Background: “Measles is a highly contagious disease and, despite the availability of a safe and effective vaccine, remains still an important cause of childhood death worldwide [1,2]. The risk of severe illness in measles-naive individuals is particularly high in immunocompromised patients with inflammatory bowel disease (IBD) or after liver transplantation (LT) [3]…Ideally, vaccination with live attenuated vaccines (LAVVs) should be completed four weeks before organ transplantation or the initiation of immunosuppressive therapy (IST) to allow for the live vaccine’s incubation period and minimize the risk of vaccine-associated disease…LAVVs are considered contraindicated during IST due to safety concerns and limited experience.”
Methods: “In this prospective multicenter observational study (DRKS00014569) 22 children and adolescents with incomplete MMR vaccination status were identified… with stable immunosuppressive therapy in the last three months with no evidence of underlying disease activity…Sixteen patients were vaccinated against MMR, eleven after liver transplantation and five with inflammatory bowel disease. At the time of vaccination, four patients were receiving moderate (e.g., tacrolimus drug level below 5 ng/ml), eleven were receiving high-intensity immunosuppression (e.g. anti-tumor-necrosis factor agents, mycophenolate mofetil) and one child had previously discontinued immunosuppressive treatment.”
Immediately prior to the references, the authors provide a downloadable document detailing how they chose to categorize the degree of immunosuppression and their precise protocol, including immunologic pretesting and drug contraindications as noted below.
Key findings:
There were no serious adverse events or complications related to the vaccination
In children receiving immunosuppressive medications, the seroconversion rate for measles after the first MMR vaccination was 73.3 % (11/15) and after the second vaccination 80 % (12/15)
My take: In carefully-selected immunocompromised pediatric patients, the MMR vaccine may be safe. However, given the small numbers receiving vaccination in this study, the absolute safety is unclear. Even infrequent adverse effects would be problematic. This study’s protocol could be helpful for those considering vaccination in immunocompromised populations with a measles epidemic. For now, the most important approach is improving vaccination rates in those (especially family members) without contraindications.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
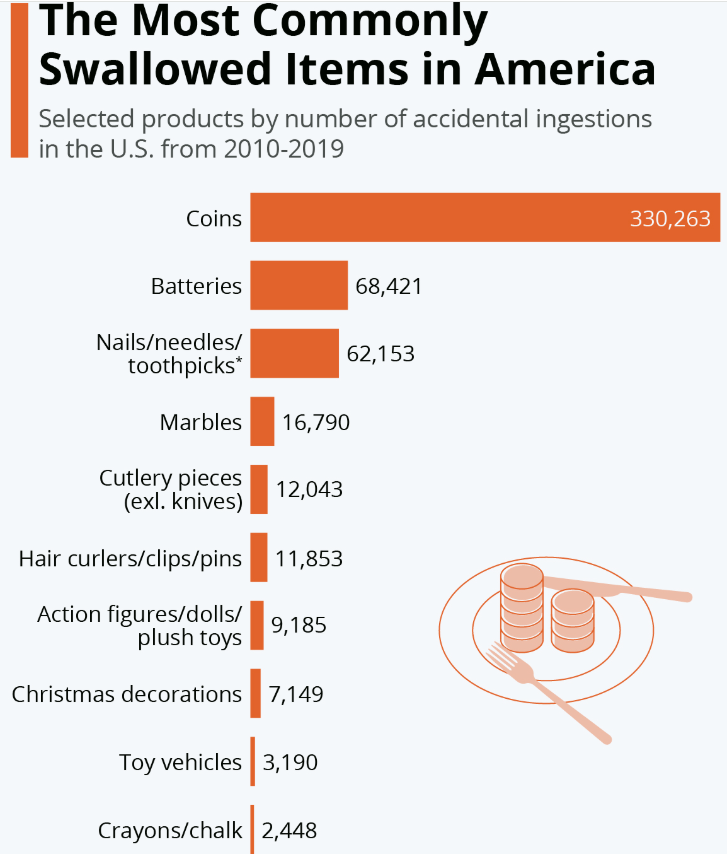
As I noted in a blog in 2012, I had advocated for removal of the penny due to frequent ingestions (starting more than 20 years ago) (link: “Watch for change in the stools”). Now it appears I will finally get my wish.
In recent weeks, Republican and Democratic lawmakers introduced separate bills in the House of Representatives and the Senate calling for an end to penny production. The change means that businesses will have to start rounding the prices of cash transactions up or down to the nearest five-cent nickel as the number of pennies in circulation dwindles.
The Treasury’s penny phase-out plan was first reported by the Wall Street Journal…The cost of producing the penny has risen from 1.3 cents per coin to 3.69 cents over the past 10 years, according to the Treasury. It said stopping production will lead to immediate annual savings of $56 million.The penny was first issued by the government in 1793
The following statistic will delight fans of obscure facts and overbearing bureaucracy: According to the U.S. Consumer Product Safety Commission, more than 850,000 accidental ingestions of everyday objects were recorded in the U.S. between 2010 and 2019. ..Coins topped the list of accidental ingestions, with around 33,000 being recorded each year (more might go unreported).
My take: While this is a step in the right direction, there are still 114 billion pennies currently in circulation in the U.S. according to the Reuters article. Perhaps, other coins will be ingested less in the coming years too as so many business transactions are via smartphones and credit cards.
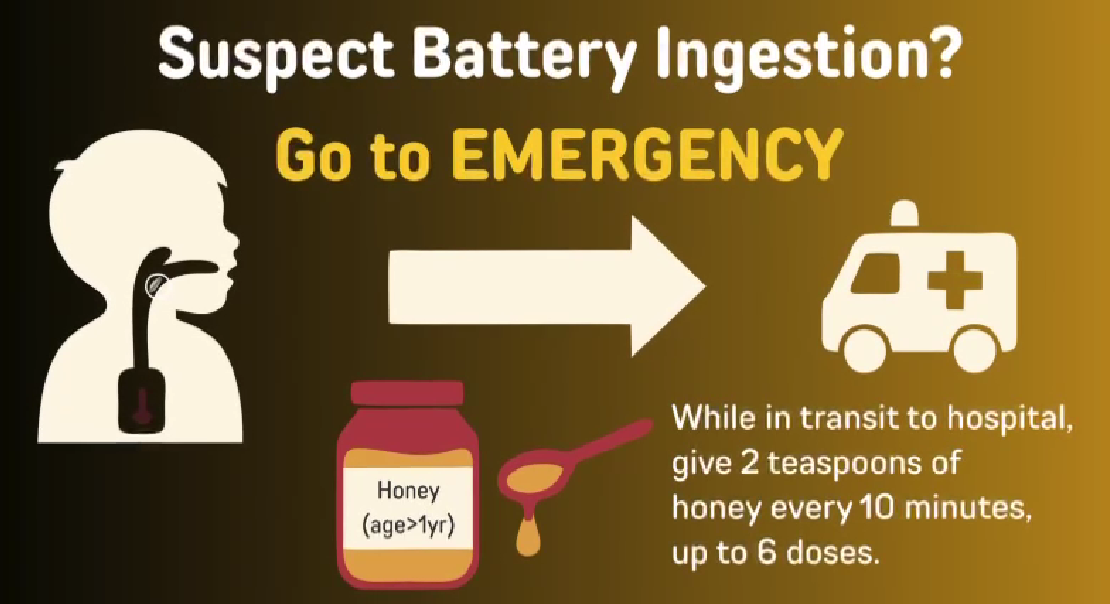
Button batteries are a much more serious ingestion than a coin. For World Button Battery Day, here’s a link to a 3 minute video from FISPGHAN. FISPGHAN Button Battery Video
The video provides a simple explanation of the problem though at times it is not certain who the target audience is. Particularly the first part feels like a video for kids rather than for parents. Thanks to Ben Gold for sharing this link.
