While famotidine (the new ingredient in Zantac 360) acts similar to ranitidine (the old ingredient), there is no longer N-nitrosodimethylamine (NDMA) detectable which was a concern as a potential cancer risk. It comes in two different strengths (10 mg and 20 mg).
My take: In my view, it is a bad decision to allow Zantac to be relaunched with this new ingredient; this is like allowing some hot dogs to be sold as hamburgers.
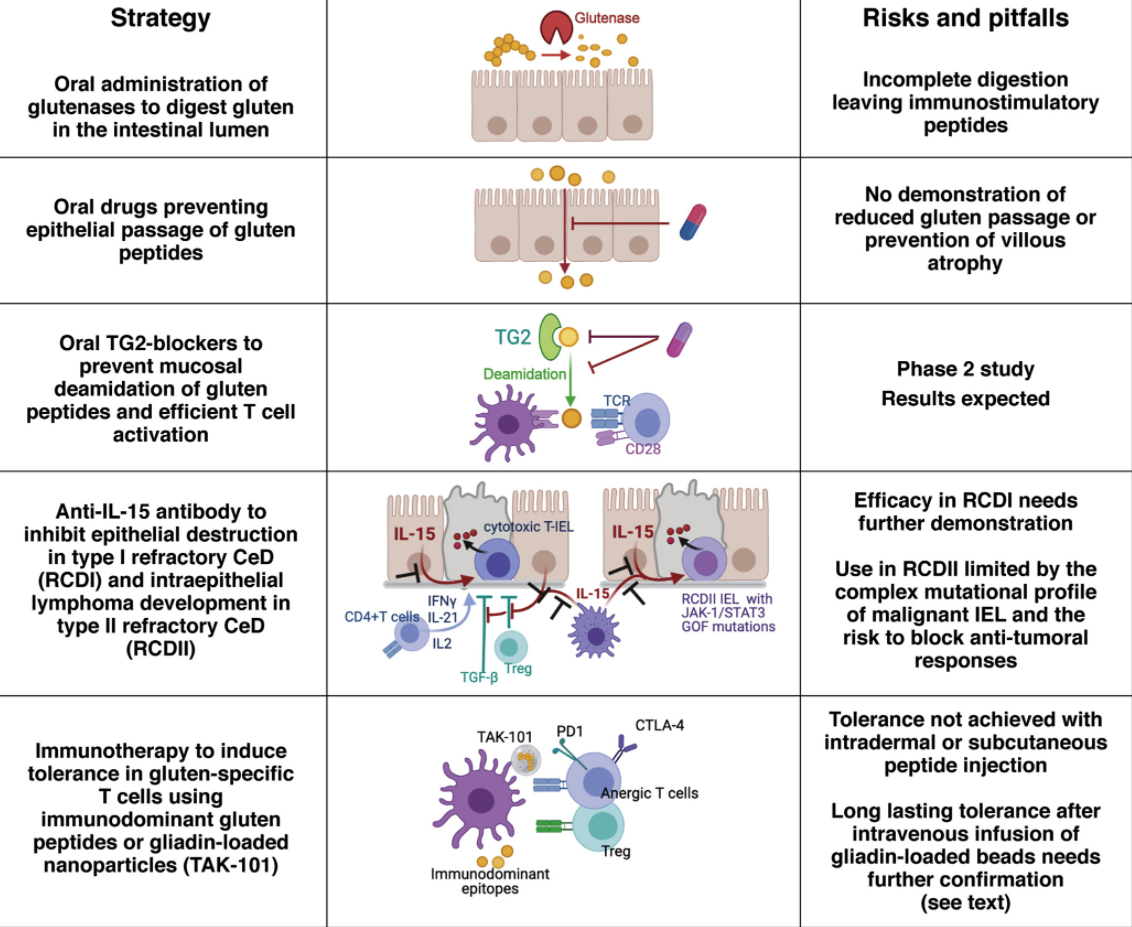
In the first study, Kelly et al used TAK-101 nanoparticles in Phase 1 and Phase 2a trials. In the Phase 2a trial with 33 patients, TAK-101 induced an 88% reduction in change from baseline in interferon-γ spot-forming units vs placebo (2.01 vs 17.58, P = .006). Vh:Cd deteriorated in the placebo group (−0.63, P = .002), but not in the TAK-101 group (−0.18, P = .110) Overall, TAK-101 was well tolerated and prevented gluten-induced immune activation.
Graphical abstract from CP Kelly et al. Gastroenterol 2021; 161: 66-80.
In the second study, Pultz et al developed TAK-062 which is a novel, computationally designed endopeptidase to break down gluten under simulated gastric conditions in vitro and in healthy participants in the phase I study. Residual gluten (collected through gastric aspiration in the phase I study) was quantified using R5 and G12 monoclonal antibody enzyme-linked immunosorbent assays. Key finding: In vitro, TAK-062 degraded more than 99% of gluten (3 g and 9 g) within 10 minutes. In the phase I study, administration of TAK-062 was well tolerated and resulted in a median gluten degradation ranging from 97% to more than 99% in complex meals containing 1–6 g gluten at 20–65 minutes postdose.
