G Lassailly et al. Gastroenterol 2020; 159: 1290-1301. Bariatric Surgery Provides Long-term Resolution of Nonalcoholic Steatohepatitis and Regression of Fibrosis
This was a prospective study of 180 severely obese patients with biopsy-proven NASH.
Key findings:
- NASH: At 5 years after bariatric surgery, NASH was resolved, without worsening fibrosis, in samples from 84% of patients (n = 64; 95% confidence interval, 73.1%-92.2%).
- Fibrosis: Fibrosis decreased, compared with baseline, in samples from 70.2% of patients (95% CI, 56.6%-81.6%). Fibrosis disappeared from samples from 56% of all patients (95% CI, 42.4%-69.3%) and from samples from 45.5% of patients with baseline bridging fibrosis.
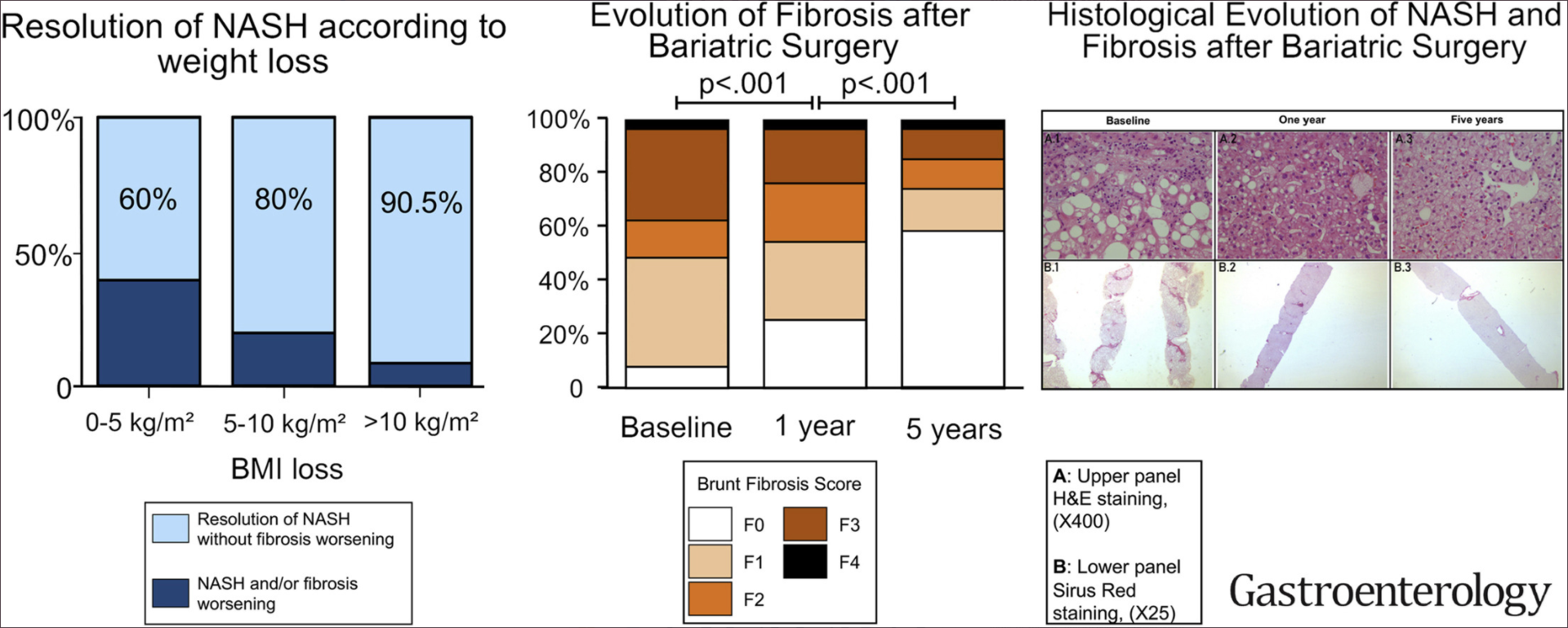
My take: This study showed that patients with NASH who underwent bariatric surgery had resolution of NASH in liver samples from 84% of patients 5 years later. The reduction of fibrosis was progressive, beginning during the first year and continuing through 5 years.
. Related blog posts:
- Bariatric Surgery and Reversal of NASH in Children
- Adolescent Bariatric Outcomes
- Is a Three Year-Old Too Young for Bariatric Surgery …
- Reaching Consensus on Bariatric Intervention… | gutsandgrowth
- Trends in Adolescent Bariatric Surgery | gutsandgrowth
- Six year outcomes with bariatric surgery | gutsandgrowth
- Staggering cost of obesity | gutsandgrowth
- Two new drugs for obesity | gutsandgrowth
- Treating diabetes with surgery | gutsandgrowth
- Six years later-Mediterranean diet comes out on top | gutsandgrowth