Mitigation Efforts for Button Batteries (also includes case report of aorto-esophageal fistula and emergency surgery 25 days after ingestion of a button battery)
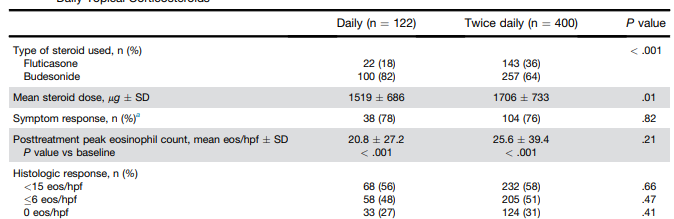
Methods: This was a retrospective cohort study using the UNC EoE Clinicopathologic Database of newly diagnosed patients with EoE treated with a tCS who had a follow-up endoscopy with biopsy. In total, there were 522 patients, including 195 pediatric patients (<18 yr). 122 patients received once daily dosing and 400 patients received twice daily dosing.
At our center, patients are typically treated on a clinical basis with either oral viscous budesonide or fluticasone from a multidose inhaler, with daily doses ranging from 1–2 mg for budesonide and 440–1760 μg for fluticasone based on patient size and at the discretion of the provider.
Key findings:
Global symptomatic response (78% vs 76%; P = .82), posttreatment eosinophil count (20.8 vs 25.6; P = .21), posttreatment EoE Endoscopic Reference Score (2.2 vs 2.2; P = .92), and histologic response (<15 eos/hpf; 56% vs 58%; P = .66) did not differ by dosing frequency
Candida was less frequent with daily dosing (2% vs 8%; P = .04)
My take: This study suggests that once daily dosing can be as effective as twice daily dosing. It may be that the total dose administered may be more important than the frequency. More studies are needed to confirm these results.
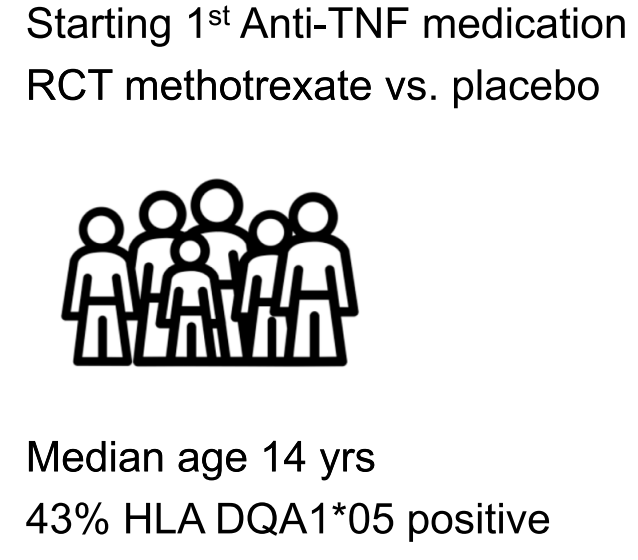
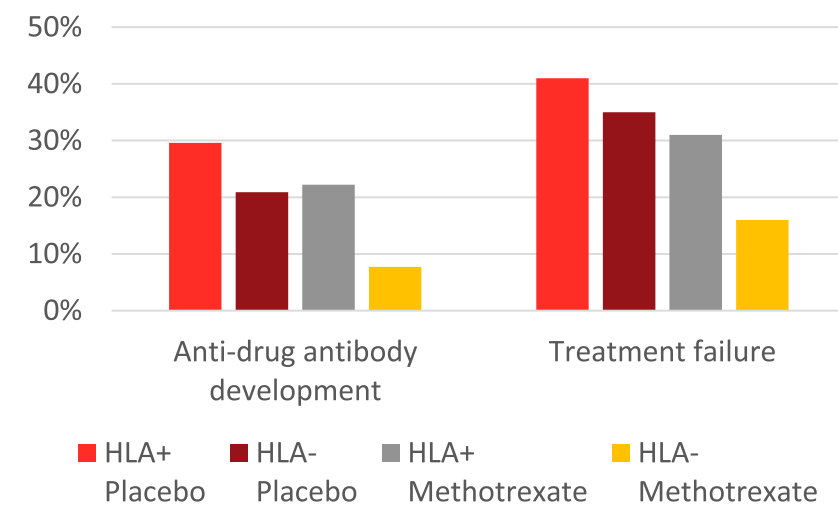
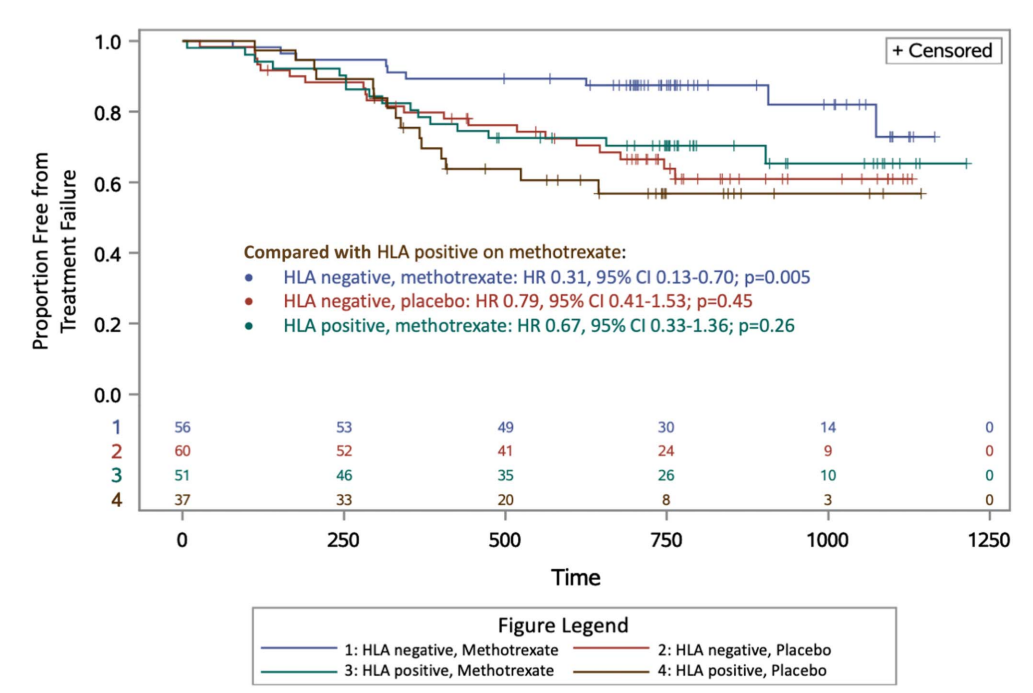
This was a prospective, double-blind, placebo-controlled trial with 204 patients examining the clinical outcomes of anti-TNF with or without methotrexate (COMBINE).
Key findings:
Treatment failure in HLA DQA1*O5: A trend toward increasedtreatment failure amongHLA DQA1*05-positive participantswas not statistically-significant (hazard ratio 1.58; P = 0.08).
HLA DQA1*05 and Treatment Failure Rate: During the followup period, HLA DQA1*05-positive patients had a 35% failure rate compared to 26% for those who were HLA DQA1*05-negative (P=0.098). The overall failure rate was 30%
Methotrexate Combined with HLA DQA1*05Effect: Patients who were HLA DQA1*05 negative and assigned to methotrexate experienced less treatment failures than HLA DQA1*05-positive patients on placebo (hazard ratio 0.31, 95% CI 0.13-0.70; P = 0.005).
Anti-TNF Medication Comparison: Treatment failure was similar between infliximab and adalimumab, 29% and 33% respectively
Antidrug antibodies (ADA): A trend toward increased ADA development among HLA DQA1*05-positive participants was not significant (odds ratio 1.96, P = 0.09). The addition of methotrexate to the treatment regimen mitigated the risk of treatment failure among individuals positive for HLA DQA1*05 and reduced the odds of developing ADA by 90%.
Rate of ADA: “After further stratification, HLA DQA1*05-negative participants assigned to methotrexate were less likely to develop ADA relative to HLA DQA1*05-positive patients on placebo (odds ratio 0.12; P = 0.008).”
Discussion Points:
“A retrospective by Fuentes-Valenzuela et al …found that if patients underwent proactive TDM, there was no increase in the rate of treatment discontinuation among those who were HLA DQ-A105 positive compared with HLA DQ-A105 negative”
“The totality of evidence suggests that HLA DQ-A1*05 seems to confer a risk of both immunogenicity and treatment failure, particularly among infliximab-treated patients. Furthermore, this risk may be mitigated by the use of proactive TDM and/or concomitant immunomodulators.”
