- Full link to CCFA Recommendations (from 3/11/20): Guidance for Pediatric Caregivers and Patients —Updates on COVID-19 and IBD
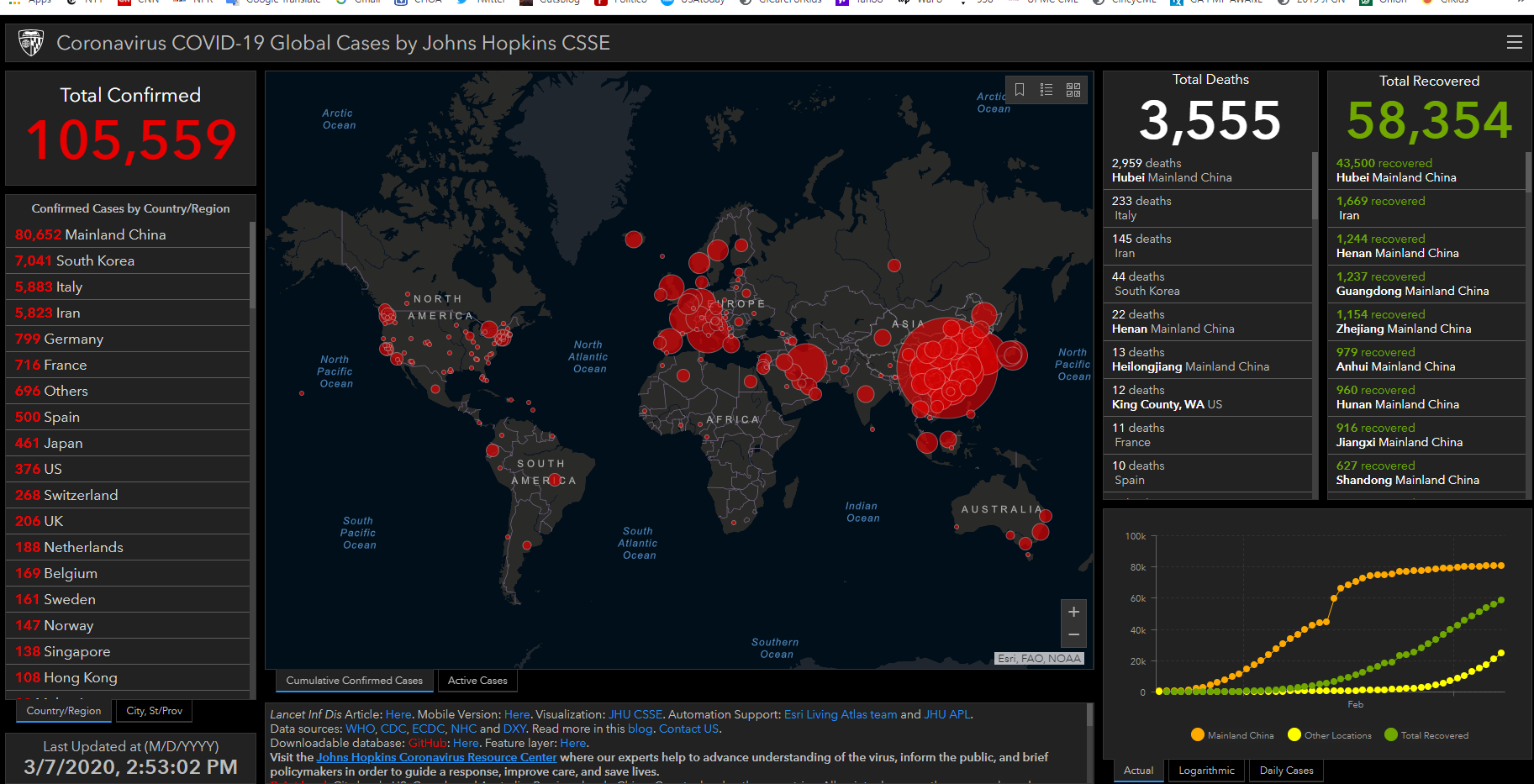
- Link to Johns Hopkins daily tracker: COVID19 Caseload & Outcomes Worldwide
- Link to New NASPGHAN/ICN COVID19/IBD worldwide registry: Can report cases at the following: SECURE-IBD Registry
- The Centers for Disease Control provides updates on the virus and safety information for the public and healthcare professionals. Here is a CDC Fact Sheet.
- The State Department provides a list of travel advisories for those who are planning to fly outside of the United States.
For Georgia:
- The State of Georgia has a new COVID-19 hotline. It can be reached by calling (844) 442-2681.
- The Georgia Department of health has put together a Daily Status Report which you can find here.
NASPGHAN statement regarding Coronavirus (SARS-CoV-2) Associated Infectious Disease (COVID -19) and Pediatric GI Patient Care and Providers.
Dear Members,
In view of the COVID -19 pandemic, care of our pediatric GI patients and at the same time our pediatric GI providers (i.e. physicians and other members of the healthcare team) is an utmost priority at NASPGHAN. NASPGHAN is working on several initiatives concurrently, and we are writing at this time to make you aware.
1. The Endoscopy Committee and the Clinical Practice Committee are working on a statement regarding elective procedures for pediatric GI patients with respect to this highly contagious pathogen, COVID to both preserve Personal Protective Equipment (PPE) as well as limit potential exposure.
2. A task force of leaders from NASPGHAN, ESPGHAN, LASPGHAN, and Asia (Hangzhou, China) will be writing a commentary to be published in the JPGN, our journal, with what COVID-19 means to the pediatric gastroenterologist.
3. Mike Kappleman of UNC, ICN, NASPGHAN and in particular the IBD Committee, are launching a prospective, real-time monitoring study of COVID-19 in IBD patients. The study is IRB and HIPAA approved and will link its data with that collected by the European Porto group’s study of coronavirus in IBD patients in Europe and Asia, thereby allowing an operational real-time active surveillance network for children and adolescents with IBD (our patients).
4. Jason Silverman, Jennifer Lee, and Peter Lu are putting together a special episode of the Bowel Sounds Podcast™ including relevant up-to-date guidelines and information about COVID-19 as it relates to our members and our patients.
5. The Endoscopy Committee and Clinical Practice Committee are working on information and options for telemedicine and virtual health, given the more recent announcement by CMS and the White House/President Trump in terms of changes in reimbursement given the coronavirus pandemic.
6. Within the next 24 hours, the NASPGHAN Website, as well as GIKids.org will house resources and links to the Centers for Disease Control and Prevention (CDC), the American Academy of Pediatrics (AAP), Crohn’s and Colitis Foundation (CCF), the Canadian Association of Gastroenterology (CAG) and the Joint GI Societies Statement (adult-based), including ASGE, ACG, AGA on Endoscopic procedures in the face of COVID-19.
7. Finally, please feel free to send us suggestions that would help our pediatric GI community work towards creative solutions during this time.
Sincerely,
Karen F. Murray MD
President, NASPGHAN
James Heubi MD
Past President, NASPGHAN
Benjamin Gold MD
President Elect, NASPGHAN
Jeannie S. Huang MD
Secretary Treasurer, NASPGHAN
Rina Sanghavi MD