Drug persistence was high (94.9%) after 54 weeks in cohort of 158 patients
Double switching from the originator Infliximab to CT-P13 and then to SB2 was associated with continued effectiveness; this study did not identify issues related to immunogenicity or safety of anti-TNF therapy after 54 weeks of follow-up.
My take: There is very limited data on repeated infliximab product changes; this small study did not identify any problems. Due to mandates from insurance, more frequent switching is likely to be more widespread and more definitive outcome data will emerge.
In this retrospective review with 89 patients who developed antidrug antibodies (ADAs), the authors identified 30 who started an immunomodulator (IM) within 3 months of developing an ADA and compared with 59 who did not start an IM. The main IM used was methotrexate (n= 28, 93%)
Key findings:
61 of the 89 patients (69%) had quiescent disease based on physician global assessment at their previous clinic visit
The initial anti-TNF was stopped shortly after ADA detection in 36% of the No-IM patients vs none of the IM patients. Thus, anti-TNF agents durability was prolonged in the IM group.
Dose intensification was also undertaken at the time of ADA detection: 25 (83%) of IM group and 28 (48%) of non-IM group.
At 12 months, steroid-free clinical and biochemical remission on the same anti-TNF occurred in 53.9% of the IM group vs 26.8% in the No-IM group (P = 0.025).
Drug levels rose higher (P = 0.003) and ADA levels fell farther (P = 0.037) in the IM group than in the No-IM group
Lower ADAs often improved without IM: An ADA level <329 ng/mL had a 76.2% sensitivity and an 83.3% specificity for ADA reversal without IM.
My take: If a patient develops a significantly elevated anti-drug antibody, addition of methotrexate/immunomodulator along with dose intensification increases the likelihood that the anti-TNF agent will continue to be effective.
Background: MALS is generally considered after other more common conditions. Typical symptoms include abdominal pain after eating or exercise and often weight loss due to fear of eating. The pain is often positional and may improve with leaning forward. The diagnostic finding of celiac artery compression may be identified in many healthy individuals (10-24% of population); thus, only severe compression, which is seen in a small number, can result in symptomatic MALS.
In this study, the key findings:
31 patients with both MALS and OI were identified from 2014-2019. Median f/u after surgery was 22 months.
Based on questionnaires, gastrointestinal symptoms of abdominal pain, nausea, and vomiting improved in 63% (P = .007), 53% (P = .040), and 62% (P = .014) of patients, respectively.
Based on questionnaires, cardiovascular symptoms of dizziness, syncope, chest pain, and palpitations improved in 45% (P = not significant), 50% (P = not significant), 54% (P = .043), and 54% (P = .037) of patients, respectively.
Importantly, the authors could not demonstrate a “statistical relationship between a postoperative decrease in celiac artery Doppler velocity and improvement in clinical symptoms.”
In an effort to gauge for a potential post-surgical placebo effect, the authors determined the degree of improvement in musculoskeletal symptoms. There was a 24% improvement which was much less than the improvement in GI symptoms.
One useful feature of this article is that the authors explicitly state how they arrive at the diagnosis of MALS. They start with an abdominal ultrasound with doppler. Criteria for suspected MALS include supine celiac artery peak systolic velocity of >300 cm/s, celiac artery/aoritic peak systolic ratio of >3:1, neutral position celiac artery peak systolic velocity of >200 cm/s, and a change in the celiac artery deflection angle of >50 degrees between inspiration and expiration. If ultrasound is abnormal, the authors obtained an enhanced CT to image inspiratory and expiratory changes in the celiac artery deflection angle, the area of stenosis, poststenotic dilation, and the collateral blood vessels. If there are discrepancies between U/S and CT, a celiac arterial angiogram is obtained.
The authors conclude that there “were minimal improvements in neurologic or psychological symptoms after MALS surgery, despite their common occurrence among patients with POTS.”
My take: This study, in agreement with others, showed that about 60% had improvement in GI symptoms including pain, nausea and vomiting. In those with OI, most continued with impaired health. Overall, MALS as a clinical entity remains a ‘needle in a haystack.’
