survey respondents were in an academic practice; it would be fun to see how the section chief views this assertion.
While the majority of survey respondents supported repeat endoscopy in all patients, the discussion point above is making a different distinction (“drive major therapeutic decisions”). I think a much higher proportion of practitioners would endorse endoscopy prior to major therapeutic decisions. However, with regard to supporting more widespread routine followup in all of those in clinical remission, the discussion references data from a single retrospective pediatric cohort study with 104 patients (Inflamm Bowel Dis 2017; 23: 1447-1453), that 30% of patients in clinical remission had active disease on endoscopy.
My take: As alluded to in the conclusion, long-term data from prospective studies are needed to determine the benefit (or lack of benefit) of followup endoscopy, especially in patients with combined clinical/biomarker remission.