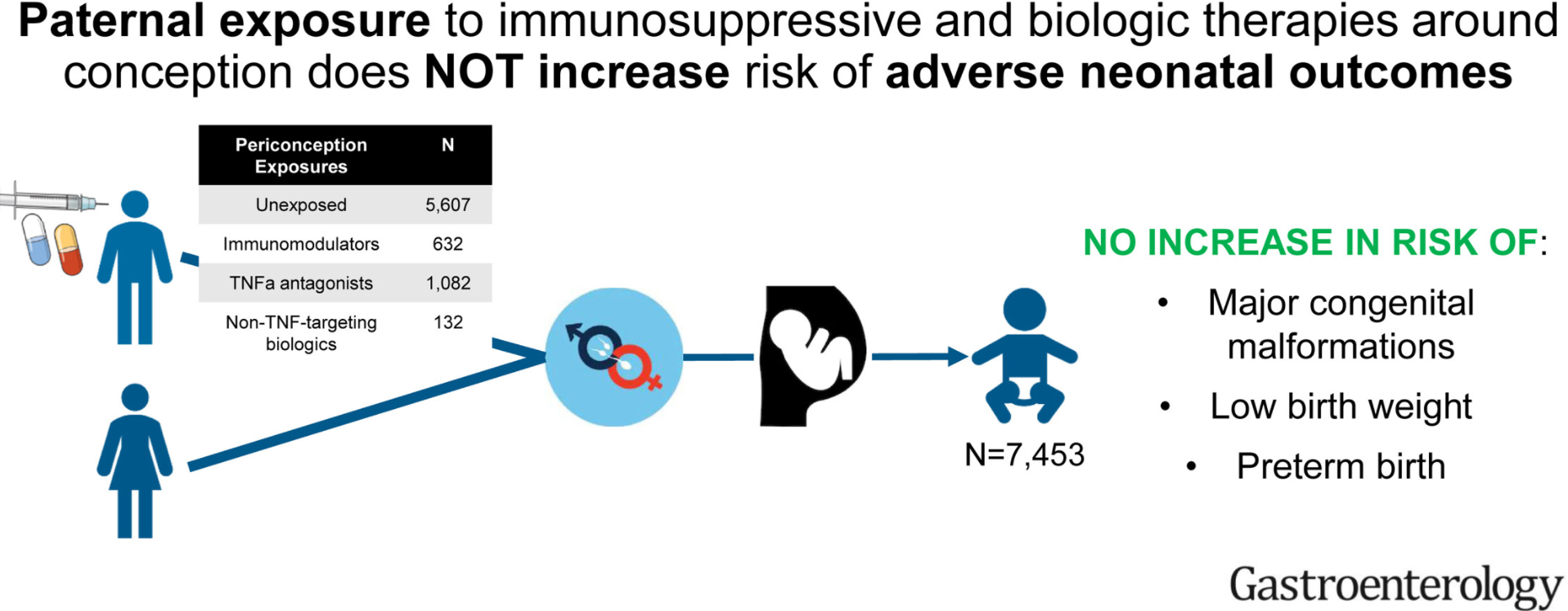
Methods: The investigators used a deidentified administrative claims database (OptumLabs Data Warehouse) with a total of 7453 expectant fathers with immune-mediated diseases.
Key findings:
As compared to unexposed fathers (3.4% prevalence of major congenital malformations), exposure to immunosuppressives/biologics were not associated with increased risk of major congenital malformations: thiopurines (relative risk [RR], 1.12; 95% confidence interval [CI], 0.66–1.76), methotrexate (RR, 0.67; 95% CI, 0.21–1.55), TNF-α antagonists (RR, 1.14; 95% CI, 0.81-1.57), and non–TNF-targeting biologic agents (RR, 1.75; 95% CI, 0.80–3.24).
No association was observed between paternal medication exposure and risk of preterm birth or low birth weight.
“Regarding major congenital malformations, we believe that the results should be interpreted with caution. The numbers of these outcomes are relatively low and the statistical precision of the risk estimates should be taken into consideration.”
My take: Overall, this study is reassuring. Though it is difficult to prove these medications do not have impacts on newborns, if these effects were frequent, it would likely be evident in this type of study.
Of the 353 patients, there were immune-tolerant 112 (34%), HBeAg-positive immune-active 47 (14%), and inactive carrier 82 (25%). The remaining 88 patients (27%) did not fit into a particular category with 26 of 88 patients meeting the criteria for inactive carrier except for mildly elevated alanine aminotransferase
Among 179 patients followed for ≥5 years, the spontaneous seroconversion rate was 38% (from HBeAg-positive to HBeAg-negative along with anti-HBeAb positivity)
In their discussion, the authors make two key points:
“No substantial benefit from anti-viral therapy” has been evident in children in the immuno-tolerant phase (MM Jonas et al. Hepatology 2016; 63: 307-318.)