Background: “Children with these levels of malnutrition have defects in the development of their gut microbiota, which leaves them with microbial communities that appear to be younger than those of their healthy counterparts”
Methods: After completing studies in mice and piglets, the authors developed several microbiota-directed complementary food (MDCF) prototypes. They compared three of these formulations with an existing ready-to-use supplementary food (RUSF) in a 1-month-long, randomized, controlled trial involving children between the ages of 12 months and 18 months with moderate acute malnutrition who were living in an urban slum known as Mirpur, located in Dhaka, Bangladesh. A total of 118 children (59 in each study group) completed the intervention.
Key findings:
The rates of change in the weight-for-length and weight-for-age z scores are consistent with a benefit of MDCF-2 on growth over the course of the study, including the 1-month follow-up.
Receipt of MDCF-2 was linked to the magnitude of change in levels of 70 plasma proteins and of 21 associated bacterial taxa that were positively correlated with the weight-for-length z score (P<0.001 for comparisons of both protein and bacterial taxa). These proteins included mediators of bone growth and neurodevelopment.
The mean weekly change in the weight-for-length z score was 0.021 (95% confidence interval [CI], 0.014 to 0.029) in the MDCF-2 group and 0.010 (95% CI, 0.003 to 0.017) in the RUSF group, for a between-group difference of 0.011 (95% CI, 0.001 to 0.021).
The mean weekly change in the weight-for-age z score was 0.017 (95% CI, 0.012 to 0.022) in the MDCF-2 group and 0.010 (95% CI, 0.004 to 0.015) in the RUSF group, for a between-group difference of 0.008 (95% CI, 0.001 to 0.015).
My take: This study supports the notion that alterations in the microbiome need to be restored for healthy growth and development. Further studies are needed regarding the durability of the improvements induced by the MDCF and long-term outcomes.
In 2011, leaders of regional endoscopy units in Northern Denmark reached a consensus on a protocol to take eight biopsy samples in dysphagia patients (four biopsies from 4 cm and 14 cm above the esophagogastric junction-“4-14-4 rule”) regardless of the macroscopic appearance.
Key finding: Thenumber of patients with esophageal eosinophilia detected per year increased 50-foldafter the protocol was implemented in 2011 (median of 1 [interquartile range 0-3] vs. 52 [47-56]; P < 0.001), and the number of biopsy samples per patient doubled (median 4 [4-5] vs. 8 [6-9]; P < 0.04). In total, there were 309 with esophageal eosinophilia identified from 2007-2017.
My take: This study provides more data that more biopsies help identify more cases of eosinophilic esophagitis.
Related blog posts:
Best Approach for Identifying Eosinophilic Esophagitis Prior studies have shown higher yield when taking 5 or 6 biopsies rather than fewer biopsies; thus, the location of biopsies may not be as important as the number of specimens. Also, prior studies have shown that having another pathologist review the slides can increase the yield by ~20%; this indicates that careful review of specimens by itself is helpful. Perhaps, more specimen containers will increase the time that a pathologist reviews the biopsies.
A recent large retrospective pediatric study provides further evidence that therapeutic drug monitoring (TDM) in inflammatory bowel disease (IBD) results in better clinical outcomes. One of my partners, Chelly Dykes, is a coauthor and leads our ImproveCareNow team.
This single center implemented a practice wide TDM approach in 2014. This study compared a historical pre-TDM group (n=108) to the TDM group (n=206). The primary outcome was sustained clinical remission (SCR22-52), defined as physician global assessment (PGA) of inactive from 22 to 52 weeks and off corticosteroids at 52 weeks. Key findings:
The SCR22-52 was achieved in 42% of pre-TDM and 59% of TDM patients (risk difference, 17.6%; 95% CI, 5.4–29%; P = 0.004)
The TDM group had an increased adjusted odds of achieving SCR22-52 (odds ratio, 2.03; 95% CI, 1.27–3.26; P = 0.003)
The adjusted risk of developing high titer antidrug antibodies (ADAs) was lower in the post-TDM group (hazard ratio, 0.18; 95% CI, 0.09–0.35; P < 0.001)
The SCBR22-52 (which was defined by normal CRP along with SCR22-52) was 24.7% in pre-TDM and 42.7% in the TDM group
The authors did not identify a significantly higher rate of anti-TNF cessation in either group
Only 12% of patients in their practice were receiving combination therapy
In the discussion, the authors review three pivotal studies which also support proactive TDM: TAXIT, TAILORIX, and PAILOT.
