F Muller et al. NEJM 2025;393:1239-1241. CD19 CAR T-Cell Therapy in Multidrug-Resistant Ulcerative Colitis
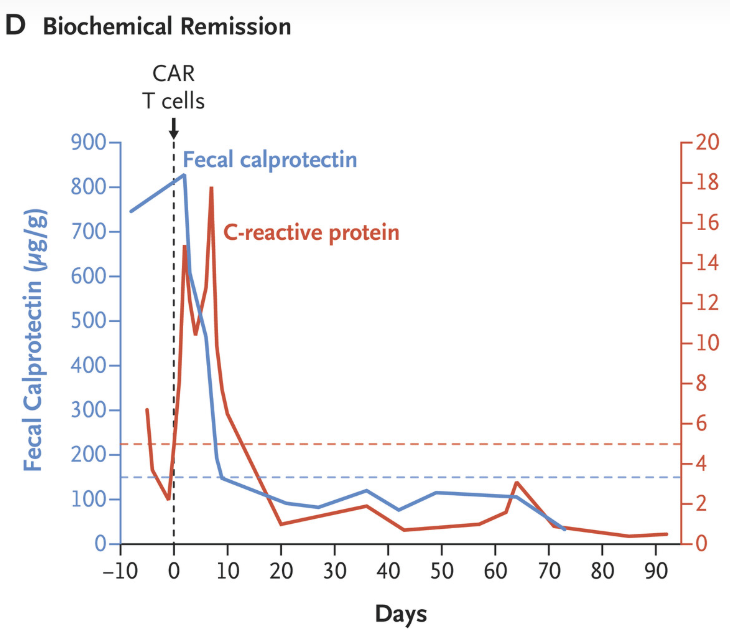
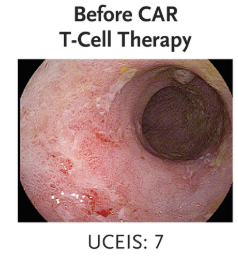
This case study involved the use of “autologous chimeric antigen receptor (CAR) T cells targeting CD19 in a 21-year-old woman with severe multidrug-resistant ulcerative colitis, who had declined colectomy. Previous treatments with prednisolone, mesalamine, infliximab, ustekinumab, ozanimod, filgotinib, vedolizumab, upadacitinib, and cyclosporine combined with mirikizumab had not induced clinical remission.”
“Clinical and biochemical remission occurred and were maintained over the 14-week follow-up period… without the use of concomitant therapy. Endoscopic, histologic, and ultrasonographic assessments showed signs of mucosal healing over time….These data suggest the possibility that CD19 CAR T-cell therapy can induce rapid drug-free remission in refractory ulcerative colitis, a disease that was previously thought to be largely B-cell–independent, given that rituximab treatment showed no efficacy..”
My take: This is only a single case report. However, it shows that modulation of the immune system could potentially cure ulcerative colitis. At the same time, long term adverse effects of CAR-T therapy will need to be monitored.
Methods: “Faecal calprotectin was measured in asymptomatic FDRs aged 6–38 years; those with persistent elevation, defined as >70 µg/g in at least two separate tests, were offered panenteric video capsule endoscopy or ileocolonoscopy”
Population: 331 (35%) first-degree relatives (FDRs) (from a group of 950) agreed to be screened: 63 (19%) had persistently elevated calprotectin, of whom 42 underwent further evaluation
Key findings:
From the initial screened cohort of 331 patients, nine (2.7%) had endoscopic appearance compatible with presymptomatic CD, and 22 (6.6%) had non-specific macroscopic mucosal changes
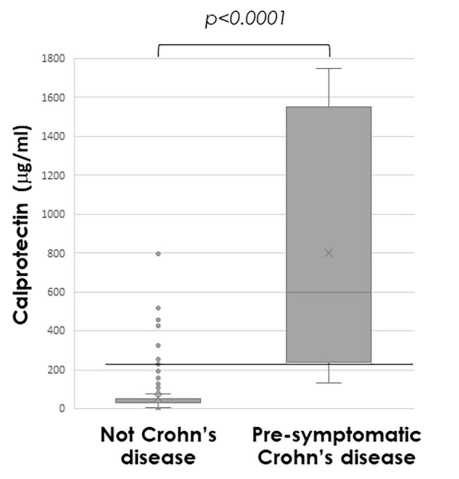
Median calprotectin was significantly higher in those with presymptomatic CD (772µg/g (IQR 279–1685)) compared with others (31µg/g (IQR 30–61), p<0.0001)
Calprotectin >225 µg/g predicted presymptomatic CD (area under the receiver operating characteristic curve 0.97 (95% CI 0.94 to 1.0; p<0.001; sensitivity 89%, specificity 94%)
Discussion Points:
“There is no universally accepted definition for preclinical stages of CD, and the distinction between these stages remains partly subjective.”
“The lack of longitudinal follow-up is also a limitation, but this will be completed as part of the PIONIR trial.”
My take (borrowed in part from the authors):
Identification of pre-symptomatic CD “can facilitate designing targeted interventions and defining inclusion criteria for prevention trials.” The disease may be more modifiable in the early stages of disease.
This trial suggests the calprotectin threshold of >70 is too low to target screening. For specificity, the study showed that persistent elevation above 225 merits investigation; though, it has been our practice to use a threshold of >150 for children older than 5 years.
