The investigators enrolled 53 adults with celiac disease (CD) for at least two years and followed symptoms as well as stool/urine testing for gluten immunogenic peptide (GIP). “GIP in stool can detect gluten consumption of more than 40 mg/d and the urine tests are positive from 40 and 500 mg/d of gluten.”
Key findings:
Over the 4-week study period, weekend samples (urine) identified 70% of patients excreted GIP at least once, compared with 62% during weekdays (stool).
Patients had a median of 3 exposures during the 4 weeks.
Also, the authors noted increases in GIP excretion towards the end of the study. “This suggests a potential Hawthorne effect that could be explained by a decrease in hypervigilance that often is seen in a context of research studies.”
The authors note that GIP “excretions of greater than 2 mcg/g in stool or greater than 12 ng/mL in urine can induce mucosal damage in almost 100% of patients.”
My take: This study adds to the body of literature emphasizing the high rate of inadvertent gluten exposure.
Diverticulitis is rarely seen in the pediatric age group. Over the course of nearly 30 years, I have encountered two cases; though, many of my partners with longer clinical experience have seen none.
Best Practice Advice 1: Computed tomography should be considered to confirm the diagnosis of diverticulitis in patients without a prior imaging-confirmed diagnosis and to evaluate for potential complications in patients with severe presentations. Imaging should also be considered in those who fail to improve with therapy, are immunocompromised, or who have multiple recurrences and are contemplating prophylactic surgery in order to confirm the diagnosis and location(s) of disease.
Best Practice Advice 3: After an acute episode of diverticulitis, colonoscopy should be delayed by 6–8 weeks or until complete resolution of the acute symptoms, whichever is longer. Colonoscopy should be considered sooner if alarm symptoms are present.
Best Practice Advice 5: A clear liquid diet is advised during the acute phase of uncomplicated diverticulitis. Diet should advance as symptoms improve.
Best Practice Advice 7: Antibiotic treatment is advised in patients with uncomplicated diverticulitis who have comorbidities or are frail, who present with refractory symptoms or vomiting, or who have a C-reactive protein >140 mg/L or baseline white blood cell count > 15 × 109 cells/L. Antibiotic treatment is advised in patients with complicated diverticulitis or uncomplicated diverticulitis with a fluid collection or longer segment of inflammation on CT scan.
Best Practice Advice 9: To reduce the risk of recurrence, patients with a history of diverticulitis should consume a high-quality diet, achieve or maintain a normal body mass index, be routinely physically active, and not smoke. Additionally, patients with a history of diverticulitis should avoid regular use (2 or more times per week) of nonsteroidal anti-inflammatory drugs except aspirin prescribed for secondary prevention of cardiovascular disease.
Seven studies reported the prevalence of IDTI (Incidentally-diagnosed terminal ileitis) in 44,398 persons undergoing non-diagnostic colonoscopy
The pooled prevalence rate of IDTI was 1.6%
Progression to overt CD was rare over 1-7 years of followup
My take: As noted below by Dr. Rubin, in those with normal labs who are asymptomatic, most incidental ileitis is not progressive and should be monitored.
This slide from @RealCecum Twitter Feed and @IBDMD Twitter Feed
A global epidemiological study of functional GI disorders • 73,076 adults surveyed (33 countries, 6 continents) • Data collection: By Internet (24 countries), by household interview (7 countries), or both methods (China and Turkey, green).
Key findings:
Diagnostic criteria were met for at least 1 FGID by 40.3% persons who completed the Internet surveys and 20.7% of persons who completed the household surveys
FGIDs were associated with lower quality of life and more frequent doctor visits
My take: In industrialized countries, about 40% have functional GI disorders.
From 2007–2015, approximately 36.9 million (95% CI, 31.4–42.4) weighted visits in patients of non-federally employed physicians for chronic symptomatic FBDs were sampled. There was an annual weighted average of 2.7 million (95% CI, 2.3–3.2) visits for symptomatic irritable bowel syndrome/chronic abdominal pain, 1.0 million (95% CI, 0.8–1.2) visits for chronic constipation, and 0.7 million (95% CI, 0.5–0.8) visits for chronic diarrhea. Pharmacologic therapies were prescribed in 49.7% (95% CI, 44.7–54.8) of visits compared to nonpharmacologic interventions in 19.8% (95% CI, 16.0–24.2) of visits (P < .001). Combination treatment strategies were more likely to be implemented by primary care physicians and in patients with depression or obesity. The direct annual cost of ambulatory clinic visits alone for chronic symptomatic FBDs is approximately US$358 million
The retrospective study by Simonov et al used data from the Women’s Veteran’s Cohort Study (1999-2017) with 465,891 patients. Key findings:
Overall, 2.4% of the cohort developed kidney stones. PPI use was associated with kidney stones in the unadjusted analysis, hazard ratio [HR], 1.74 (95% CI, 1.67–1.82), and persisted in the adjusted analysis with HR, 1.46 (CI, 1.38–1.55). The association was maintained in a propensity score-matched subset of PPI users and nonusers (adjusted HR, 1.25; CI 1.19–1.33).