My take (borrowed in part from authors): “40% of patients were HLA DQ-A1*05 positive, which was associated with a trend toward increased risk of both treatment failure and ADA. These risks were mitigated, but not eliminated, by adding oral methotrexate.” The use of combination therapy (methotrexate with anti-TNF) was associated with the lowest failure rates.
Recently Dr. Arun Singh gave our group a terrific update on Celiac Disease. I have taken some notes and shared some slides. There may be inadvertent omissions and mistakes in my notes.
Key points:
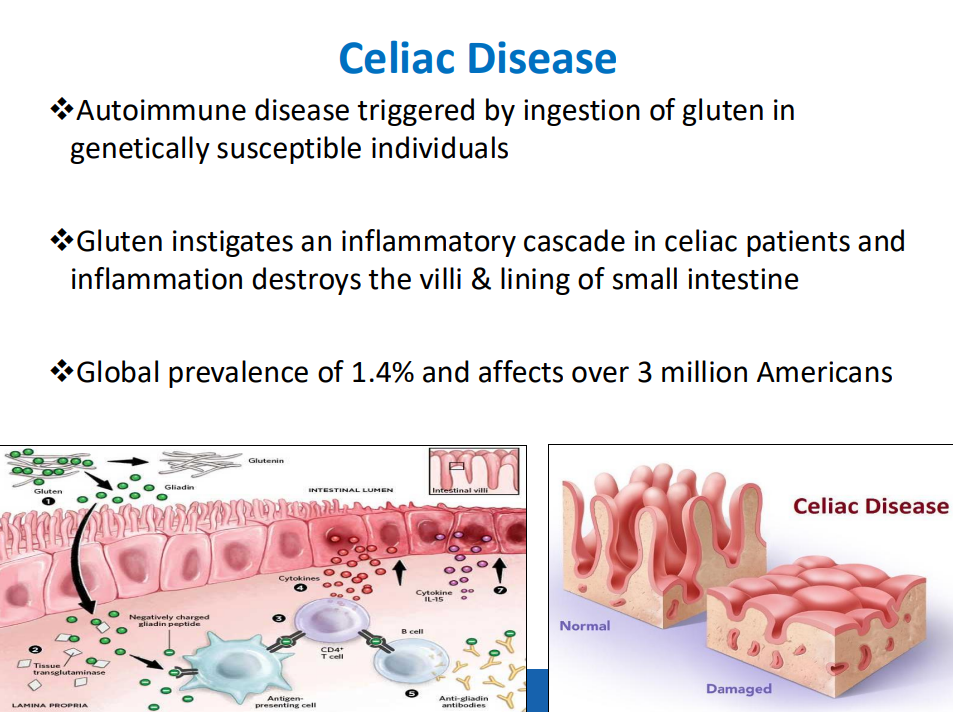
Celiac disease (CD) global prevalence is about 1.4%, though there are ‘pockets’ with much higher rates (~3% prevalence in Colorado). This equates to more than 3 million Americans with CD
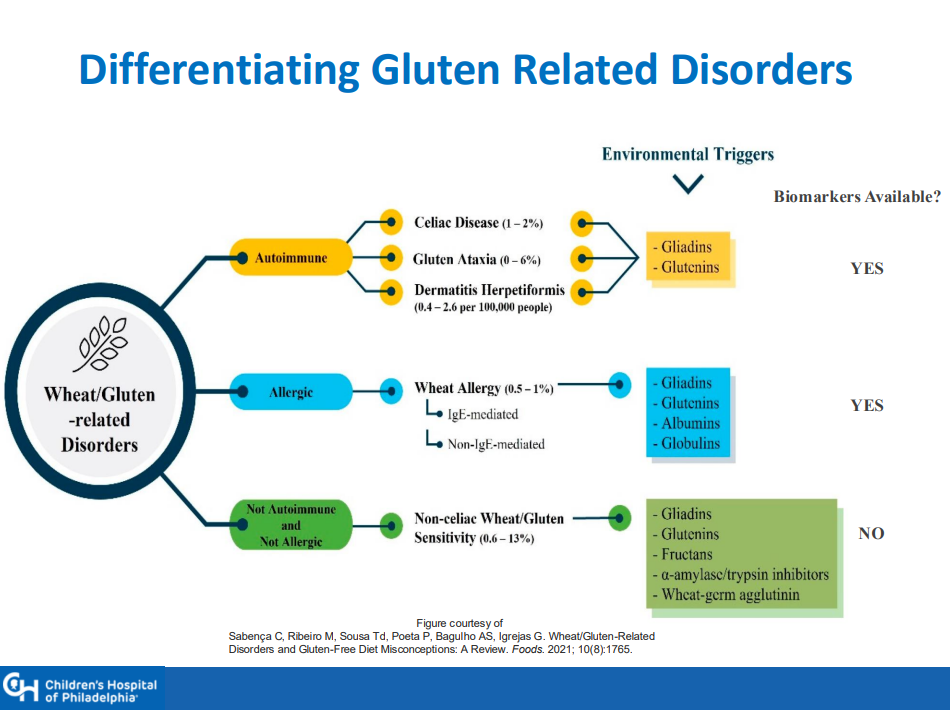
There is a huge gluten free diet market of ~$7 billion. This market includes CD, nonceliac gluten sensitivity (NCGS) and those with wheat allergies
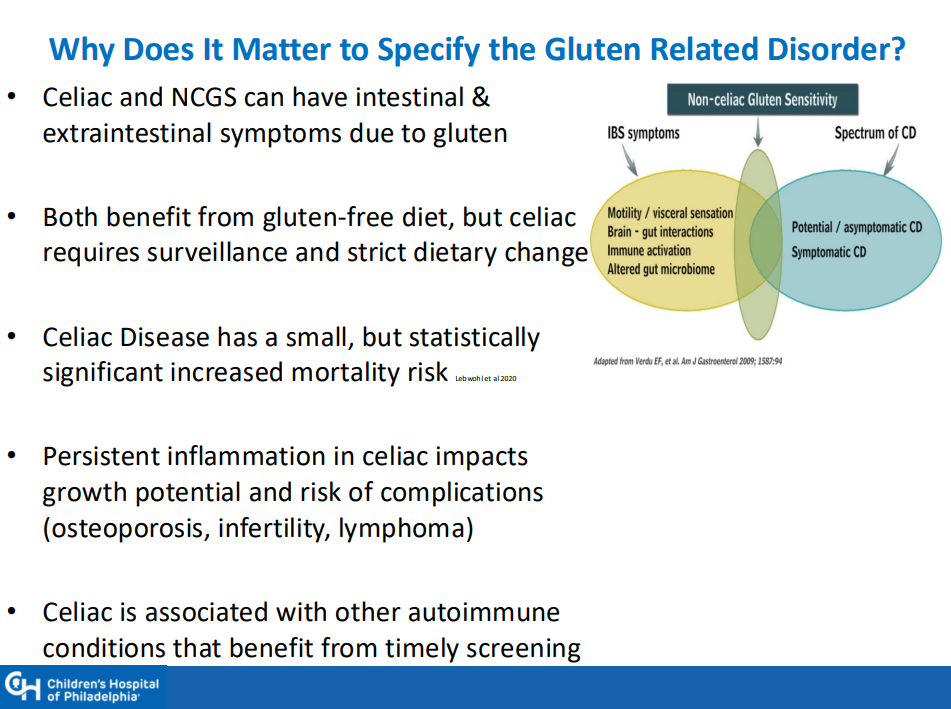
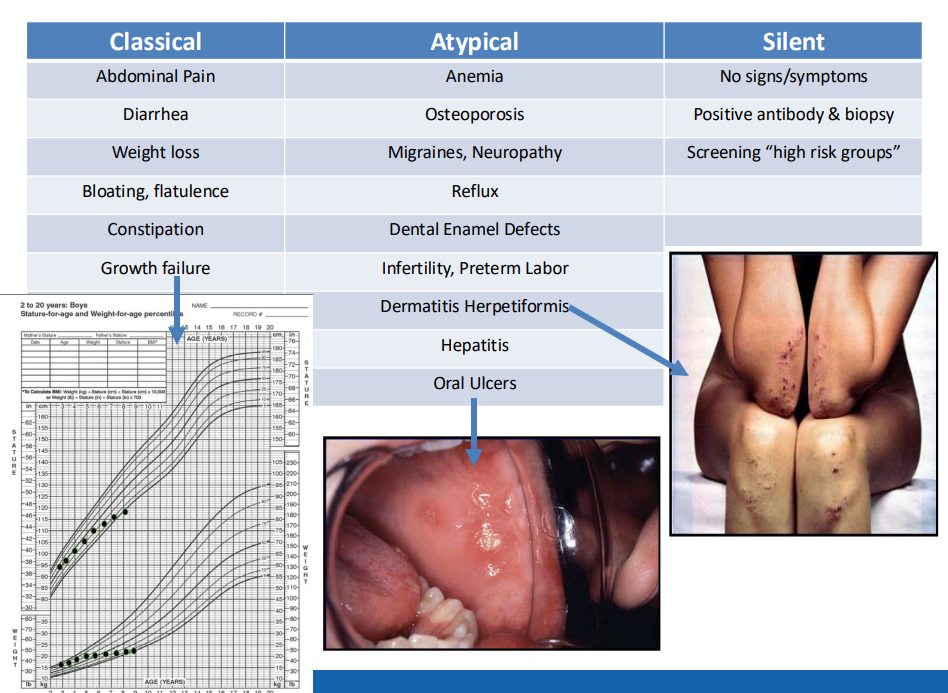
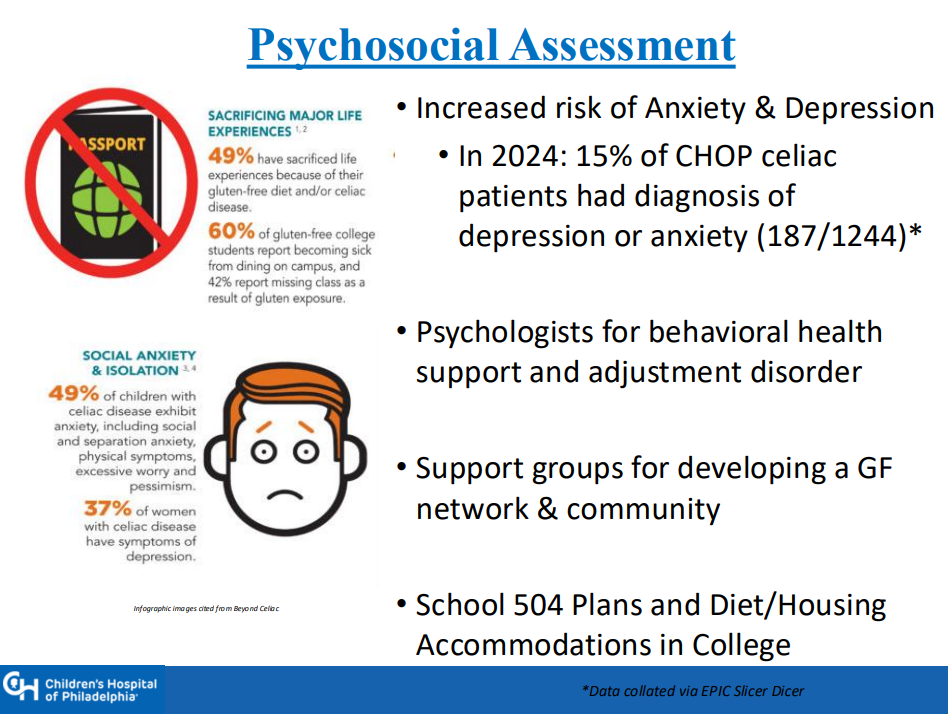
Many patients have atypical symptoms which can include ADHD, brain fog, headaches, and elevated LFTs. Many have silent CD with no symptoms
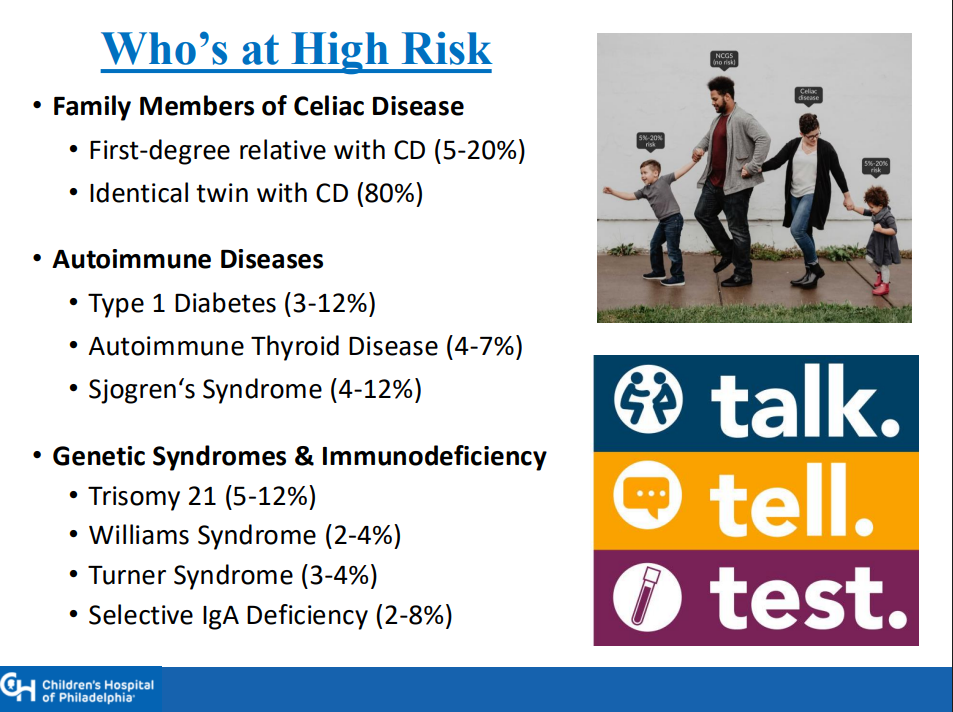
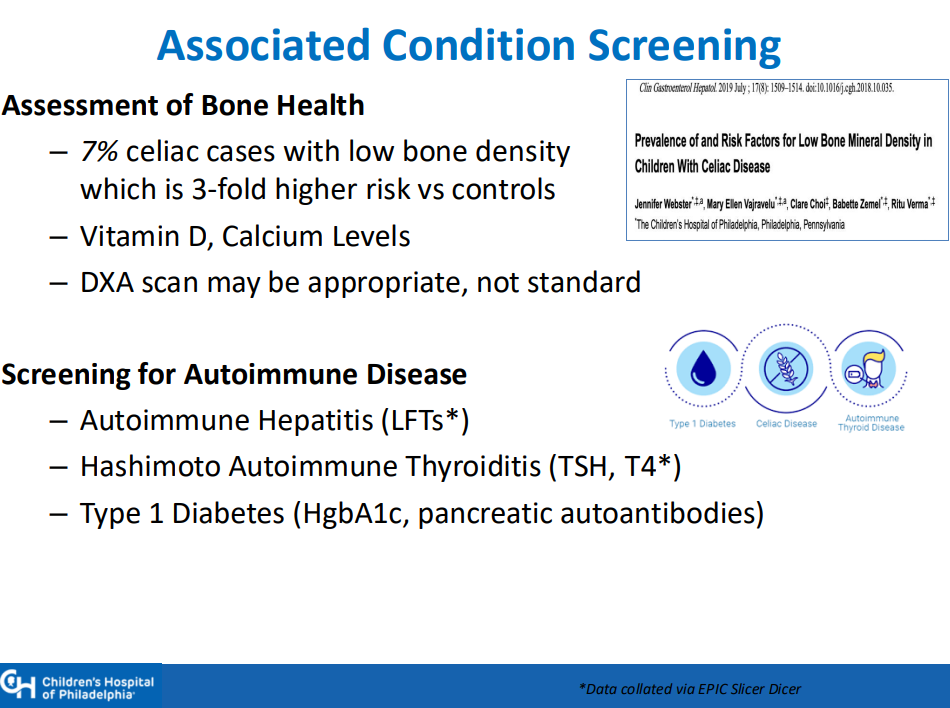
Higher risk groups include family members (~10% risk for 1st degree, ~80% risk for identical twin), autoimmune diseases (thyroid, diabetes, others), and genetic disorders (Down syndrome, Williams syndrome, Turner syndrome)