Approximately 5% of asymptomatic FDRs of CD patients have evidence of pre-symptomatic CD and approximately 10% more have non-specific mucosal changes when evaluated
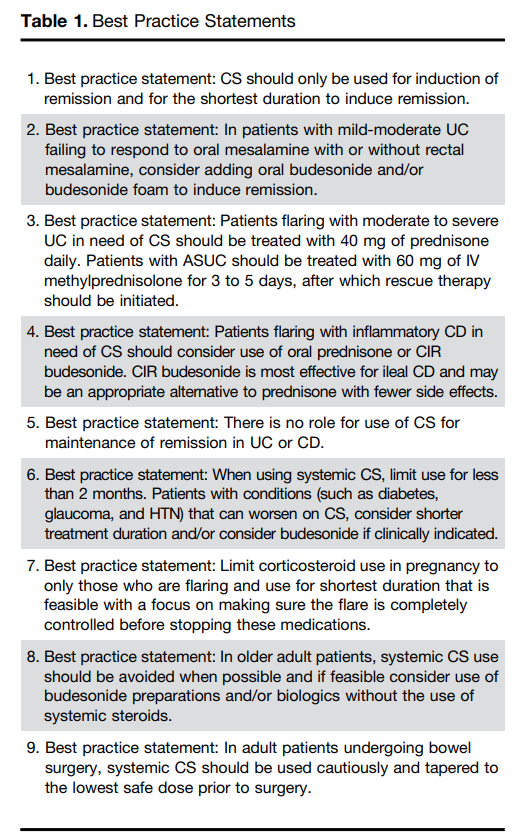
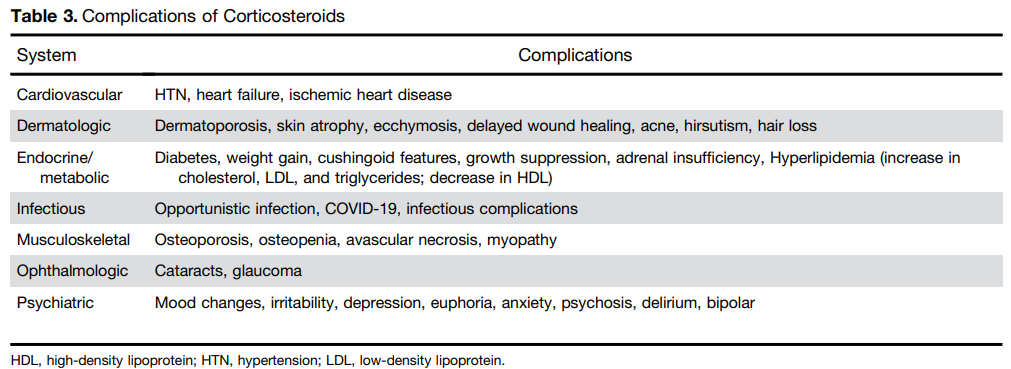
Steroids are commonly used and misused for inflammatory bowel disease. This article reviews best practices, steroid formulations/dosing, and potential complications.
For moderate to severe ulcerative colitis (in adults), the authors recommend treatment with 40 mg of prednisone daily. Patients with ASUC (acute severe ulcerative colitis) should be treated with 60 mg of IV methylprednisolone for 3 to 5 days, after which rescue therapy should be initiated
Use of budesonide is recommended as an option for many clinical situations to minimize steroid adverse effects. These situations include mild-moderate UC failing to respond to mesalamine, ileal CD and older patients
Postoperative complications: “In the postoperative period, patients treated with CS had a higher risk of both infectious complications (aOR, 3.69; 95% CI, 1.24–10.97) and major infectious complications (aOR, 5.54; 95% CI, 1.12–27.26) [Abrerra et al].135 Subramanian pooled data from 7 studies showing that preoperative CS use is associated with increased postoperative complications (OR, 1.41; 95% CI, 1.07–1.87) as well as infectious complications.
The authors note that corticosteroids “remain widely available and are an effective short-term option for induction of remission in patients with active UC or inflammatory CD. However, their well-described and significant safety profile warrants proactive strategies to limit their use through non-systemic formulations, short-term exposures, steroid-sparing maintenance options, and most recently, complete steroid avoidance strategies.”
My take: Continuing steroids when they are not effective prior to potential surgery (eg. ASUC) remains a frequent problem. Sometimes, it is difficult to know it they are helping some.