H2RAs were also associated with increased risk with adjusted HR, 1.47
While this study is interesting, the editorial provides a great deal of insight into how this study and many others can be misleading. Key points:
“It seems that every few months a new issue arises, with the list of problems that PPIs might cause becoming ever longer, including pneumonia, fracture, heart disease, Clostridium difficile–associated diarrhea, dementia, chronic kidney disease, low B12 levels, gastric cancer, and even all-cause mortality.”
If the findings in the study are correct, with the unadjusted HR, “this translates to a number needed to harm (NNH) of 365 patients who need to take PPIs for 1 year to observe 1 extra episode of kidney stones…if the adjusted HR is used …the NNH was 1550.”
Limitations:
Confounding variables are hard to eliminate in an observational study. “Studies usually show that patients who are prescribed PPIs are, on average, sicker than those who are not taking these drugs.”
In the only large randomized controlled study (>17,000 patients over 3 years) of PPIs, there was no difference in pneumonia, Clostridium difficile infection, fracture, gastric atrophy, chronic kidney disease, dementia, cardiovascular disease, cancer, hospitalizations, and all-cause mortality in the PPI compared with the placebo arms.”Enteric infections, which were slightly more common in patients randomized to PPIs, but even there the NNH was more than 900 per year.”
Biases undermine the interpretation of observational studies. One example for PPIs is its association with pneumonias in prior observational studies.
“The effect was strongest within the first week of prescription when the odds ratio was approximately 4, although this was reduced to approximately 1.5 after 1 month. This marked reduction in risk over a relatively short period of time is not biologically plausible and a more likely explanation is that the association is the result of protopathic bias. Patients presenting to the clinician with a cough may be diagnosed with silent reflux and given a PPI. A few days later other symptoms develop, and pneumonia is made as the final diagnosis. This will not be apparent when simply interrogating a database where the researcher will observe that a PPI was prescribed before the onset of pneumonia and will imply the association is causal when this is not the case.”
This same type of bias could be present with the association between PPI and kidney stones.
“Patients may present with abdominal pain and be given a PPI as a therapeutic trial, assuming the pain may be acid-related when subsequently it is found that the pain relates to kidney stones. Simonov et al reported that 3% were prescribed PPIs within 1 month of the diagnosis of kidney stones, but did not provide the analysis that would allow us to interpret whether protopathic bias may play a role in the associations observed”
My take: It is unlikely that PPIs cause kidney stones; however, if this is a risk factor, it is very rare. Understanding how PPIs have been incorrectly linked to a multitude of problems is a valuable lesson for any practitioner and emphasizes the need for randomized controlled studies to determine medication safety.
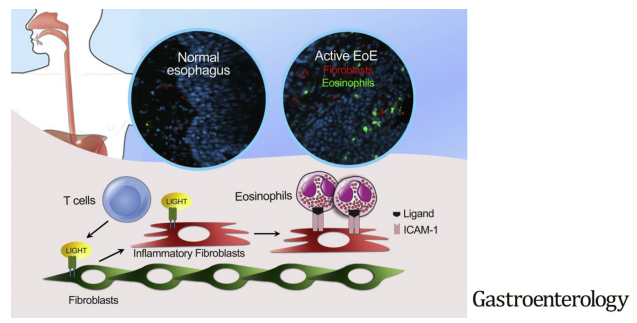
The authors investigated the effects of tumor necrosis factor superfamily member 14 (TNFSF14, also called LIGHT) on fibroblasts in EoE.
Key findings:
LIGHT was up-regulated in the esophageal tissues from patients with EoE, compared with control individuals
Stimulation of esophageal fibroblasts with LIGHT induced inflammatory gene transcription
My take: The authors show that patients with EoE had proinflammatory fibroblasts in the epithelium. Further, they show that eosinophil-fibroblast interaction was dependent on intact LIGHT signaling.
“The committee strongly recommends that adults with moderate‐to‐severe CVS receive a tricyclic antidepressant (TCA) such as amitriptyline, as a first‐line prophylactic medication. “
Topiramate, Aprepitant, “Zonisamide or levetiracetam and mitochondrial supplements (Coenzyme Q10, L‐carnitine, and riboflavin) are conditionally recommended as alternate prophylactic medications, either alone or concurrently with other prophylactic medications.”
