

Author Archives: gutsandgrowth
Another Day in the US: School Deaths Related to Firearms
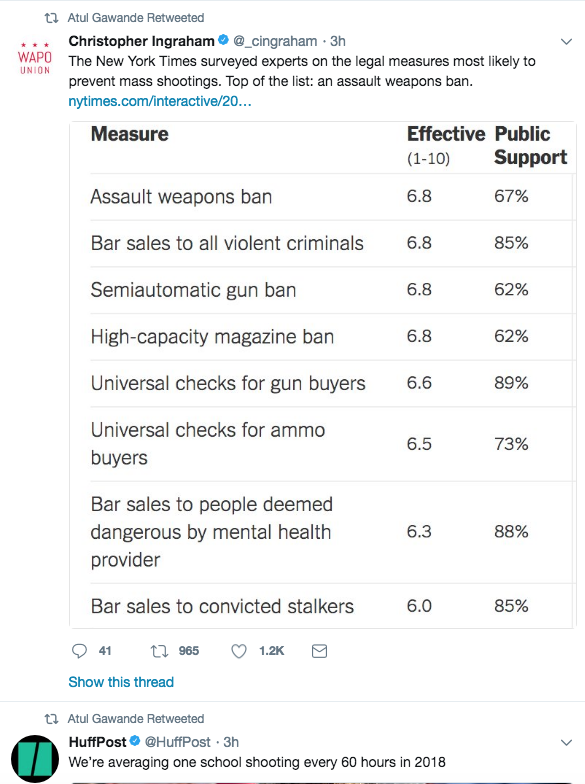
Between 2001-2013, gun related deaths exceeded the total number of deaths from AIDS, terrorism, war, and illegal drug overdoses combined (according to Vox -see Firearm Mortality in U.S). Here are some tweets in reaction to yesterday’s tragic events.

Link to The Onion commentary: ‘No Way To Prevent This’
Related blog posts:
- Firearm Mortality -Tragic Inertia
- Is It OK for Pediatricians to try to Prevent Firearm Injuries? Focus on Child Safety –Not on Gun Safety
- Physician narrative on gun control | gutsandgrowth
- NY Times: End the Gun Epidemic in America | gutsandgrowth
- A Call to Arms for Health Care Professionals
Acute Pancreatitis: Clinical Report from NASPGHAN
There are no surprises in a recent clinical report on acute pancreatitis (M Abu-El-Haija et al. JPGN 2018: 66: 159-76) from NASPGHAN.
Here are a few of the points:
- The authors recommend ultrasound for initial imaging and checking liver enzymes, GGT, calcium and triglycerides.
- For fluids, they indicate that in adults there is evidence suggesting that lactated ringer’s (LR) is likely preferable to normal saline. In children, on presentation, “if evidence of hemodynamic compromise, a bolus of 10 to 20 mL/kg” of crystalloid is recommended followed by “1.5 to 2 times maintenance IV fluids.”
- For pain management not responding to acetaminophen or NSAIDs, “IV morphine or other opioids should be used.”
- They recommend early oral/enteral nutrition (within 48 to 72 hours of presentation).
- They recommend against prophylactic antibiotics in severe acute pancreatitis.
- They recommend against probiotics, anti-proteases, and antioxidant therapy.
- For fluid collections that need drainage or necrosectomy, nonsurgical approaches are favored.
- Acute biliary pancreatitis, “Cholecystectomy safely can and should be performed before discharge in cases of mild uncomplicated acute biliary pancreatitis.”
Related blog posts:
- Acute Pancreatitis Review (2016)
- For the pediatric pancreatologists
- Pancreatitis Update (part 1) | gutsandgrowth 2017
- Pancreatitis Update (part 2) 2017
- Changing Practice Patterns with Pediatric Pancreatitis | gutsandgrowth
- Why an ERCP Study Matters to Pediatric Care | gutsandgrowth This post explains why LR may be best.
- Nutrition University / gutsandgrowth

American Ingenuity!!
Cancer due to Overweight/Obesity
The increasing risk of cancer due to overweight and obesity has been reported by the Centers for Disease Control and Prevention in recent MMWR report (CB Steele et al. MMWR 2017; 66: 1052-8) Vital Signs: Trends in Incidence of Cancers Associated with Overweight and Obesity — United States, 2005–2014
Key points:
- Overweight and obesity are associated with increased risk of at least 13 different types of cancer.
- Overweight- and obesity-related cancers accounted for 40% of all cancers diagnosed in 2014.
- The incidence of overweight- and obesity-related cancers (excluding colorectal cancer) increased significantly among persons aged 20–74 years during 2005–2014, mirroring increases of obesity observed since 1960.
- The findings emphasize the importance of intensifying nationwide efforts to prevent and treat overweight and obesity.
My take: While the medical risks related to overweight/obesity generally are attributed to worsened cardiovascular disease, this study adds information regarding the increased risks of some types of cancer as well.
Related blog posts:
- Projected Obesity Rates: Majority of Today’s Children Will Be Obese in U.S.
- Six years later-Mediterranean diet comes out on top | gutsandgrowth
- Six year outcomes with bariatric surgery | gutsandgrowth
- Healthy Obesity? | gutsandgrowth
-