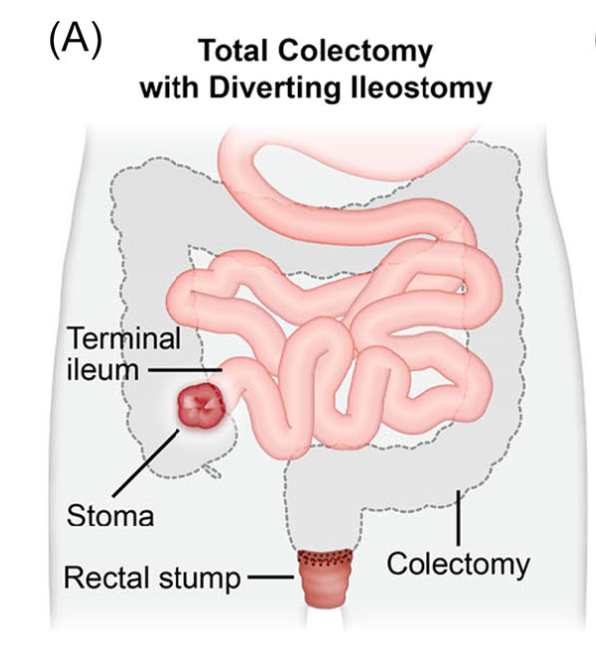
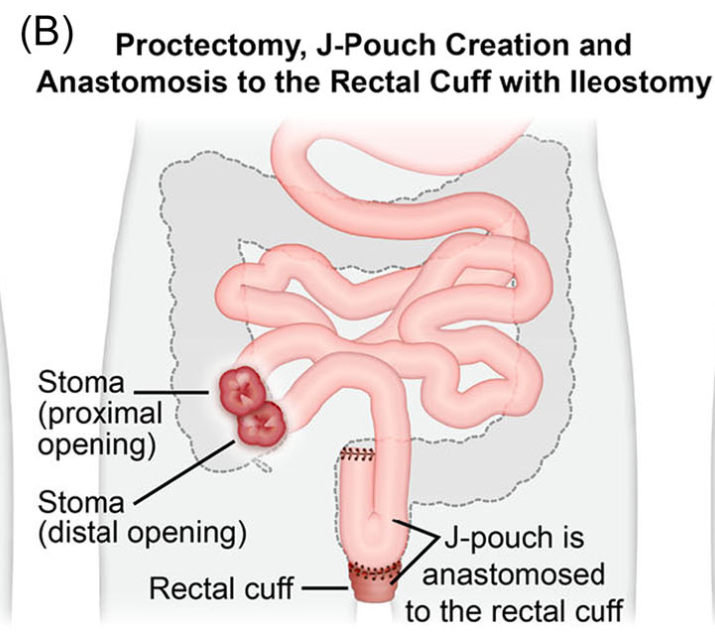
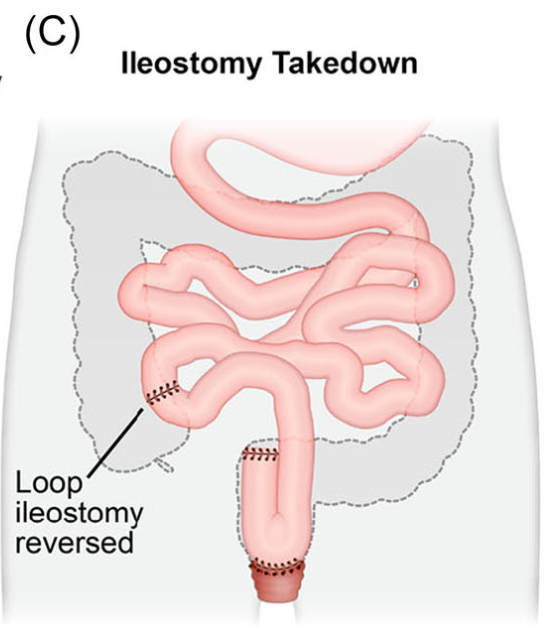
A Phillip et al. J Pediatr Gastroenterol Nutr. 2025;81:913–921. A narrative review of the ileal pouch in pediatric inflammatory bowel disease and familial adenomatous polyposis
Introduction: Total proctocolectomy with ileal pouch-anal anastomosis (IPAA) can be a life changing solution for a subset of pediatric inflammatory bowel disease (IBD) and familial adenomatous polyposis (FAP) patients. For patients with severe disease a three-stage approach is commonly performed.
Creation of IPAA -Three Stages:
Endoscopic Images and IPAA Anatomy:
The article provides guidance on complications including pouchitis, CD-like inflammation of the pouch, J-pouch failure, fertility after IPAA along with follow-up/screening recommendations.
As for screening, adult guidelines recommend annual screening for IBD patients with high risk features—previous dysplasia, primary sclerosing cholangitis, type C mucosa, refractory pouchitis. In those without these features, guidelines are variable, with one suggesting screening every 5 years. In FAP patients, the recommendation for surveillance screening following IPAA is pouchoscopy every 1–2 years.8
My take: Most pediatric gastroenterologists are not proficient in pouch management due to the small number of our patients needing IPAA. This review provides a terrific review/resource.
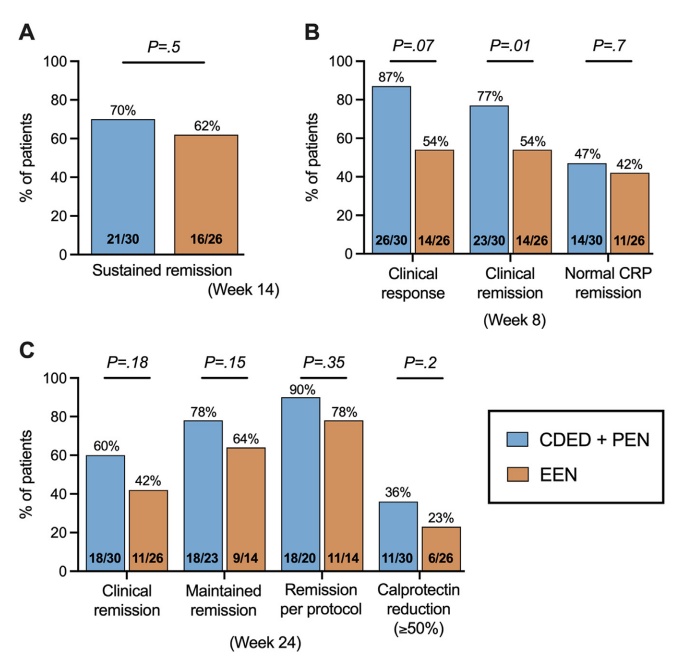
In this “DIETOMICS” study with 56 children with mild-to-severe Crohn’s disease, after a 2 week exclusive enteral nutrition (EEN) diet, 30 patients were randomized to CDED and 26 to EEN.