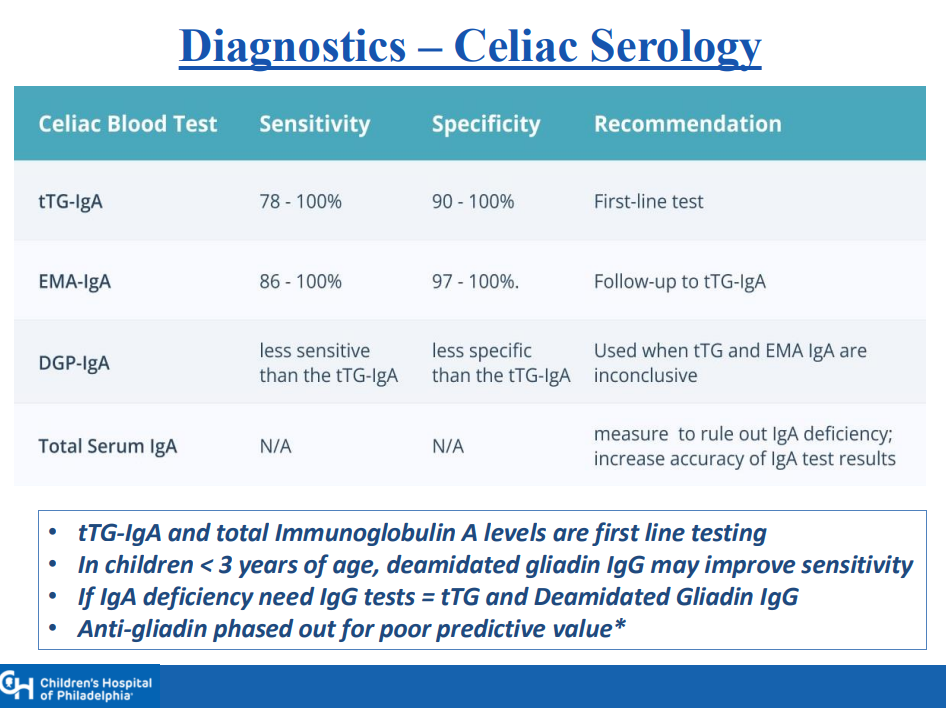
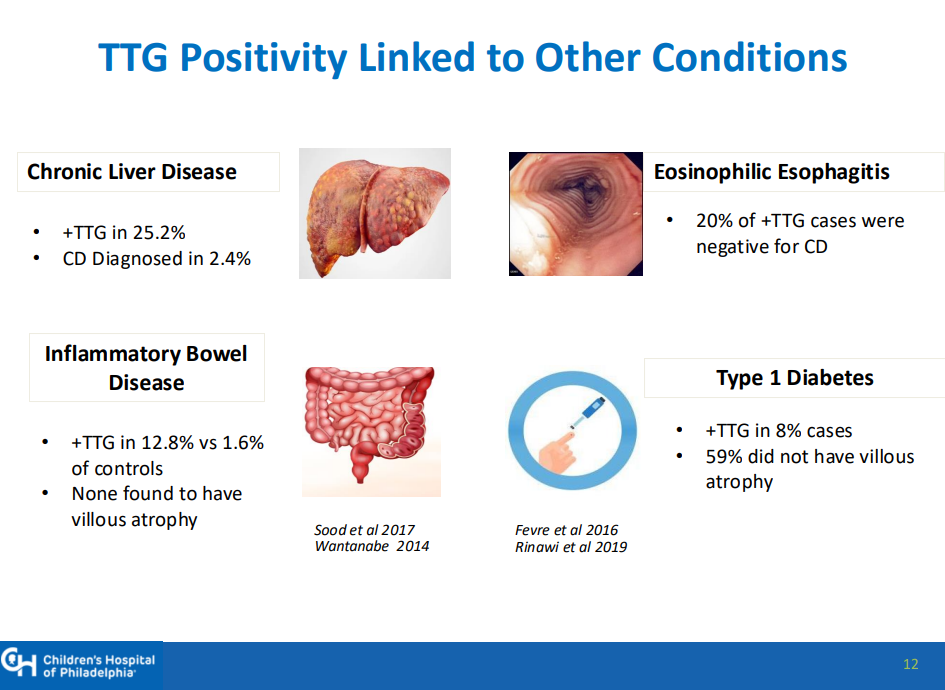
Transient elevation of TTG IgA is common. In TEDDY study, 19% had TTG IgA spontaneously normalize. Thus, a single abnormal lab is not reliable
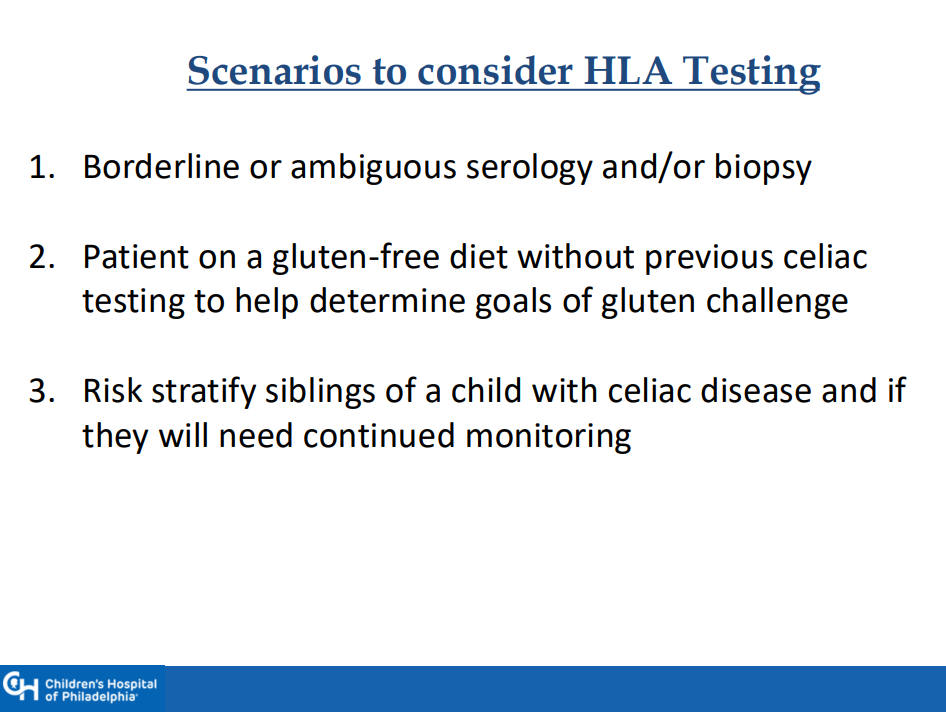
Genetic testing can be a useful adjunct in a few specific situations, including prior to instituting a gluten challenge
1-3% of those with celiac disease may be negative for HLA-DQ2 and HLA-DQ8
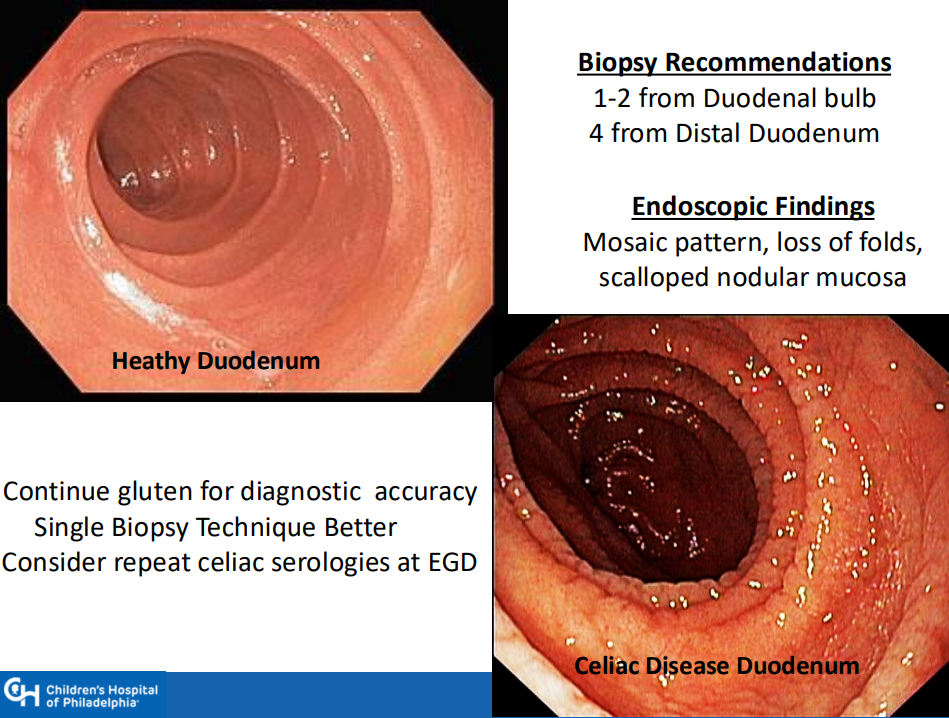
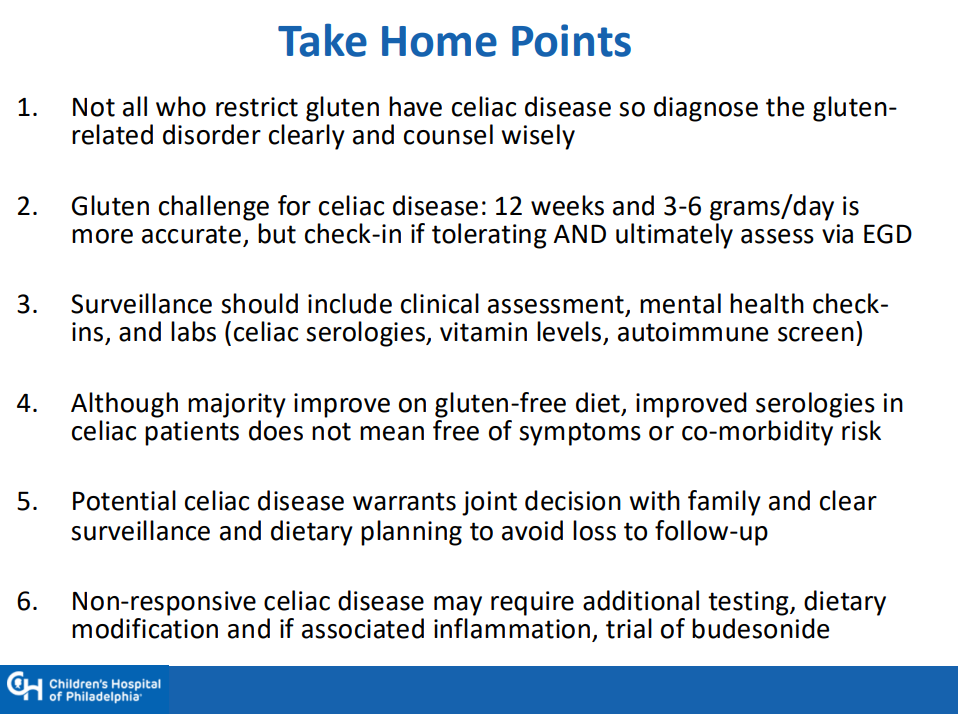
If a gluten challenge is needed, 12 weeks is ideal. However, if poorly tolerated, then consider endoscopy earlier and Dr. Singh recommends checking in with family 4-6 weeks into the challenge
Endoscopy recommendations: Taking a single biopsy per pass can improve orientation when obtaining duodenal biopsies (bulb and distal portion, 5-6 in total)
NASPGHAN has not updated comprehensive guidelines for CD in 20 years
A survey of NASPGHAN members indicated that ~40% utilize a “no-biopsy” approach in patients. Dr. Singh noted that the accuracy of this approach, based on data from North America, may be about 96%
Drug trials for CD require a biopsy-confirmed diagnosis
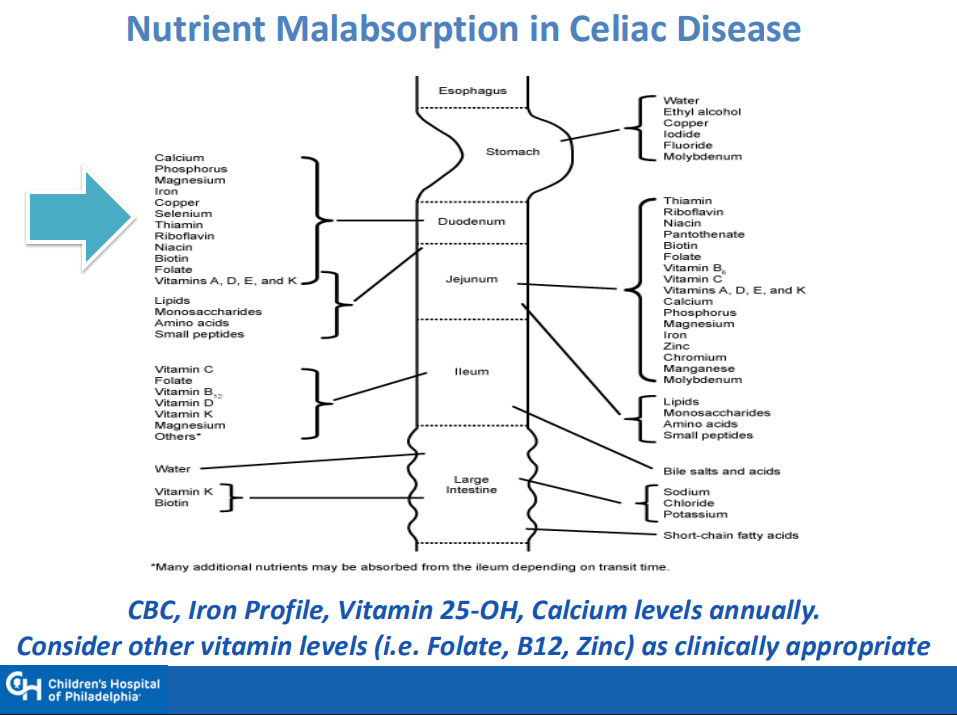
Surveillance practice is quite variable. Important to follow growth and serology. CHOP approach includes surveillance for type 1 DM
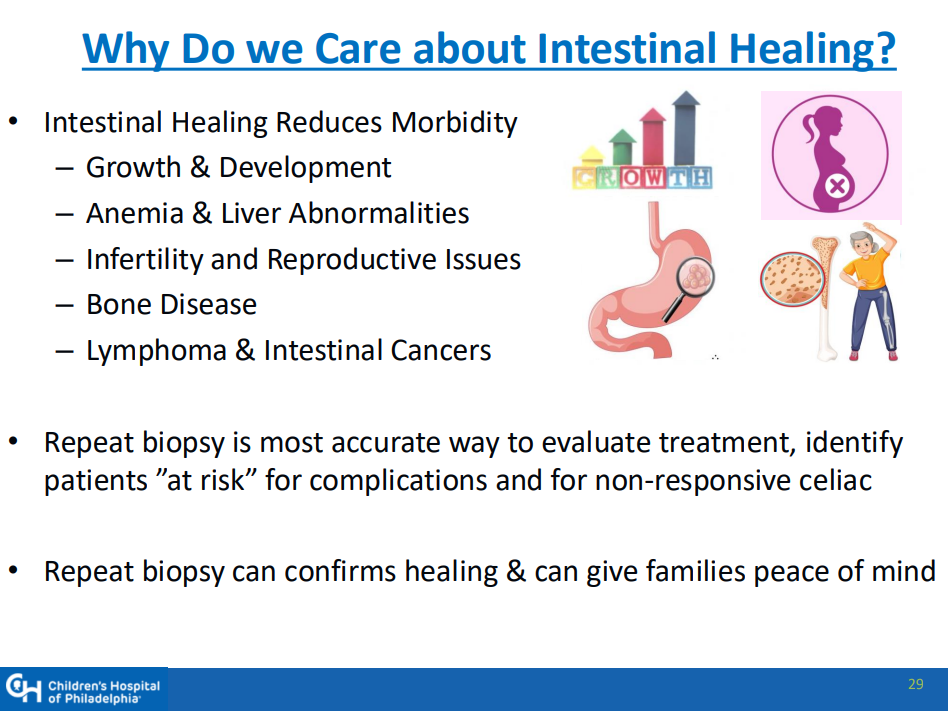
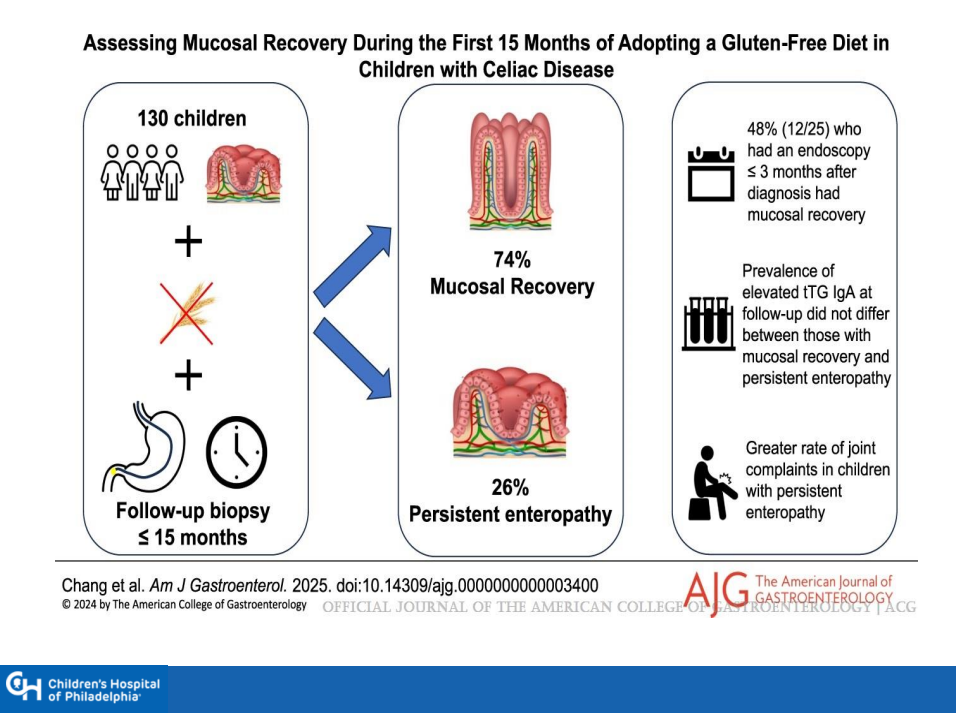