Outside our house this past weekend

Colorectal Cancer: Of Mice and Microbiota
A recent study (SH Wong et al. Gastroenterol 2017; 153: 1621-33) highlights the potential role of the microbiota and colorectal cancer (CRC).
In this study, the stool from either patients with CRC or control patients was gavaged into mice twice a week for 5 weeks. One group of mice had received azoxymethane (AOM) which induces neoplasia and the other group were germ-free mice. Extensive studies involving immunohistochemistry, expresssion microarray, quantitative polymerase chain reaction, immunoblot, and flow cytometry.
Key findings:
- Conventional, AOM-treated mice who received gavage from patients with CRC had significantly higher proportions of high-grade dysplasia (P<.05) and macroscopic polyps (P<.01)
- Among the germ-free mice fed with stool from patients with CRC, there was a higher proportion of proliferating Ki-67-positve cells
- These findings correlated with more dysbiosis in the mice who received stool from patients with CRC and with upregulation of genes involved in cell proliferation, stemness, apoptosis, angiogenesis, and invasiveness
“This study provides evidence that the fecal microbiota from patients with CRC can promote tumorigenesis in germ-free mice and mice given a carcinogen.”
My take: This study shows that microbiota clearly influence the risk of CRC. I infer from this study that this could explain the potential healthy roles of diets with more fruits and vegetables, that promote healthier microbiota as well as the potential detrimental role of diets with more processed meats.
Related study: L Liu et al. Association between Inflammatory Diet Pattern and Risk of Colorectal Carcinoma Subtypes Classified by Immune Responses to Tumor Gastroenterol 2017; 153 1517-30. Using two databases from 2 prospective cohorts with followup of 124,433 participants, inflammatory diets had a higher risk of a colorectal cancer subtype.
Related blog posts:
- Better Diet, Lower Mortality
- Colon Cancer at Younger Ages
- Diet, Meat and Colrectal Cancer
- For Increased Longevity: More Greens are Good


Bright Angel Trail
Screening for Bile Acid Synthesis Disorders
A recent study (AA Al-Hussaini et al. JPGN 2017; 65: 613-20) showed that serum (total) bile acids is effective in screening for bile acid synthesis disorders. In this prospective study from Saudi Arabia, with 626 patients and 450 with infantile cholestasis, the authors identified bile acid synthetic disorder (BASD) in 2.7% of infantile cholestasis patients. Among the 15 cases, 11 were due to 3β-hydroxyl-Δ5-C27 steroid oxidoreductase dehydrogenase deficiency (HSD3B7). In these conditions, serum bile acids are low or normal (< 10 μmol/L) in the setting of cholestasis; most cholestatic conditions have elevated bile acids. In addition, all of their patients with bile acid synthetic disorders had a normal or low GGT.
Cholic acid is the “only effective therapy” for bile acid synthetic disorders. It has a high cost of “$31,000 yer year in Europe” (50 mg per day).
My take: While the authors provide a diagnostic algorithm (figure 3) for diagnosis of bile acid synthetic disorders, this will likely change with the emergence of genetic screening panel. At this time, in infants/children with cholestasis along with a normal/low GGT and normal/low serum bile acids, one should check urine for fast atom bombardment mass spectrometry.
Related blog post:

Bright Angel Trail, Grand Canyon

Iron Metabolism Improves after Anti-TNF Therapy for Crohn’s Disease
A previous study has shown that low vitamin D levels improved with anti-TNF therapy for Crohn’s disease in the absence of supplemental vitamin D. Similarly, a recent study (MA Atkinson, MB Leonare, R Herskovitz, RN Baldassano, MR Denburg. JPGN 2018; 66: 90-4) showed improvement in iron metabolism with anti-TNF therapy.
In 40 children and adolescents with Crohn’s disease, the authors measured serum hepcidin-25 and hemoglobin at baseline and then 10 weeks after anti-TNF therapy.
Key findings:
- Median hepcidin concentrations decreased (27.9–>23.2 ng/mL) and mean hemoglobin increased (10.6–>10.9).
- Disease activity and markers of inflammation also decreased.
My take: This study shows that improvement in inflammation is associated with meaningful improvement in anemia. However, most patients will need additional treatment for anemia, particularly as anemia may be related to blood loss in addition to anemia of chronic disease/inflammation.
Related blog posts:
- Microcytic Anemia Review | gutsandgrowth
- Help with hepcidin
- Be Aggressive! Treating Anemia Associated with Inflammatory Bowel Disease | gutsandgrowth
- Why Adding Vitamin D May Not Help IBD