Diet intervention: The CDED group followed 3 diet phases over 24 weeks: phase 1 (weeks 3–8) supplemented with 50% PEN; phase 2 (weeks 9–14) with 25% PEN, as described previously16; and phase 3 (weeks 15–24) with gradual introduction of more foods, including 1 and 2 free meals per week from weeks 15 and 18, respectively.17 Patients in EEN group received 8 weeks of EEN followed by gradual introduction of free diet with 25% PEN up to week 24.
Key findings:
This study with a relatively small number of enrolled patients had a lot of variables in dietary parameters. “An additional potential confounder in this study is the use of IMM therapy. Although both groups were recommended to initiate IMM therapy from weeks 4 to 5 to maintain remission, several CDED patients opted for monotherapy with CDED and preferred to delay medication initiation. Interestingly, 90% of patients on CDED without IMM therapy were in remission at week 14 and 100% were in remission at week 2” (possibly impacting decision not to use IMM).
My take: This study adds another piece of information to the puzzle on dietary therapy for Crohn’s disease. The authors note the following: “while CDED shows promise as a standalone therapy in some cases, in more severe cases it may be more appropriately as an adjuvant to top-down treatment with early anti-TNF.4 Recent research and guidelines advocate for a top-down approach (anti-TNF ± nutrition) for more severe disease, emphasizing the integration of anti-TNF therapy with nutrition.8,29 This approach is crucial during critical growth stages, as the conventional step-up method may lead to ineffective use of IMM with prolonged steroid exposure and growth issues.12“
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition
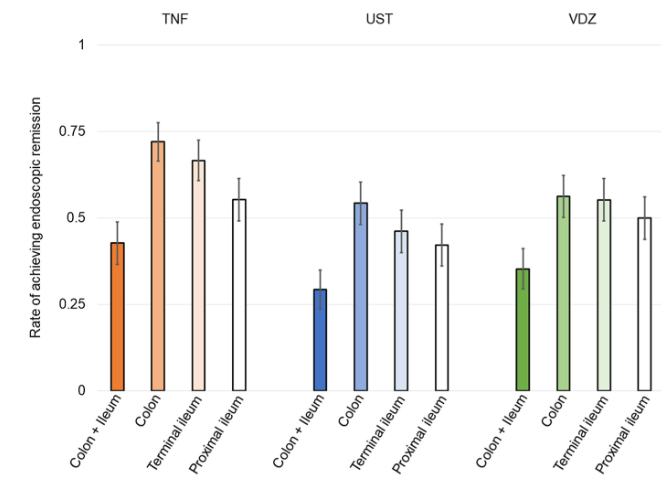
This multicenter prospective study (n=253) examined efficacy of treatment in patients with proximal ileal disease using balloon-assisted enteroscopy (BAE). The recruited patients had a mean disease duration of 4 years. 52% were naive to biologic treatment at baseline.
Key findings:
At baseline, 74 patients (29.2%) had proximal ileal ulcerations without terminal ileal ulcerations
At week 26, after treatment with anti-TNF therapy (n=103), ustekinumab (n=99) or vedolizumab (n=51), endoscopic remission was achieved in 91 patients (36.0%). Of the patients with complete ulcer healing of the terminal ileum, 28.6% (22/77) had residual ulcers in the proximal ileum
The rate of endoscopic remission in the proximal ileum (50.9%) was relatively lower compared with the colon (63.4%) and terminal ileum (56.7%)
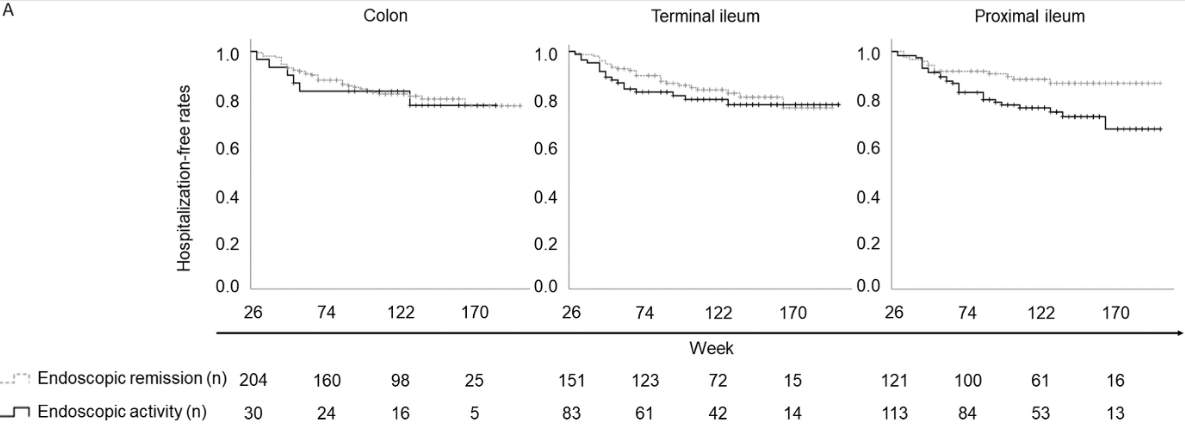