Followup endoscopy to assess mucosal healing is not the current standard of care but could be helpful in some patients
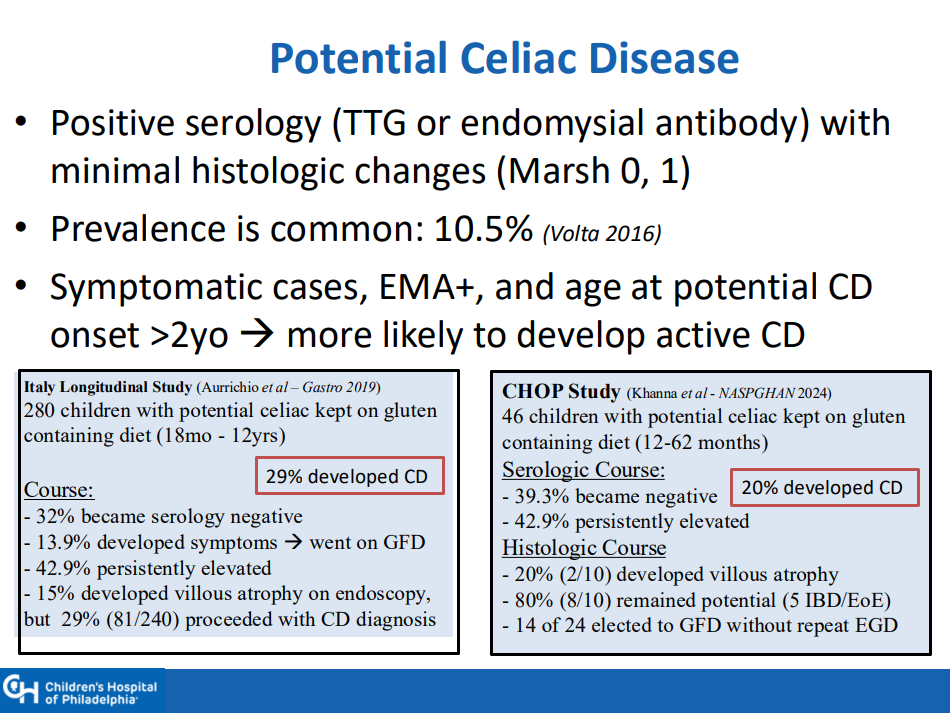
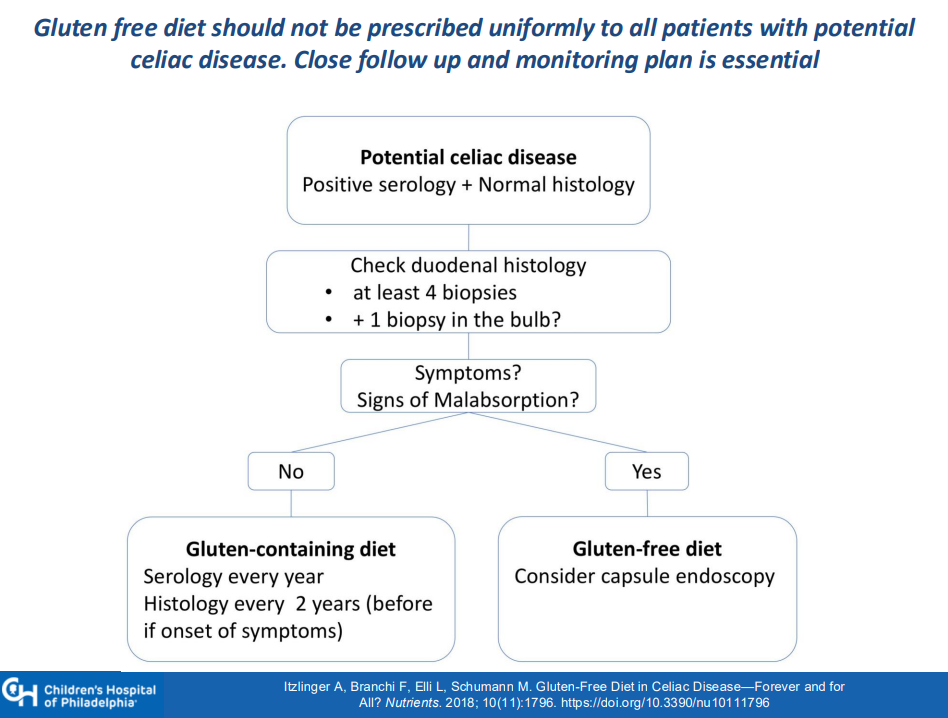
Among patients with potential CD, about 30% develop CD over time. Thus, these patients should be monitored (yearly labs, f/u scope after 2 years)
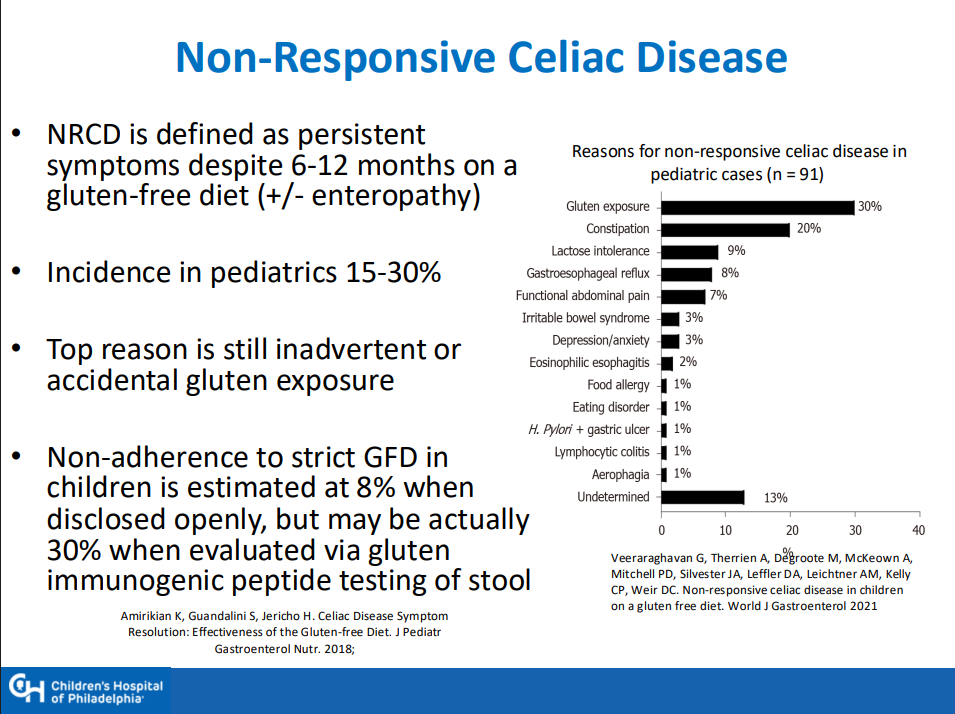
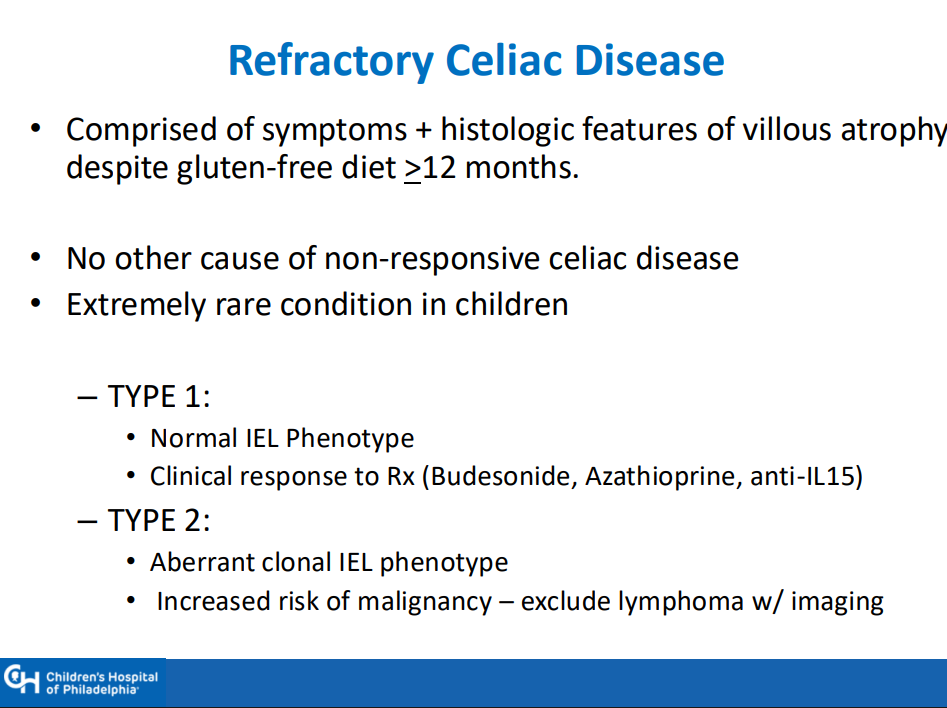
Nonresponsive/refractory CD: start with nutrition assessment, often needs a f/u scope before consideration of budesonide therapy (9 mg x 12 weeks) or gluten contamination elimination diet
UnitedHealth Group, the nation’s largest healthcare conglomerate, has secretly paid nursing homes thousands in bonuses to help slash hospital transfers for ailing residents – part of a series of cost-cutting tactics that has saved the company millions, but at times risked residents’ health, a Guardian investigation has found…
Those secret bonuses have been paid out as part of a UnitedHealth program that stations the company’s own medical teams in nursing homes and pushes them to cut care expenses for residents covered by the insurance giant.
In several cases identified by the Guardian, nursing home residents who needed immediate hospital care under the program failed to receive it, after interventions from UnitedHealth staffer…UnitedHealth said the suggestion that its employees have prevented hospital transfers “is verifiably false”. It said its bonus payments to nursing homes help prevent unnecessary hospitalizations that are costly and dangerous to patients and that its partnerships with nursing homes improve health outcomes…