“For acute attacks, the committee conditionally recommends using serotonin antagonists such as ondansetron, and/or triptans such as sumatriptan or newer agents such as aprepitant (NK1 receptor antagonist) to abort symptoms.”
Evidence, dosing regimens, and algorithms are detailed in article
Sample ED CVS Protocol (for Adults):
____[name]____________ has an established diagnosis of Cyclic Vomiting Syndrome
Operational definition
* A recurring pattern of discrete episodes of severe vomiting, accompanied by profound nausea and/or severe abdominal pain * Patient returns to usual health status between episodes (may have inter‐episodic nausea and or dyspepsia) * In some patients, CVS episodes resemble a migraine attack * Patients may be restless, anxious, and distressed * Patients are not customarily dehydrated until late in the episode
Therapeutic goal
Rapid recognition and intervention may decrease severity of the attack and promote prompt resolution of symptoms
ED management
1. Clinical assessment: Pulse/Temp/BP/Weight, consciousness, and hydration 2. Laboratories/evaluation: CBC, urea, creatinine, LFT’s, lipase, glucose, and electrolytes EKG Urine analysis Diagnostic imaging at discretion of attending physician
Treatment
1. Intravenous fluids a. IV saline bolus if clinically dehydrated b. IV D5NS at 100%‐150% maintenance (suggested rate is 200 cc/h for a 70 kg adult.) 2. For vomiting and nausea a. IV ondansetron 8 mg IV × 1—may repeat q 4‐6 h if ondansetron is ineffective b. Consider diphenhydramine 50 mg IV and metoclopramide 10 mg IV c. Consider IV fosaprepitant 150 mg if available 3. For sedation a. IV lorazepam 1‐2 mg and b. IV diphenhydramine 50 mg for additional sedation 4. For migraine‐like presentation a. Sumatriptan nasal 20 mg (head forward technique) or b. Sumatriptan subcutaneous injection 6 mg/0.5 mL 5. For pain a. IV ketorolac 30 mg if > 60 minutes from onset; may repeat 15 mg q 6 h x 2 (maximum 60 mg/d) b. Opioids may be considered as part of an ongoing treatment plan in refractory patientsa
Reassess
1. Treatment failure—intensify treatment as indicated above or admit patient 2. Positive treatment response—discharge a. Continue ondansetron (soluble tablets) q 6‐8 h × 24‐48 h if initially effective b. Continue lorazepam × 24‐48 h if initially effective c. Continue NSAIDs for pain as needed
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition
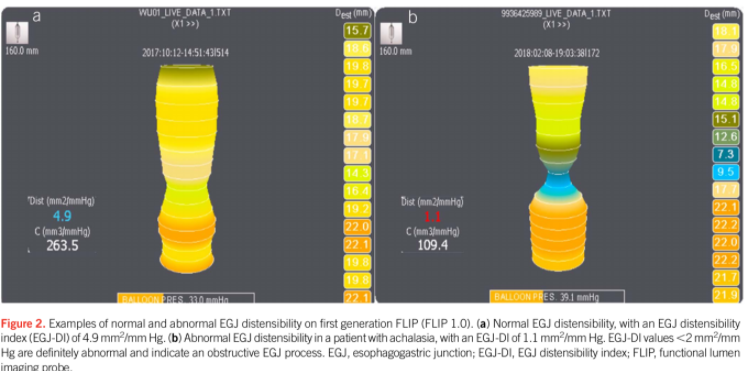
A recent review article (E Sararino et al. Am J Gastroenterol 2020; 115: 1786-06. Use of the Functional Lumen Imaging Probe in Clinical Esophagology) is a terrific article for understanding Functional Lumen Imaging Probe (FLIP) techonology and uses. Thanks to Ben Gold for this reference.
The FLIP “measures luminal cross sectional area (CSA) and pressure in the esophagus using impedance planimetry and serves as an adjunct to existing esophageal investigative tests. A distensible balloon encasing a catheter with multiple pairs of impedance electrodes is used, and the balloon is distended with fluid of known conductivity and volume.”
FLIP can be done at time of endoscopy.
Distensibility index (DI). This is the ratio of EGJ cross sectional area to intraballoon pressure is generally considered the most useful FLIP metric. Normal DI values in adults range from 3.1 to 9.0 m3/mm Hg. Lower values indicated reduced EGJ opening.
FLIP can complement the diagnosis of achalasia when manometry and barium studies are inconclusive or negative in patients with typical symptoms.
FLIP can be used to assess fibrostenotic remodeling of the esophagus in eosinophilic esophagitis.
Lumen diameter measured using FLIP in complex strictures can potentially guide management.
This review has several helpful figures to illustrate the type of visual data available. It also provides a standard protocol for using FLIP. The current limitations for FLIP include the lack of real-time software analysis of the data which hinders reporting, and limited data supporting use.