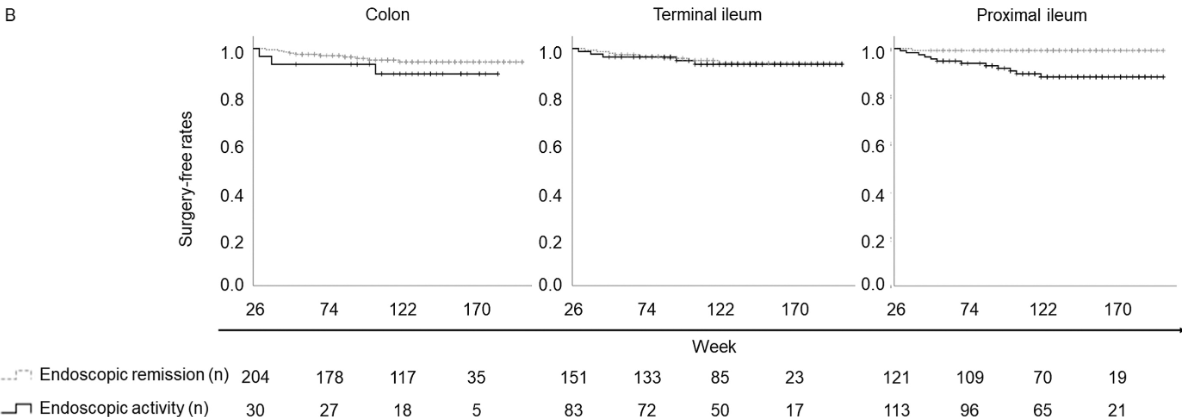
After a median follow-up of 134 weeks, residual ulcerations in the proximal ileum were associated with a poorer prognosis (P = .0126 for hospitalization and P = .0014 for surgery). In contrast, there was no significant differences in hospitalization and surgery associated with endoscopic activity vs remission in the colon or terminal ileum.
Discussion: Residual “proximal ileal ulcerations … are associated with a poorer prognosis…Additionally, we confirmed that proximal ileal inflammation is less responsive to biologic therapies compared with colonic inflammation. Although the reasons for this disparity remain unclear”
My take: Balloon-assisted enteroscopy is not frequently used in the setting of inflammatory bowel disease, particularly in pediatrics. MRE is typically used to follow proximal small bowel disease, though it has less sensitivity for luminal mucosal disease.
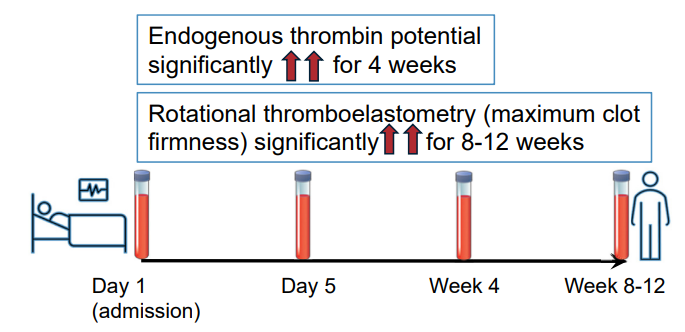
Methods: In this prospective study, twenty-seven adult patients with ASUC and 25 control patients with quiescent ulcerative colitis were recruited. Thrombin generation (endogenous thrombin potential), rotational thromboelastometry (EXTEM and FIBTEM maximum clot firmness), procoagulant factors, anticoagulant factors, and fibrinolytic markers were assessed for those with ASUC on admission (Day 1), Day 5, 4 weeks, and at 8–12 weeks. These assessments were performed on a single occasion for control patients.
Key findings:
Discussion:
“Patients with ASUC had a hypercoagulable profile on initial presentation to the hospital, before receipt of LMWH, which was consistently demonstrated by individual and global assays of coagulation. The most marked elevations of individual factors at presentation were seen in the levels of Clauss fibrinogen, platelets, VWF, and FVIII, alongside heightened levels of the inhibitors of fibrinolysis PAI-1 and TAFIa.”
“This hypercoagulable state persisted for many weeks after hospital discharge, with levels of FVIII, fibrinogen, VWF, and inhibitors of fibrinolysis (TAFIa) remained significantly elevated at all timepoints up to 12 weeks, compared with the control population. This is despite intensive treatment for ASUC in all patients.”
“VTE and pulmonary embolism are 1 of the leading causes of morbidity and mortality during IBD flare-ups. The findings from this study reinforce the importance of thromboprophylaxis administration to all patients with ASUC at first presentation to hospital.”
My take: This study is in adults; the risk of VTE is lower in children and guidance on VTE prophylaxis is not clear.