My take: While this was an observational study with historical controls, the findings are convincing that proactive TDM is helpful, particularly in patients who are not receiving combination therapy.
AGA 2017 Guidelines on Therapeutic Monitoriing Proactive drug monitoring: “careful and selective use of proactive TDM could be beneficial, but current evidence for its routine use is limited and its overall benefits remain uncertain”
Key finding: 606 patients were randomized to treatment (placebo: n=202; lubiprostone: n=404). No statistically significant difference in overall SBM (spontaneous bowel movement) response rate was observed between the lubiprostone and placebo groups (18.5% vs 14.4%; P=.2245).
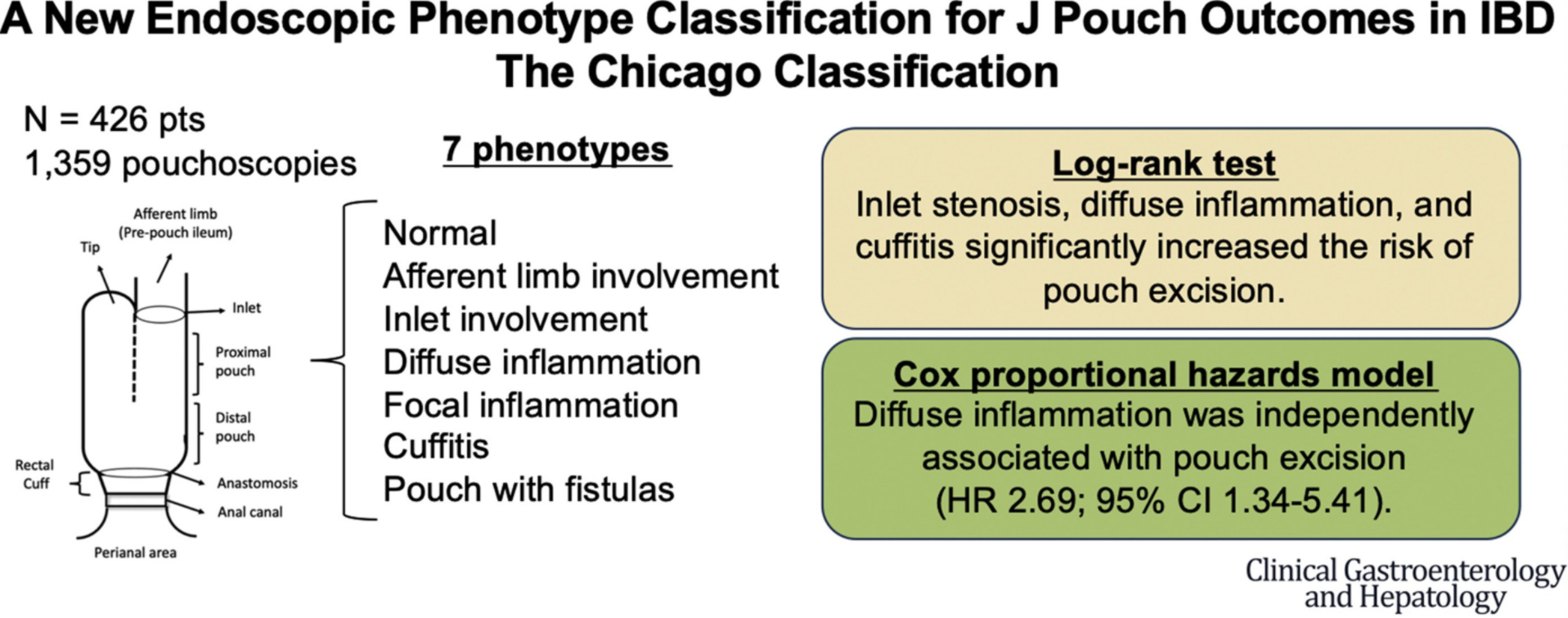
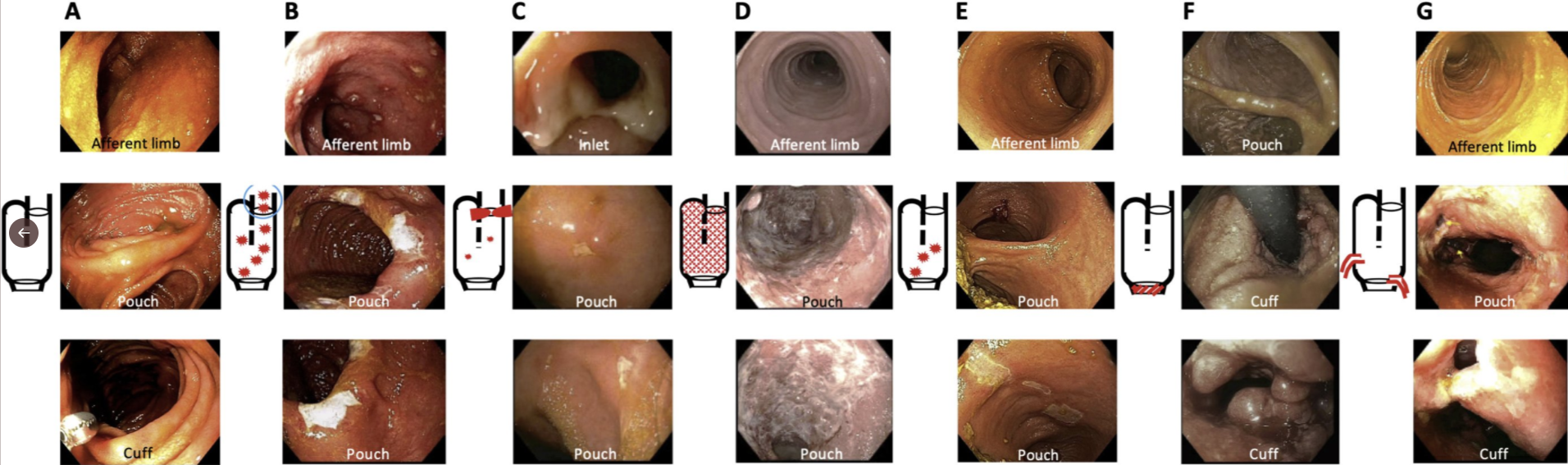
The authors retrospectively reviewed 1359 pouchoscopies and classified them into 7 main pouch phenotypes: (1) normal, (2) afferent limb involvement, (3) inlet involvement, (4) diffuse, (5) focal inflammation of the pouch body, (6) cuffitis, and (7) pouch with fistulas noted 6 months after ileostomy takedown.
Key finding: Diffuse inflammation was associated independently with pouch excision (hazard ratio, 2.69; 95% CI, 1.34–5.41; P = .005).
This retrospective study had 235 patients (median age 38 years). 90% had endoscopy at a median of 2 days from admission. Key findings:
155 of the 235 patients (66.0%) responded to steroids