The updated AASLD guidelines “strongly recommend anti-viral therapy for HBeAg-positive pregnant women with a serum HBV DNA >200,000 IU/mL”
As noted above, antiviral therapy has not been shown to be effective in children who are in the immuno-tolerant phase; however, the authors of this study explored whether combination therapy could be effective in a randomized, controlled, multicenter study (n=59).
Key finding: At 24 weeks post-treatment, 1 of 26 patients in the antiviral treatment group experienced HBsAg loss (vs none of 33 patients in the control group)
My take: These studies reinforce the notion that children in the immuno-tolerant phase of HBV infection do not benefit from antiviral therapy. Prevention of infection is the most promising strategy.
So sad to hear that Jim Heubi has passed away. Jim Heubi was the person I interviewed with when I was considering where to do my pediatric residency and he helped convince me to come to Cincinnati. During my fellowship, I came to admire how he was so good at everything though it was always unassuming. He was such a kind person in addition to being a mentor and role model.
PPI response: 56% for erosive reflux disease, 37% for NERD, and 25% for functional heartburn (FH) per Figure 3 (*”FH might be a placebo effect owing to short follow-up evaluation”
Determination of abnormal acid exposure time (AET >6% in adults) is key in distinguishing NERD from FH which in turn helps with selection of treatment. NERD is notable for AET >6% in adults. Many patients with NERD may also have esophageal hypersensitivity
Table 2 reviews efficacy of neuromodulators for functional esophageal disorders; these include TCAs, SNRIs, SSRIs, and other agents (eg. gabapentin)
Heartburn etiologies in adults, per Yamasak T et al. J Neurogastroenterol Motil 2017; 23: 495-503.
Background: “A high-fat diet has been associated with an increased risk of ulcerative colitis (UC). We studied the effects of a low-fat, high-fiber diet (LFD) vs an improved standard American diet (iSAD, included higher quantities of fruits, vegetables, and fiber than a typical SAD)”
Key findings:
Compared with baseline, the iSAD and LFD each increased quality of life, based on the short IBD questionnaire and Short-Form 36 health survey scores (baseline short IBD questionnaire score, 4.98; iSAD, 5.55; LFD, 5.77; baseline vs iSAD, P = .02; baseline vs LFD, P = .001)
Fecal levels of acetate (an anti-inflammatory metabolite) increased from a relative abundance of 40.37 at baseline to 42.52 on the iSAD and 53.98 on the LFD (baseline vs LFD, P = .05; iSAD vs LFD, P = .09)
Overall, in this small cross-over study (cross-over study) of 17 patients with UC in remission, a catered LFD or a iSAD were each well tolerated and increased quality of life. However, the LFD decreased markers of inflammation and reduced intestinal dysbiosis in fecal samples
My take: While dietary intervention is recognized as a more effective intervention in Crohn’s disease, this study shows that a low-fat high fiber diet for patients with ulcerative colitis may be beneficial.
The four trials (n=255) directly compared the use of normal saline and heparin; the studies all used different protocols for the intervention and control arms, however, and all used different concentrations of heparin.
The estimated RR for CVC occlusion per 1000 catheter days between the normal saline and heparin groups was 0.75 (95% CI 0.10 to 5.51; 2 studies, 229 participants; very low certainty evidence).
The estimated RR for CVC‐associated blood stream infection was 1.48 (95% CI 0.24 to 9.37; 2 studies, 231 participants; low‐certainty evidence).
The duration of catheter placement was reported to be similar for the two study arms in one study (203 participants; moderate‐certainty evidence), and not reported in the remaining studies.
This is in agreement with another updated Cochrane review assessing the effectiveness and safety of intermittent locking of CVCs with heparin vs. normal saline to prevent occlusion in adults (11 studies; N=2,392). The pooled analysis did show fewer occlusions with heparin than with normal saline (RR 0.70, 95% CI 0.51 to 0.95; P = 0.02; 1672 participants; 1025 catheters from 10 studies; I² = 14%), but it is based on a very low-quality of evidence given the differences in methodology, unclear allocation concealment, imprecision, and suspicion of publication bias. (López-Briz E, Ruiz Garcia V, Cabello JB, et al. Heparin versus 0.9% sodium chloride locking for prevention of occlusion in central venous catheters in adults. Cochrane Database Syst Rev. 2018;7(7):CD008462. doi: 10.1002/14651858.CD008462.pub3)
My take: This review found there was not enough evidence to determine which solution, saline or heparin, is more effective for reducing complications.
Adalimumab trough levels (TLs) at both weeks 4 and 8 were significantly higher in remitters vs nonremitters at week 24 (P < 0.001 and P = 0.002, respectively)
The best ADA TL cutoffs at weeks 4 and 8 for predicting clinical/biomarker remission at week 24 were 22.5 µg/mL (80% sensitivity, 90% specificity) and 12.5 µg/mL (94% sensitivity, 60% specificity) respectively
My take (borrowed from authors): Greater early ADA exposure is associated with superior clinical/biomarker outcomes at week 24. ADA pediatric dosing is looking a lot like infliximab dosing in which nearly 75% would be underdosed if using on-label dosing.