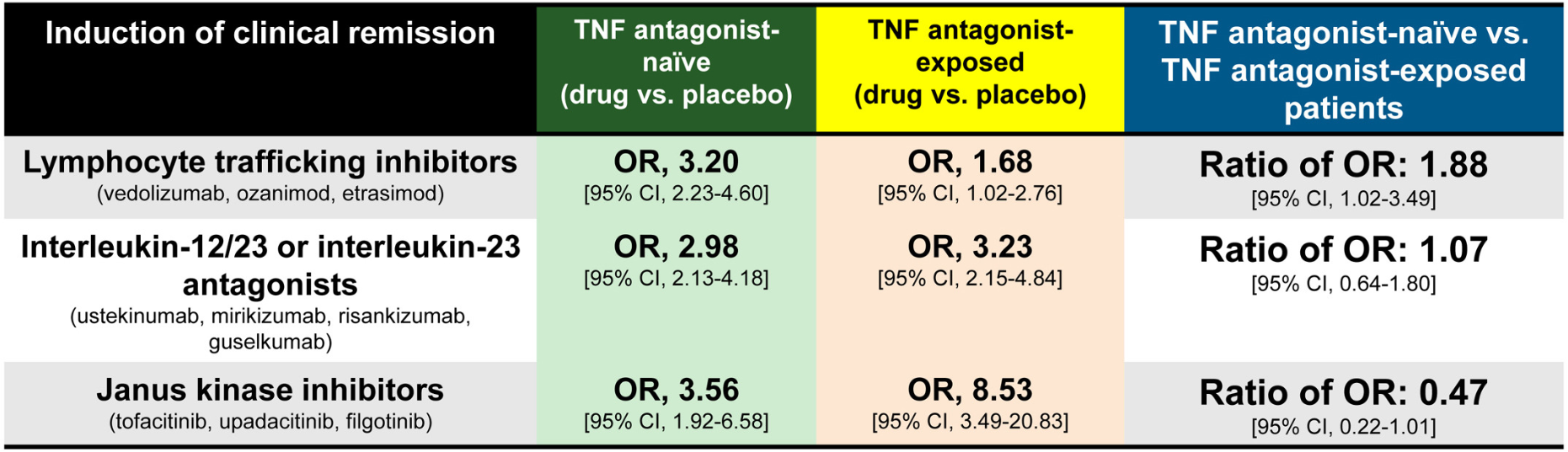
Methods: Meta-analysis of 17 randomized controlled trials in 8871 adults with moderate-severe UC. The authors calculatedthe ratio of odds ratio of achieving remission with active drug vs placebo, in TNF antagonist–naïve vs TNF antagonist–exposed patients.
Key findings:
JAK inhibitors: Less efficacious in TNF antagonist–naïve vs exposed patients (6 trials; ratio of OR, 0.47)
IL-23 antagonists: No significant difference was observed in efficacy of selective interleukin-23 antagonists vs placebo in TNF antagonist–naïve vs exposed patients (6 trials; ratio of OR, 1.07)
Lymphocyte trafficking inhibitors: More efficacious in TNF antagonist–naïve vs exposed patients (5 trials; odds ratio [OR], 1.88)
Discussion:
This study “confirmed prior observations that exposure to TNF antagonists significantly reduces the efficacy of lymphocyte trafficking inhibitors in inducing remission, including both vedolizumab and S1P receptor modulators, by approximately 50%.In contrast, prior exposure to TNF antagonists was associated with a significant increase in the efficacy of JAK inhibitors in inducing remission, with 2-fold higher efficacy in TNF antagonist–exposed vs TNF antagonist–naïve patients”
In the SELECT-COMPARE trial in patients with rheumatoid arthritis, there was also an improved response to upadacitinib in patients with prior adalimumab.
“The current findings raise the intriguing possibility that exposure to TNF antagonists could result in lasting effects on the immune system that differentially alter responsiveness to therapies with distinct mechanisms of action”
My take: This study suggests that JAK inhibitors are a good choice for secondary therapy after anti-TNF agents. Other factors, besides efficacy, including safety, extraintestinal manifestations, and cost, have to be considered as well.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Today and tomorrow I am highlighting two adult clinical guidelines both of which are equivalent to up-to-date textbook chapters with specific recommendations; both are open access. In addition, the articles have accompanying author podcasts. Thanks to Ben Gold for these references.
Table 2 in the UC guideline makes 54 recommendations and Table 3 provides 57 key concepts.