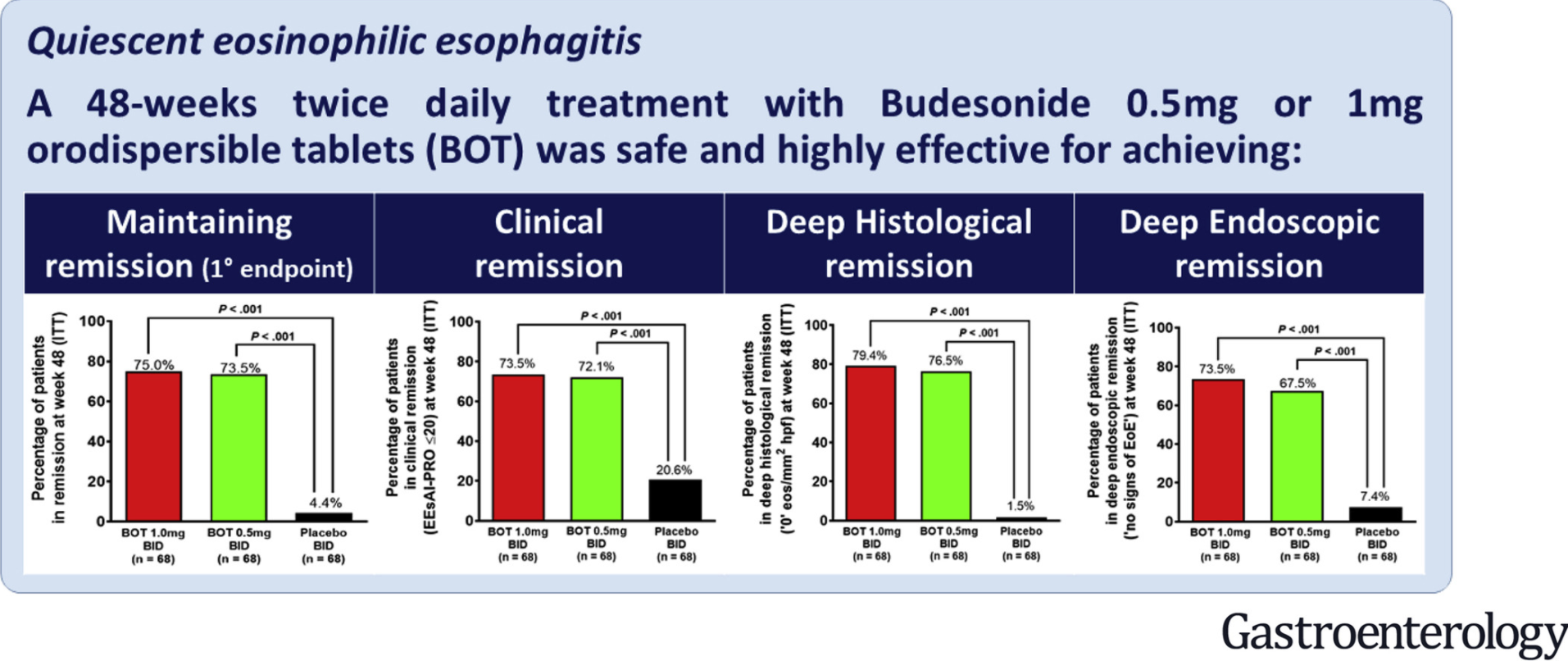
Methods: Two hundred and four adults with EoE in clinical and histologic remission, from 29 European study sites, were randomly assigned to groups given budesonide orodispersible tablet (BOT) 0.5 mg twice daily (n = 68), BOT 1.0 mg twice daily (n = 68), or placebo twice daily (n = 68) for up to 48 weeks
Key Findings:
At end of treatment, 73.5% of patients receiving BOT 0.5 mg twice daily and 75% receiving BOT 1.0 mg twice daily were in persistent remission compared with 4.4% of patients in the placebo group (P < .001 for both comparisons of BOT with placebo)
Four patients receiving BOT developed asymptomatic, low serum levels of cortisol. Clinically manifested candidiasis was suspected in 16.2% of patients in the BOT 0.5 mg group and in 11.8% of patients in the BOT 1.0 mg group; all infections resolved with treatment
In the discussion, the authors state that “we recommend monitoring symptoms and signs of adrenal insufficiency when administrating topical-acting corticosteroids over prolonged time periods, in particular in children and when using higher dosages.”
My take (from discussion): “EoE requires a proper long-term anti-inflammatory therapy because, without active treatment, the vast majority of patients experience a relapse within the first 100 days after cessation of the medication.”