To reduce residents’ hospital visits, UnitedHealth has offered nursing homes an array of financial sweeteners…
Two current and three former UnitedHealth nurse practitioners told the Guardian that UnitedHealth managers pressed nurse practitioners to persuade Medicare Advantage members to change their “code status” to DNR even when patients had clearly expressed a desire that all available treatments be used to keep them alive...
My take: Healthcare insurance companies are incentivized to act as financial institutions and gatekeepers/third party administrators. This often compromises and delays patient care.
This case report of four patients provides a good review of metastatic Crohn’s disease (MCD). MCD indicates that there is noncontiguous dermatological spread of CD involving the genitalia and perineum.
Key points:
“Less than 100 cases of pediatric MCD have been reported in the literature to date. These lesions are characterized by swelling, plaques, nodules, fissures, ulcerations, or crusts. In children, MCD typically presents as genital swelling with or without erythema in approximately 85% of cases.”
“Prior studies have shown that MCD co-occurs with CD in 50.8% of children, while others may develop GI symptoms after MCD diagnosis (15.3%) or even lack signs of CD (11.9%).”
“Scrotal histopathology revealed granulomatous inflammation, and genetic testing identified pathogenic variants in NOD2, COL7A1, and Chek2, as well as additional variants of uncertain significance.”
The optimal treatment is not clear. “Prior case reports and case series have shown positive responses to TNF-α inhibitors, but relapses may be common. Similarly, only partial improvement was noted in our patients treated with infliximab and adalimumab.”
Discussion: “Many patients do not demonstrate GI symptoms and may experience significant delays in diagnosis.”
My take: This article provides a good review of metastatic Crohn’s disease which is a rare problem. I have had two patients with this disorder. This problem fits the adage of “the more you see, the more you know; and, the more you know, the more you see.”
Background: “Caution regarding live vaccine administration emerged following reports of 5 fatal outcomes following the administration of the Bacille Calmette-Guérin vaccine in biologic-exposed infants.9 This has resulted in gastroenterology guidelines recommending that biologic-exposed infants should avoid live vaccines within the first 6 to 12 months of life or until drug concentrations are no longer detectable in the infant’s blood to reduce potential risks.2,10 [J Crohns Colitis. 2023; 17:1-27, Gastroenterology. 2021; 161:669-680.e0]. Contrary to this, inadvertent administration of the live oral rotavirus vaccine in biologic-exposed individuals has not been associated with significant adverse effects.7,11 Withholding the rotavirus vaccine has implications, given that rotavirus infection in infants is a leading cause of severe, dehydrating diarrhea in children under the age of 5 years globally.12,13“
This prospective cohort study enrolled 57 biologic-exposed infants, including infliximab (n = 21), adalimumab (n = 19), vedolizumab (n = 10), and ustekinumab (n = 7), in the third trimester.
Key findings:
Immunologic assessments validated for age were normal in all infants despite median infliximab concentrations of 6.1 ug/mL, adalimumab concentrations of 1.7 ug/mL, ustekinumab concentrations of 0.6 ug/mL, and undetectable for vedolizumab at median of 10.7 weeks of age
The live oral rotavirus vaccine series was provided to 50 infants with the first dose given at a median of 13 weeks of age. No adverse effects following immunization were reported
Discussion:
“Administration of the live rotavirus vaccine appeared low-risk in biologic-exposed infants born to mothers with IBD”
“Routine drug concentration testing in the infant should not be utilized to determine the safety of live rotavirus vaccination”
“Physicians should advise patients to ‘be more concerned about active disease rather than active medications’ and to continue effective therapy through pregnancy and lactation”
My take: Given the difficulty in excluding rare adverse outcomes, it is unlikely that formal vaccine recommendations will change in infants exposed to biologics; however, inadvertent administration of a live oral rotavirus vaccine poses a very lowl risk based on current studies.
Floating flowers -seen in several places in Thailand
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.