Second-Line Treatments for Autoimmune Hepatitis
A recent retrospective study (C Efe et al. Clin Gastroenterol Hepatol 2017; 15: 1950-6) examined both mycophenolate mofetil (MMF, n=121) and tacrolimus (TAC, n=80) as second-line therapies for autoimmnue hepatitis with a median followup of 62 months. Patients were divided into two groups. The first group (n=108) had a complete response to steroids/azathioprine but had side effects. The second group (n=93) were nonresponders to steroids/azathioprine. Overall, the cohort examined patients as young as 7 years and as old as 76 years.
Key findings:
- No significant difference in complete response noted in 69.4% of MMF-treated compared with 72.4% in TAC-treated patients.
- In group 1 patients (responders to azathioprine), MMF and TAC maintained biochemical remission in 91.9% and 94.1% respectively.
- In group 2 (prior nonresponders), TAC-treated patients had a complete response rate of 56.5% compared with 34% for MMF-treated patients (P=.029).
- Liver-related deaths and transplantation occurred with similar rates: MMF 13.2% compared with TAC 10.3%. With each treatment, 10 patients withdrew from treatment due to side effects.
My take: In this study, both agents were effective in those who changed due to side effects. However, tacrolimus-treated patients had a higher response among prior nonresponders.
Related blog posts:
- Slim Pickings: Data for 2nd Line Treatment in Pediatric Autoimmune Hepatitis
- Autoimmune Liver Disease in Children with Sickle Cell Anemia
- Azathioprine metabolite measurement in Autoimmune Hepatitis
- Adult versus Pediatric Data: Autoimmune Hepatitis
- Diagnosing autoimmune hepatitis
- Withdrawing immunosuppression with autoimmune hepatitis
- Liver Problems with Inflammatory Bowel Disease
- Staying current with PSC | gutsandgrowth

Bright Angel Trail, Grand Canyon

Glecaprevir-Pibrentasvir for Hepatitis C Infections
Before discussing one of the newest therapies for Hepatitis C, I wanted to give a shout out to Barbara McElhanon who along with Joanna Lomas-Mevers provided a quick update to our group on their important research to improve the management of encopresis in children with autism spectrum disorders.

Last August, the FDA announced approval of glecaprevir-pibrentasvir as a pangenomic treatment for Hepatitis C (From blog: Eight Week Pangenomic HCV Treatment Approved).
However, it is only in this past two weeks that some of the data from two large randomized, open-label, multicenter trials have been published: Z Zeuzem et al. NEJM 2018; 378: 354-69. In total, 1208 patients were treated in the “ENDURANCE-1” and “ENDRUANCE-3” trials.
Key findings:
- For genotype 1-infected patients, glecaprevir-pibrentasvir resulted in a sustained virologic response rate (at week 12) of 99.1% in the 8-week group and 99.7% in the 12-week group.
- For genotype 3, glecaprevir-pibrentasvir resulted in a sustained virologic response rate (at week 12) of 95% with both 8-week and 12-week treatment. A comparison group of sofosbuvir-daclatasvir (12 week treatment) resulted in a sustained virologic response rate (at week 12) of 97%.
- Serious adverse events were rare. There were three patients who died during the post-treatment period: two from heroin overdoses and one from ethanol intoxication/methadone toxicity. Headache and fatigue were the most common reported adverse events.
- There were no relapses among HCV-1-infected patients who were treated for 8 weeks
In addition to these studies, “recent phase 3 trials have shown that an 8-week regimen of glecaprevir-pibrentasvir in patients without cirrhosis” yielded response of 98% for genotype 2 and 93% for genotypes 4, 5, and 6.
My take: These studies indicate that glecaprevir-pibrentasvir is an effective 8-week therapy for patients with HCV infection. Despite this terrific advance, unless we find a way to address the opioid crisis which is triggering an HCV epidemic, I am not optimistic that there will be an improvement in the number of individuals with HCV infection.
Related blog posts:
- New HCV Treatments Effective in Adolescents
- HCV Guidelines
- Hepatitis C : New and Newer Treatments
- Word of Caution with New Hepatitis C Medications | gutsandgrowth
- FDA Approval of HCV Medications for Children, 12-17 years
- Keeping Track of HCV Trials -Three More