Selected Management Recommendations:
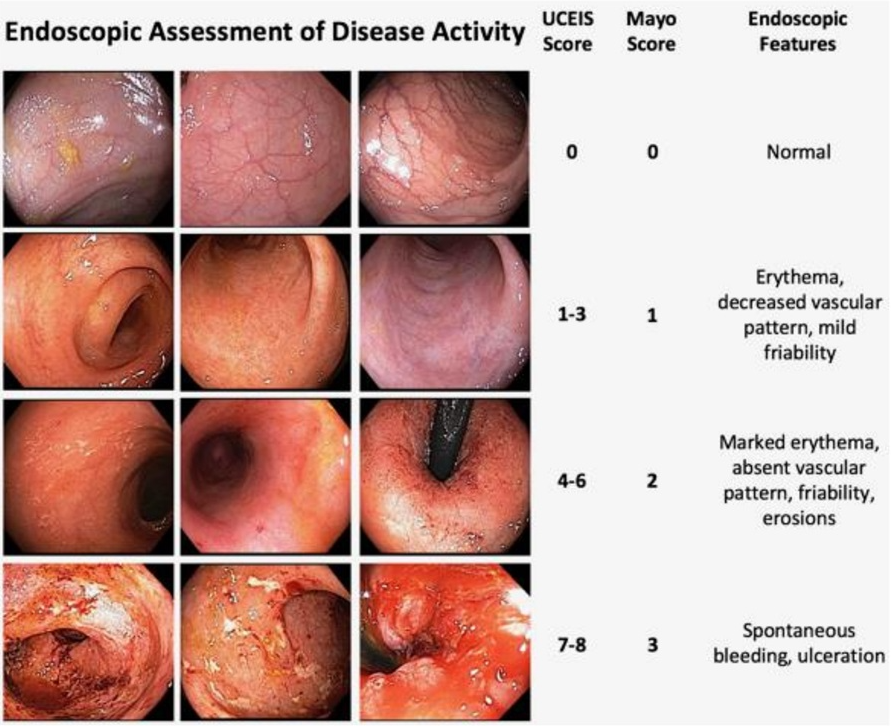
Table 2, #4: We recommend treating patients with UC to achieve endoscopic improvement (Mayo score 0 or 1) to increase the likelihood of sustained steroid-free remission and to prevent hospitalization and surgery
Table 2, #5: We recommend the use of FC (fecal calprotectin) in UC to assess response to therapy, to evaluate suspected relapse, and during maintenance
Table 2, #33: When infliximab is used as induction therapy for patients with moderately to severely active UC, we recommend combination therapy with a thiopurine
Table 2, #43: Recommend continuing tofacitinib or upadacitinib as compared with no treatment for maintenance of remission in patients with prior moderately to severely active UC now in remission after induction with tofacitinib or upadacitinib. **The authors recommend continuing each biologic that achieved remission with induction therapy (#38-#43)
Table 2, #51: In patients with ASUC failing to adequately respond to intravenous corticosteroids (IVCS) by 3 days, we recommend medical rescue therapy with infliximab or cyclosporine (Strong recommendation, moderate quality of evidence).
Key concepts:
Table 3, #29: Patients who are primary nonresponders to an anti-TNF (defined as lack of therapeutic benefit after induction and despite sufficient serum drug concentrations) should be evaluated and considered for alternative mechanisms of disease control (e.g., in a different class of therapy) rather than cycling to another drug within the anti-TNF class.
Table 3, #31: Subcutaneous infliximab and vedolizumab are considered equivalent to the standard intravenous maintenance dosing of these agents. The equivalence of the subcutaneous formulations for induction or as substitution for escalated doses of these therapies has not been robustly established.
Table 3, #41: Patients with UC should have available all medical options as recommended by their doctor and healthcare team. Third-party payers and requirements for step therapy should not come between the patient and their healthcare team in making decisions about treatment for UC.
Table 3, #48: All patients with ASUC should undergo a flexible sigmoidoscopy within 72 hours and preferably within 24 hours of admission. This should be used to assess endoscopic severity of inflammation and to obtain biopsies to evaluate for cytomegalovirus (CMV) colitis.
Table 3, #51: Nonsteroidal anti-inflammatory drugs (NSAIDs), narcotics, and medications with anticholinergic side effects should be avoided in ASUC.
Table 3, #57: In patients with ASUC initiating infliximab, dose intensification should be considered for those patients with low serum albumin (<2.5 g/dL).
My take: This article does an excellent job of summarizing current available evidence and good practice. Many of the recommendations may be helpful in garnering approval from third party payers.
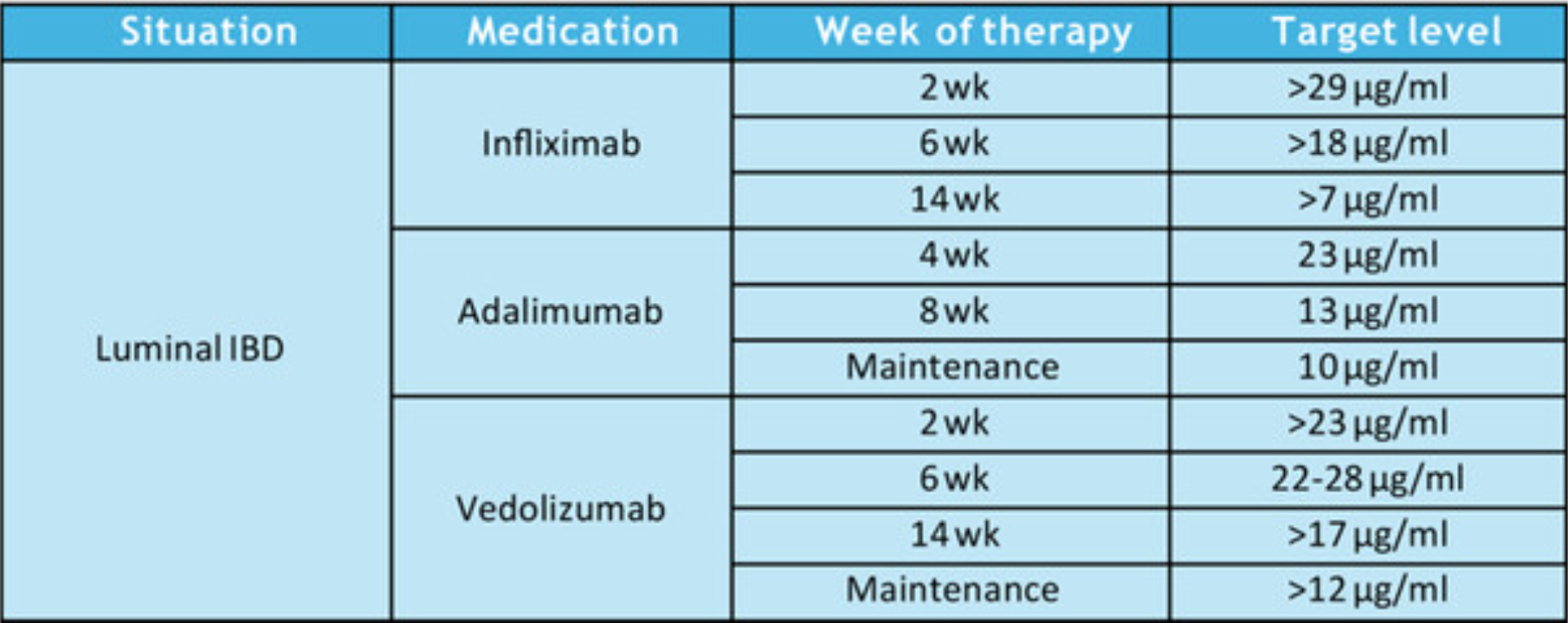
Therapeutic Drug Targets Based on Condition, Medication and Time of Therapy:
Discussion Points:
Pediatric Dosing is Different: “Pediatric studies have also determined adult infliximab targets are insufficient…In a prospective pediatric study, Clarkston et al. found that a trough level of 29 μg/mL at 2 weeks is required to achieve both clinical and biologic response. Patients with lower trough levels had 13-fold greater odds of clinical nonresponse. Additionally, a trough of 18 μg/mL at 6 weeks was associated with improved response. Patients with lower trough levels had sixfold greater odds of clinical nonresponse. They also observed that patients who did not achieve a trough >5–7 μg/mL by 14 weeks of therapy had a 21-fold increase in the odds of clinical nonresponse.62“