78.1% (25 of 32) of patients with concurrent CRP ≥50 mg/L, albumin ≤30 g/L, and increased endoscopic severity (severe on physician’s global assessment) (maximum score = 3) did not respond to IV steroids (positive predictive value [PPV] 78.1%, negative predictive value [NPV] 87.1%).
Comparison with Truelove and Witts Score: 56 of 119 (47.1%) of those classed TWS severe did not respond to steroids. Previously TWS score of acute severe ulcerative colitis (ASUC), defined by at least 6 bloody stools per day plus at least 1 marker of systemic disturbance has been associated with a 19% risk of colectomy during admission.
My take: In patients with ulcerative colitis who present with low albumin and high CRP values, early escalation of medical therapy is highly likely; don’t forget to check a PPD or quantiferon Gold assay early on.
Dr. Joseph D. Feuerstein, gastroenterologist at Beth Israel Deaconess Medical Center in Boston… “It’s rising in incidence and prevalence throughout the world,” he said, and gastroenterologists are still trying to figure out why it shows up when it does in different people.
Crohn’s disease was first described in 1932 by Dr. Burrill B. Crohn…
Prompt diagnosis and appropriate therapy to suppress inflammation in the digestive tract are extremely important because a delay can result in scar tissue and strictures that are not reversed by medication…
Crohn’s is not curable and most patients have to stay on medication indefinitely. That can create yet another stumbling block. The biologics are very costly…












{kind=link}