Undetectable/very low anti-TNF levels: “If the serum level is extremely low or undetectable, then full re-induction is warranted in addition to dose escalation.”
Timing of TDM: “As a practice point, TDM is routinely recommended at the end of induction for most patients. We recommend obtaining TDM earlier during induction in at-risk populations, including younger age children, those with hypoalbuminemia, and those with increased inflammatory burden.”
Maintenance proactive TDM: “Based on prospective randomized trial evidence, we recommend proactive TDM during maintenance every 6–12 months…yearly proactive TDM was associated with 55% reduced risk of developing antidrug antibodies.26“
Increased Antidrug Antibodies with Lower Infliximab Dosing: “In the pivotal REFINE study on immunogenicity in pediatric IBD, Coleman et al. found that antibodies to infliximab were detected in 68% of patients in the cohort, and starting dose under 7.5 mg/kg was one of the strongest predictors of developing antidrug antibodies.4“
Higher Doses Prevent Antidrug Antibodies: “The best available evidence for preventing immunogenicity supports initiating therapy with infliximab doses greater than 8 mg/kg, and in the case of hypoalbuminemia, doses greater than 10 mg/kg. For children <40 kg, doses of 200 mg/m2 are more appropriate.”
Perianal fistulas: “Overall, there is less evidence to support adalimumab use over infliximab for treatment of perianal fistulas. It is possible that adalimumab may have lower efficacy for perianal fistula.105 However, it is unclear if this is inherent to adalimumab, or if it relates to less frequent TDM or less frequent dose escalation in practice.”
Vedolizumab: “In general, as with other biologic therapies, a higher serum vedolizumab concentration is associated with higher likelihood of treatment response…Multiple studies identified that in patients with IBD (either UC or CD) early trough levels at Week 2132 with a cut off of >23.2 μg/mL or Week 6133, 134 with a cut off of above 22–28 μg/mL or at Week 14135) above 16.55 μg/mL predicted a higher likelihood of sustained response over the first year. In regard to clinical remission one study identified that corticosteroid free, clinical and biochemical remission was correlated to higher trough vedolizumab concentration.136“
Vedolizumab in younger patients: “Children under 30 kg require vedolizumab doses of 200 mg/m2 or 10 mg/kg.”
My take: “This NASPGHAN position paper should also serve to document that high-dose therapy, especially guided by TDM, is evidence-based standard of care.” This article clearly establishes three key points:
“Intensive anti-TNF⍺ dosing strategies are not experimental. The initial doses of infliximab and adalimumab approved by the United States Food and Drug Administration (FDA) routinely lead to under-treatment, poor outcomes, and treatment discontinuation.60, 117 There is a rich, corroborated, and verified evidence-base to support the safety and efficacy of high-dose therapy anti-TNF⍺ therapy when clinically indicated, especially as supported by TDM.50, 62, 65, 100, 101, 103, 118“
Therapeutic drug monitoring is essential in the pediatric population to optimize drug levels, allow many patients to do well with monotherapy, and to help avoid development of antidrug antibodies.
The best available evidence supports TDM during induction of vedolizumab as well.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.